|
Abstract
Carcinoid tumors are relatively rare and can occur in the thorax, abdomen, or pelvis. Functional imaging in the form of Indium-111 pentetreotide scanning is widely used for identification of these tumors and it exploits the fact that the vast majority of these tumors express somatostatin receptors on their cell membrane. In this report, we present a case of a 76-year-old man who was diagnosed with peritoneal carcinomatosis. The findings of the initial imaging made by planar and single photon emission computed tomography were misleading and the actual diagnosis was only made by single photon emission computed tomography/computed tomography.
Keywords: Neuroendocrine Tumor; 111In-Pentetreotide; OctreoScan; SPECT CT.
Introduction
Since the success of hybrid imaging modality with positron emission tomography (PET) and computed tomography (CT), different combination of radiological and nuclear medical imaging systems have been developed such as single photon emission computed tomography (SPECT) with CT, PET with magnetic resonance imaging (MRI). The addition of CT to the SPECT study aims to increase the sensitivity and improve localization of lesions and metastasis in cases of cancer. We describe a case of advanced peritoneal carcinomatosis in the form of omental cake that was missed in the annual follow up by 111In-pentereotide scan in which planar and SPECT imaging was only performed. The diagnosis was made in the third annual follow up with OctreoScan which was performed as SPECT CT study. This highlights the potential risk of misdiagnosis based on 111In-pentetreotide planar or SPECT scan alone without the correlation with anatomical cross sectional imaging.
Case Report
A 76 years old man was diagnosed to have small bowel carcinoid in 2007 with a positive 111In-pentetreotide scan. He was subsequently treated with surgical resection later in that year. Regional nodes were found to be positive with metastases. Post-operative 111In-pentetreotide scan (planar and SPECT imaging) showed only physiological uptake with no somatostatin receptor avid lesions found. Follow-up CT in 2010 showed residual small mesenteric nodes and few liver lesions. 111In-pentetreotide scan (planar and SPECT imaging) did not show active disease.
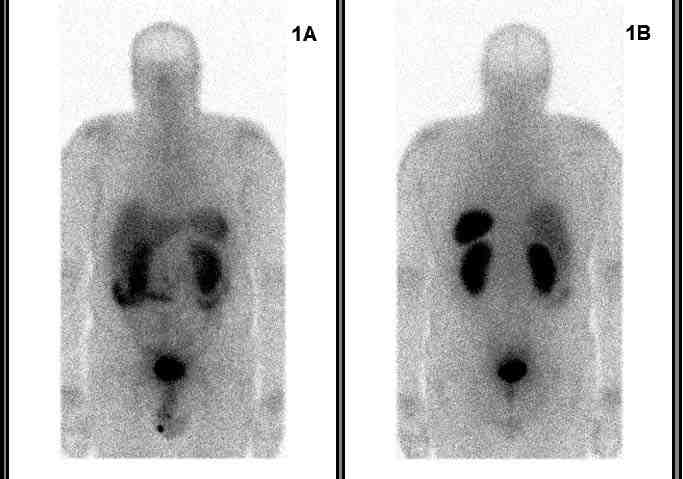 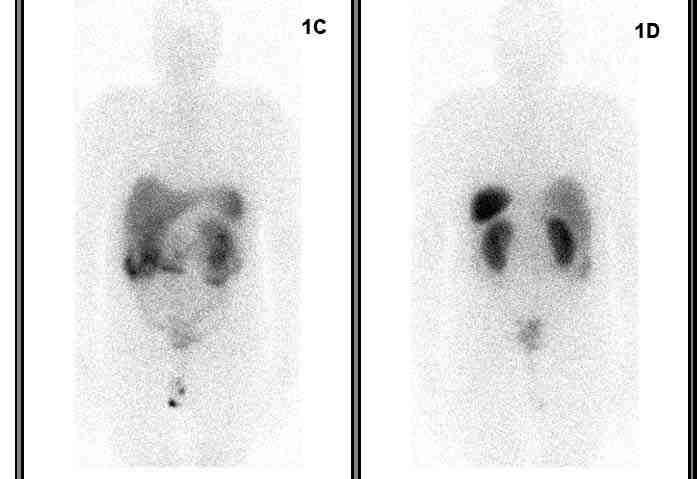
Figure1: 111In-pentetroetide planar images from vertex to mid thighs. 1A & 1B: Anterior and posterior images at 4 hours post tracer administration demonstrate linear uptake in both sides of mid-abdomen which may suggest bowel activity. Physiological uptake is also noted in the liver, spleen and kidneys; 1C & 1D show persistent linear uptake in the mid abdomen.
Follow-up 111In-pentetreotide scans in 2011 and 2012 (Fig. 1), showed a linear heterogeneous tracer activity seen in the mid abdomen; it was initially assumed to be physiological bowel uptake, but on the SPECT CT imaging, the tracer activity co-register to the soft tissue opacities seen in the omentum on the CT images (Fig. 2). The appearance would be consistent with somatostatin receptor avid omental disease/cake.
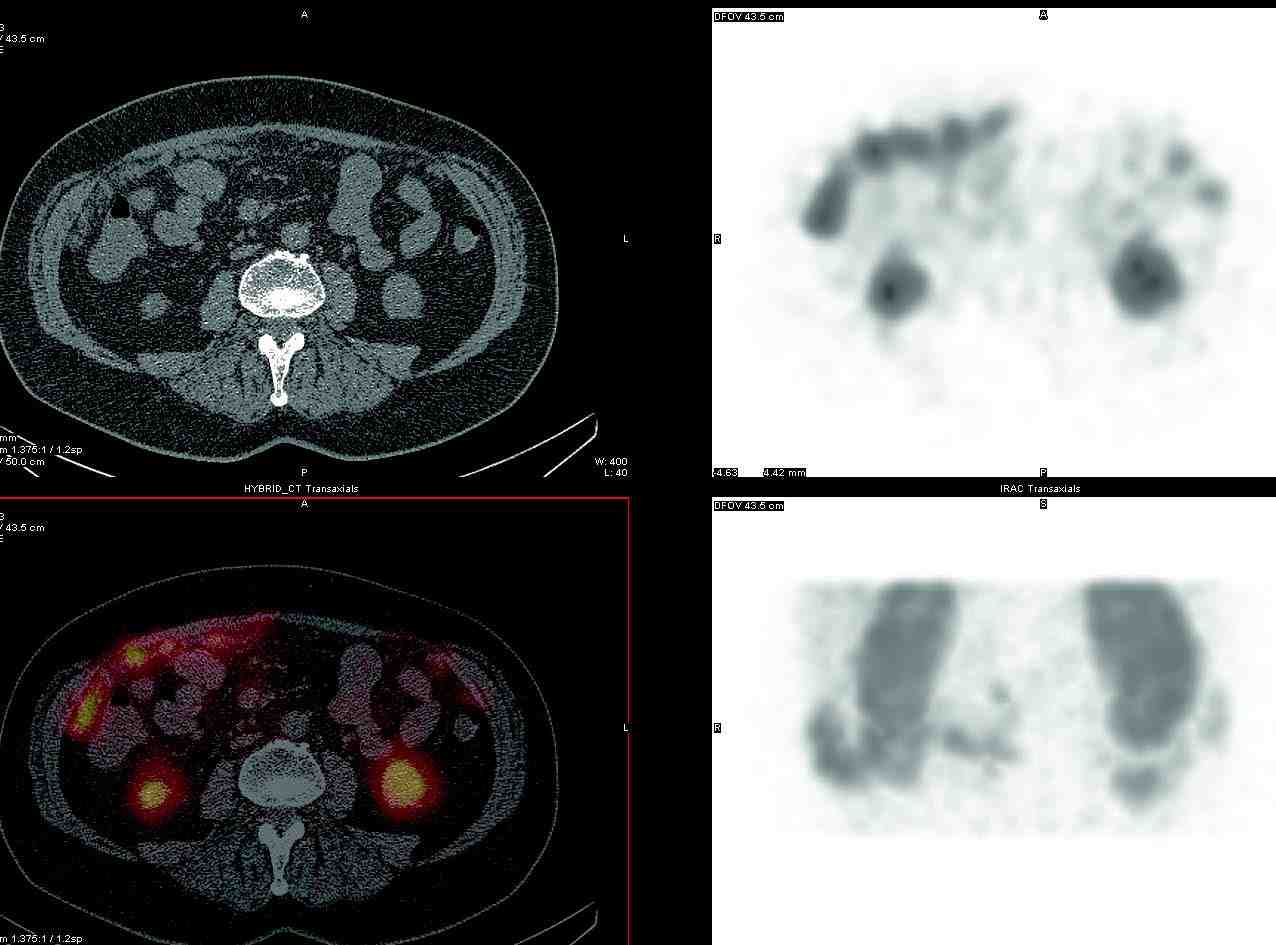 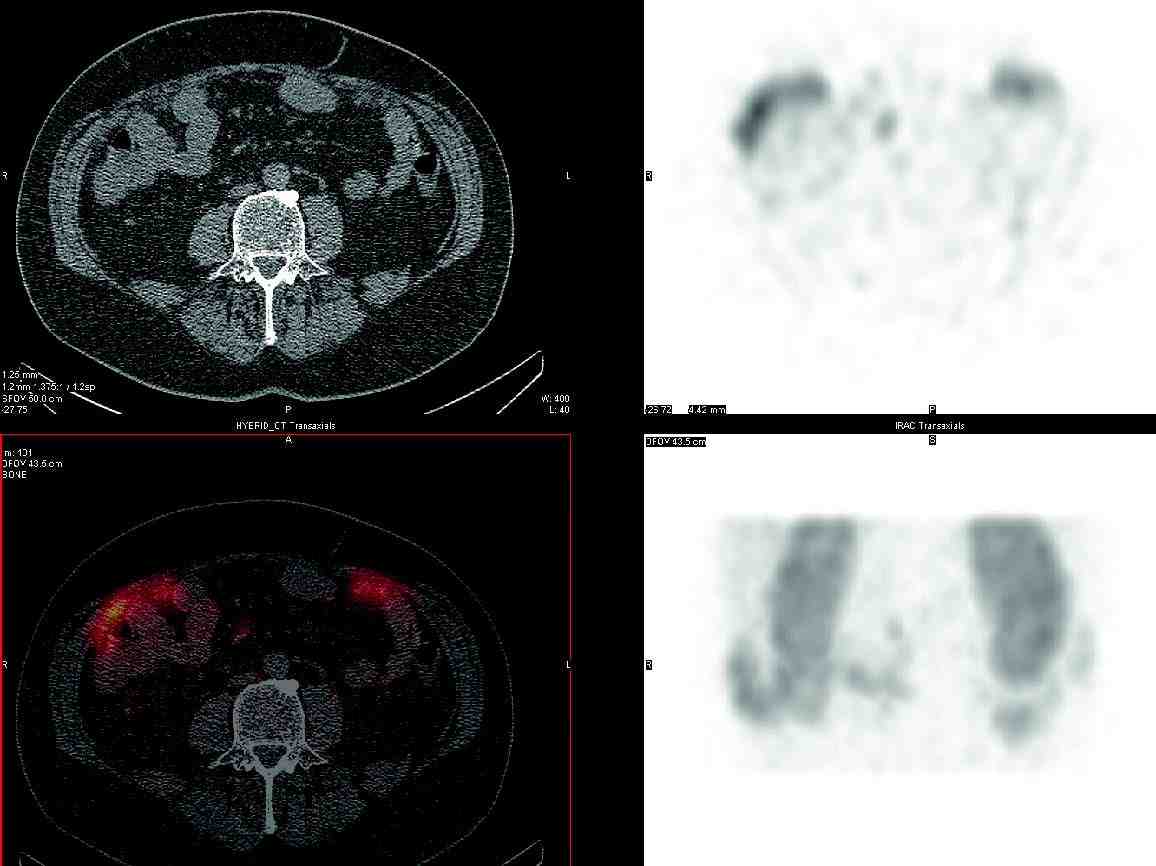
Figure 2 and 3: Axial sections from SPECT CT scan done 24 hours post tracer administration. Both figures show the high tracer uptake along the anterior abdomen corresponding to the several omental deposits seen in this area. No abnormal tracer uptake was identified in the patient’s bowel and the finding is consistent with omental carcinomatosis.
Discussion
The classical finding of a carcinoid is a stellate soft tissue mass with radiating pattern and beading of mesenteric neurovascular bundles, commonly described as desmoplastic reaction. Peritoneal carcinomatosis arising from neuroendocrine tumor is not common1; within this group of tumors, carcinoid is the most common neuroendocrine tumor with this presentation with a prevalence of 13%.2
It was found that neuroendocrine tumors have an increased number of somatostatin receptors, as compared to normal tissues. At present time, there are five known subtypes.3 Somatostatin receptor scintigraphy with 111In-pentetreotide (OctreoScan) binds to two of these subtypes and is effective in visualizing neuroendocrine tumors, and its metastasis with an overall diagnostic sensitivity of 70% to 90%.4,5 It is considerably more sensitive than conventional anatomic imaging. Its usage in neuroendocrine tumors not only includes assessment of disease extent, but also in identified primary lesion, assesses treatment response, and selection of patients for radionuclide therapy. Physiological uptake of this tracer can be seen in pituitary gland, thyroid gland, liver, spleen, urinary tract, bowel and gallbladder.6 Planar or SPECT alone might not be able to differentiate physiological uptake in some of these organs from metastatic disease. The most common pitfall is on the uptake from the metastatic mesentery lymph nodes which is misinterpreted as physiological small bowel uptake. Another example includes liver metastasis which are misinterpreted as physiological gallbladder uptake.7 One study has found that SPECT CT affected the diagnostic interpretation of somatostatin receptor scintigraphy in 32% of the patients and induced changes in management in 14% of the patients.8
In this case, the assumption of bowel uptake was made in 2011 on his annual 111In-pentetreotide study. At that time, SPECT CT was not available at our institution. Routine contrast enhanced CT was not carried out as the patient did not have any symptoms. In the subsequent year, he was imaged with SPECT CT machine and the diagnosis was made. The overall distribution of tracer uptake seen on SPECT between 2011 and 2012 has not changed significantly. The patient was subsequently treated with chemotherapy.
Conclusion
This case has challenged the imaging findings which are based on the SPECT study alone and it has highlighted the importance of anatomical correlation. Hybrid imaging by adding CT scan to the already acquired SPECT images has improved diagnosis, localization of lesions and subsequent follow up. SPECT CT has found its place in several other areas like parathyroid scintigraphy, thyroid cancer scintigraphy, bone scans and sentinel lymph nodes localization amongst others.
Acknowledgements
The author reported no conflict of interest and no funding was received on this work.
References
1. Modlin IM, Oberg K, Chung DC, Jensen RT, de Herder WW, Thakker RV, et al. Gastroenteropancreatic neuroendocrine tumours. Lancet Oncol 2008 Jan;9(1):61-72.
2. Modlin IM, Lye KD, Kidd M. A 5-decade analysis of 13,715 carcinoid tumors. Cancer 2003 Feb;97(4):934-959.
3. Ulrich CD II, Holtmann M, Miller LJ. Secretin and vasoactive intestinal peptide receptors: members of a unique family of G protein-coupled receptors. Gastroenterology 1998 Feb;114(2):382-397.
4. Oberg K. Carcinoid tumors, carcinoid syndrome, and related disorders. In: Larsen PR, Kronenberg HM, Melmed S, Plansky KS, eds. Williams textbook of endocrinology. 10th ed. Philadelphia, Pa: Saunders, 2003; 661-690.
5. Reidy-Lagunes DL, Gollub MJ, Saltz LB. Addition of octreotide functional imaging to cross-sectional computed tomography or magnetic resonance imaging for the detection of neuroendocrine tumors: added value or an anachronism? J Clin Oncol 2011 Jan;29(3):e74-e75.
6. Kwekkeboom DJ, Kam BL, van Essen M, Teunissen JJ, van Eijck CH, Valkema R, et al. Somatostatin-receptor-based imaging and therapy of gastroenteropancreatic neuroendocrine tumors. Endocr Relat Cancer 2010 Mar;17(1):R53-R73.
7. Intenzo CM, Jabbour S, Lin HC, Miller JL, Kim SM, Capuzzi DM, et al. Scintigraphic imaging of body neuroendocrine tumors. Radiographics 2007 Sep-Oct;27(5):1355-1369.
8. Krausz Y, Keidar Z, Kogan I, Even-Sapir E, Bar-Shalom R, Engel A, et al. SPECT/CT hybrid imaging with 111In-pentetreotide in assessment of neuroendocrine tumours. Clin Endocrinol (Oxf) 2003 Nov;59(5):565-573.
|