|
Abstract
Objective: To illustrate the patient safety culture in Oman as gleaned via 12 indices of patient safety culture derived from the Hospital Survey on Patient Safety Culture (HSPSC) and to compare the average positive response rates in patient safety culture between Oman and the USA, Taiwan, and Lebanon.
Methods: This was a cross-sectional research study employed to gauge the performance of HSPSC safety indices among health workers representing five secondary and tertiary care hospitals in the northern region of Oman. The participants (n=398) represented different professional designations of hospital staff. Analyses were performed using univariate statistics.
Results: The overall average positive response rate for the 12 patient safety culture dimensions of the HSPSC survey in Oman was 58%. The indices from HSPSC that were endorsed the highest included ‘organizational learning and continuous improvement’ while conversely, ‘non-punitive response to errors’ was ranked the least. There were no significant differences in average positive response rates between Oman and the United States (58% vs. 61%; p=0.666), Taiwan (58% vs. 64%; p=0.386), and Lebanon (58% vs. 61%; p=0.666).
Conclusion: This study provides the first empirical study on patient safety culture in Oman which is similar to those rates reported elsewhere. It highlights the specific strengths and weaknesses which may stem from the specific milieu prevailing in Oman.
Keywords: Patient safety; Organizational culture; Hospital administration; Health care surveys; Oman.
Introduction
At an age when humanism is often perceived to pervade in all spheres of life, where doctors are accepted to be abreast with the Hippocratic oath, ‘do no harm’ and health care settings are often scrutinized for accreditation, the issue of safety has come to the forefront for both healthcare planners, stakeholders and healthcare workers alike. For the health planner, safety measures represent the desirable quest to acquire a reputable quality health care system. In some instances, this has a direct bearing on accreditation.1 For the healthcare workers, lack of vigilance about safety may result in jeopardizing their own career, as well as the risk of exposing themselves to unintended occupational hazards. From such discussions, the relevant issue is safety culture.
The concept of safety culture has been variously conceptualized. Cox and Cox2 have operationalized safety culture as the anthology of “attitudes, beliefs, perceptions, and values that employees share in relation to safety”. Neva & Sorra3 have perceived safety culture as a pro-social behavior that has direct bearing on safety measures practiced in organizational settings. The U.K. Health and Safety Commission have defined safety culture as an amalgamation of ‘individual and group values, attitudes, perceptions, competencies, and patterns of behavior that determine the commitment to, and the style and proficiency of, an organization’s health and safety management.”4
The most important aspect of patient safety culture is its applicability within healthcare settings. The entrance of ‘culture’ in patient safety came into prominence within the background that ‘that the majority of errors and adverse events more accurately stem from a complex chain of events that jointly contribute to the cause rather than human errors,”5 and therefore gestalt phenomena appears to be at work in that the ‘whole is greater than the sum of the parts’.
In recognizing that culture has direct bearing on organizational functions, patient safety culture has come to prominence with a plethora of studies that have documented patient safety culture in many parts of the world.6-14 Such an undertaking has been essential for auditing the integrity of health systems, and for providing a venue for further improvement in addition to fulfilling benchmarks relevant to accreditation and quality assurance. While there is a plethora of studies on patient safety, most of them have employed measurements that have no heuristic value for international comparison. On this ground, there is a need to identify instruments or a set of benchmarks that could capture variations of patient safety culture in different countries as well as having potential for instituting baseline assessment.15,16 From available literature, one instrument is increasingly becoming sine non qua for surveying patients, that is the Hospital Survey on Patient Safety Culture (HSPSC), developed by the Agency for Healthcare Research and Quality.17 HSPSC is a portable, easy-to-use measure of 12 composites of culture pertaining to safety in an organizational setting. The available evidence does suggest that it applies to different populations with adequate psychometric properties.6-15
While many regions of the World have documented patient safety culture,6-15 there is a dearth of such undertakings from Arabic speaking countries with a few exceptions. With increasing globalization and being custodians of most of the hydrocarbon, many Arabic speaking countries, despite being characterized with seismic political and social predicaments, have grown to be a ‘hub’ of globalization. Studies on patient safety culture are therefore imperative. In the available literature, four studies have emerged from Saudi Arabia on patient safety. Most of these studies were limited by the fact that the studies have focused on quantification of patient safety culture in a single institution,18 region 5 or simply have employed instruments that hamper international comparison.19,20 Other Arabic speaking countries have documented some veneer of patient safety culture but these studies appear to suffer similar misgivings as those emanating from Saudi Arabia.21-25 However, El-Jardali and his colleagues15 in Lebanon have examined patient safety using criteria suitable for international comparison. More studies are needed to chart patient safety culture in other Arabic speaking countries and international comparison would be an added asset.
Oman represents a fertile ground for exploring patient safety culture for various reasons. Firstly, no such studies have been undertaken on patient safety. Its healthcare system has recently been lauded as one of the most efficient in the world according to the World Health Organization but little is known about how such attributes translate into safety culture. Secondly, Oman has attracted a cadre of health care workers from different parts of the world. It remains to be seen how people from different backgrounds would fare on the indices of safety culture. Lastly, Oman has spent a very small fraction of its GNP on health care services26 and it remains to be seen how such a meager investment fosters safety culture. The aim of this study is twofold. The first is to illustrate the patient safety culture in Oman as gleaned via the Hospital Survey on Patient Safety Culture.17 Related to this, the second aim is to compare the average positive response rates in patient safety culture between different countries (USA, Lebanon and Taiwan), and therefore the situation in Oman could be reflected in terms of contrast to other parts of the world. There is rationale for selecting these studies. Apart from being divergent in term of geographic locations, these countries are socio-culturally different from each other though there might be parallel subterranean themes. Lebanon is an Arabic country but with different socio-cultural constitution compared to Oman. USA, with a global outlook and being arguably the most advanced country in the world, provides a benchmark for comparison within the background that HSPSC is ‘made in the USA’. On the other hand, Taiwan is one of the Asian Tiger economies with a cultural background that is predominantly Confucius in nature while that of the USA is secular. Oman is Islamic but adheres to the Ibadism sect while Lebanon has diverse religious denominations.
Methods
The target population was health care and allied health care professional staff working in different government hospitals in Oman. Out of eight regional hospitals under the umbrella of the Ministry of Health of Oman, the five hospitals in northern Oman were selected because of logistic region. The north of Oman is separated from the south by mainly desert.
A simple random sampling scheme was given to an administrator of each hospital to be used to select 10% of the staff. The selected were then contacted by a member of the research team. No attempt was made to select by quota based of work type. Unsurprisingly, the results showed the highest proportional representation for the largest groups in a hospital, nurses and doctors. Of the 400 hospital employees selected and invited to participate 390 participants responded, resulting in a response rate of (98%).
The Hospital Survey on Patient Safety Culture developed by the Agency for Healthcare Research and Quality.17 was used to quantify the patient safety culture in Oman. As alluded above, HSPSC has been shown to be acceptable in many cross-cultural samples12,13 including the Arab World.15,22,27 Some studies have also found that HSPSC is not biased towards false positives.6
Oman health care services are manned by health professionals from different parts of the World and therefore English is the ‘lingua Franca’ for healthcare communities though those who communicate with patients are required to be well-versed in the local language, Arabic. As a result of such an amalgamation of different cultural and linguistic groups, medical education in Oman, including training of physicians, nurses and technical staff, is in English. On this ground, the English version of the HSPSC was employed. Since the aim of the present study was to compare its performance in Oman with other populations, it was deemed essential that it should be conducted in its original language, English. During preparation for the study, research assistants were trained to decode any misunderstanding of the items of the HSPSC instrument.
Once a brief explanation of the study was given and participants were assured that all data would be confidential, informed consent was obtained from participants. The instrument, HSPSC, was administered to the health workers during working hours. It was explicitly stated that their responses would have no influence on their professional development in the hospital. To avoid peer influence, the participants were asked not to discuss the questionnaire with each other. Ethical approval for this study was obtained from the Institutional Review Board of the Ministry of Health.
The protocol for establishing psychometric property of HSPSC has been detailed elsewhere.15 Internal consistency of the instrument was measured by calculating the Cronbach’s coefficient for the 12 composites of HSPSC. As shown in Table 1, the above value, ranging from 0.41 to 0.78, appears to fall within the expected range that has been reported in earlier studies.15,17 Being a protean concept without central features, it should be expected that the value could dip much lower. Therefore, as noted elsewhere,13 the Hospital Survey on Patient Safety Culture appears to have adequate internal consistency and reliability.
Table 1: Cronbach’s alpha and distribution of positive responses for survey composites.
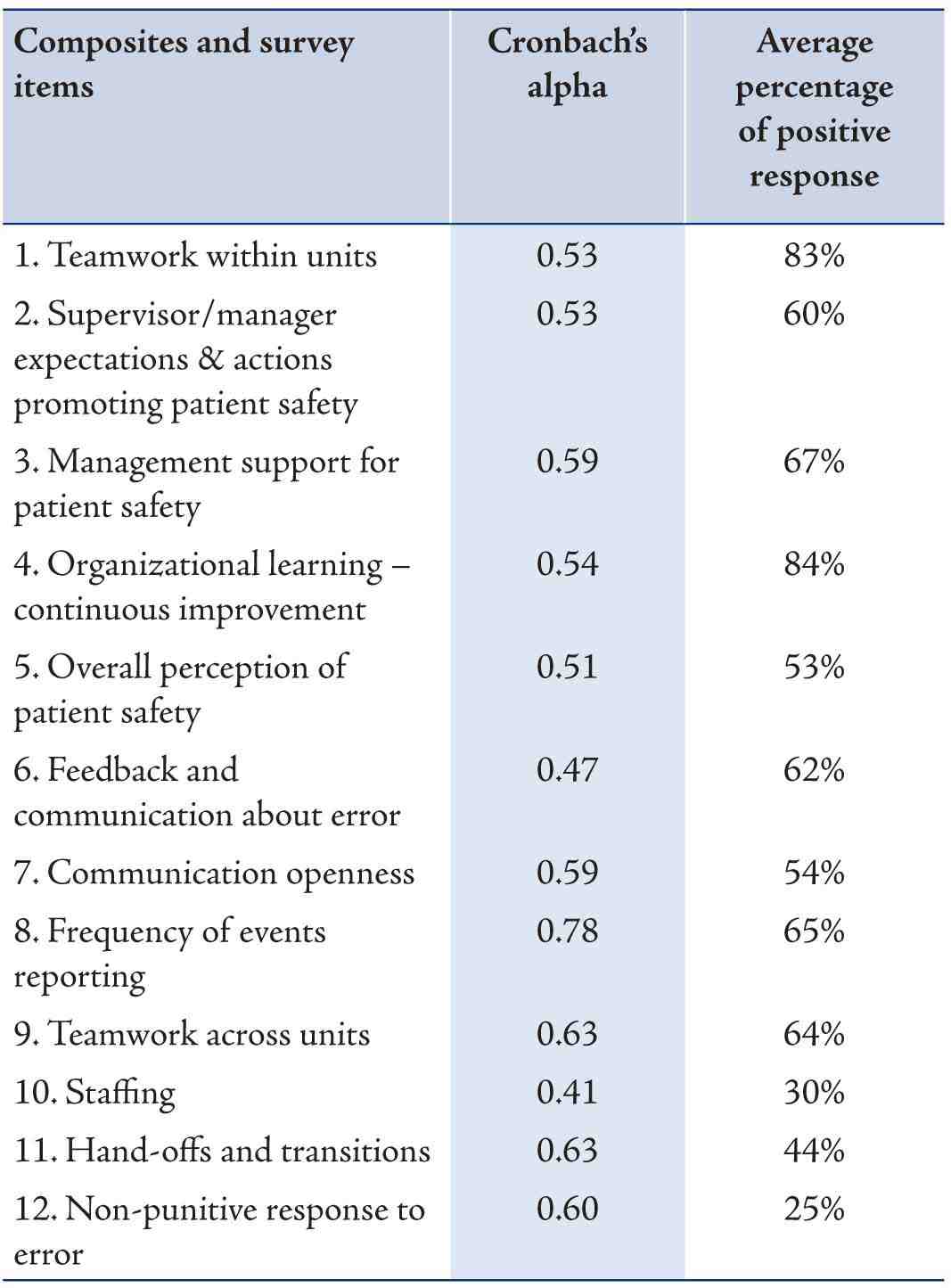
1The composite-level percentage of positive responses were calculated using the following formula: [number of positive responses to the items in the composite/total number of responses to the items (positive, neutral and negative) in the composite (excluding missing Responses)
Descriptive statistics were used to describe the data. For categorical variables, frequencies and percentages were reported. Differences between groups were analyzed using Pearson’s chi-squared tests (or Fisher’s exact tests for cells less than 5). Differences between groups were analyzed using Student’s t-test or Kruskal-Wallis Test, wherever appropriate. An a priori significance level was set at 0.05. Statistical analyses were performed using version 12.1 of Stata, (StataCorp, College Station, TX, USA).
Results
The overall mean positive response rate in Oman was 58%. Table 2 describes the demographic characteristics of the participants from Oman. There were significant differences among the 5 care hospitals (p<0.001). Al-Nahdha hospital fared better than either Ibri hospital (73% vs. 57%; p=0.046) or Ibra hospital (73% vs. 64%; p=0.001) or Nizwa hospital (73% vs. 58%; p=0.001) or Al-Rustaq hospital (73% vs. 47%; p<0.001). Mean positive response rates were not significantly different between the genders (59% vs. 57%; p=0.486) or professions (59% (nurse) vs. 56% (physician) vs. 58% (technician) vs. 57% (pharmacist); p=0.699). There were also no significant differences in mean positive scores with regards to how long staff have worked in the current hospital (p=0.943), how long someone has worked in their current hospital unit/area (p=0.953) or staff level of knowledge on patient safety (p=0.375).
Table 2: Demographic and professional characteristics of the participants.
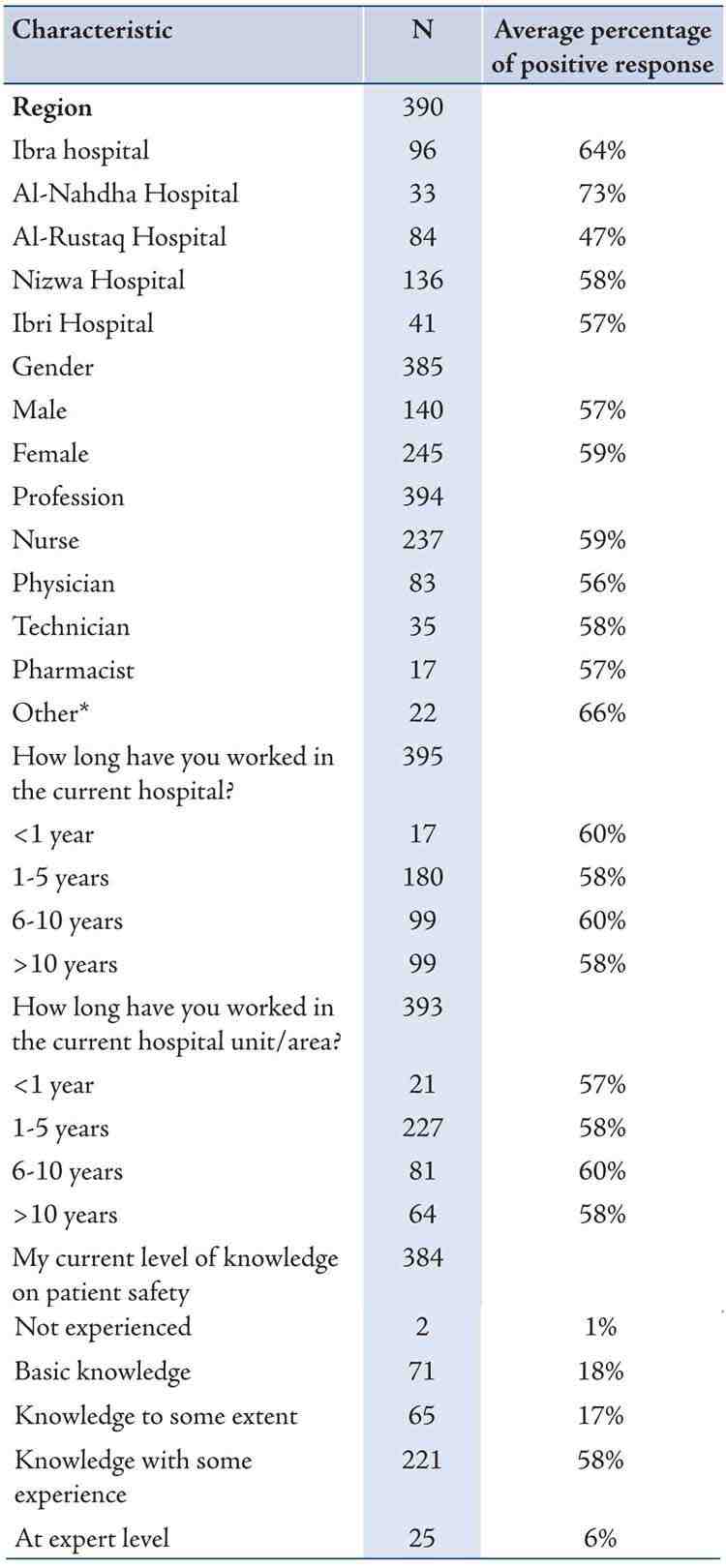
Other*=Includes physiotherapists and dieticians; Analyses were performed using univariate statistics
Composites outcomes are shown in Table 3. The three safety culture dimensions with the highest positive scores were ‘organizational learning – continuous improvement’ (84%), ‘teamwork within units’ (83%), and ‘management support for patient safety’ (67%). The three indices of patient safety culture that were least indorsed included ‘hand-offs and transitions’ (44%), ‘staffing’ (30%) and ‘non-punitive response to error’ (25%).
With regards to comparison with other countries, there were no significant differences in average positive response rates between Oman and the United States (58% vs. 61%; p=0.666), Taiwan (58% vs. 64%; p=0.386) and and Lebanon (58% vs. 61%; p=0.666). In Oman, the dimension that received the highest endorsement was ‘Organizational learning – continuous improvement” (84%). This differs from Taiwan, Lebanon and USA where “Teamwork within units” garnered the highest positive response rate. It may also be theoretically interesting to explore which dimension received the lowest positive response rate. For Oman, Lebanon and the USA, ‘Non-punitive response to error’ received the least positive responses. Taiwan has begged to differ, as ‘Feedback and communication about error” received the least positive response rate.
Oman’s patient safety culture domain of “Teamwork within units” was associated with significantly lower average positive response rates compared to those from Taiwan (83% vs. 94%; p=0.015) but not that different when compared to scores from the USA (83% vs. 78%; p=0.372) and Lebanon (83% vs. 82%; p=0.852). With regards to the composite “Organizational learning – continuous improvement”, Oman’s average positive response rates were significantly higher compared to those from the USA (84% vs. 69%; p=0.012) but not significantly different when compared to those from Taiwan (84% vs 84%; p=1.000) and Lebanon (84% vs. 78%; p=0.279). The average positive response rates from the composite “Overall perception of patient safety” were significantly lower in Oman when compared to those from Lebanon (53% vs. 72%; p=0.006). “Staffing” as a patient safety culture domain, was associated with lower scores for Oman when compared to those from the United States (30% vs. 55%; p<0.001). Furthermore, average positive response rates for “Non-punitive response to error” were significantly lower in Oman when compared to those from the United States (25% vs. 43%; p=0.007) and (25% vs. 45%; p=0.003). They were however, not significantly different when compared to those from Lebanon (25% vs. 24%; p=0.869).
Table 3: Average positive response rates among Oman, USA, Taiwan, and Lebanon cohorts.
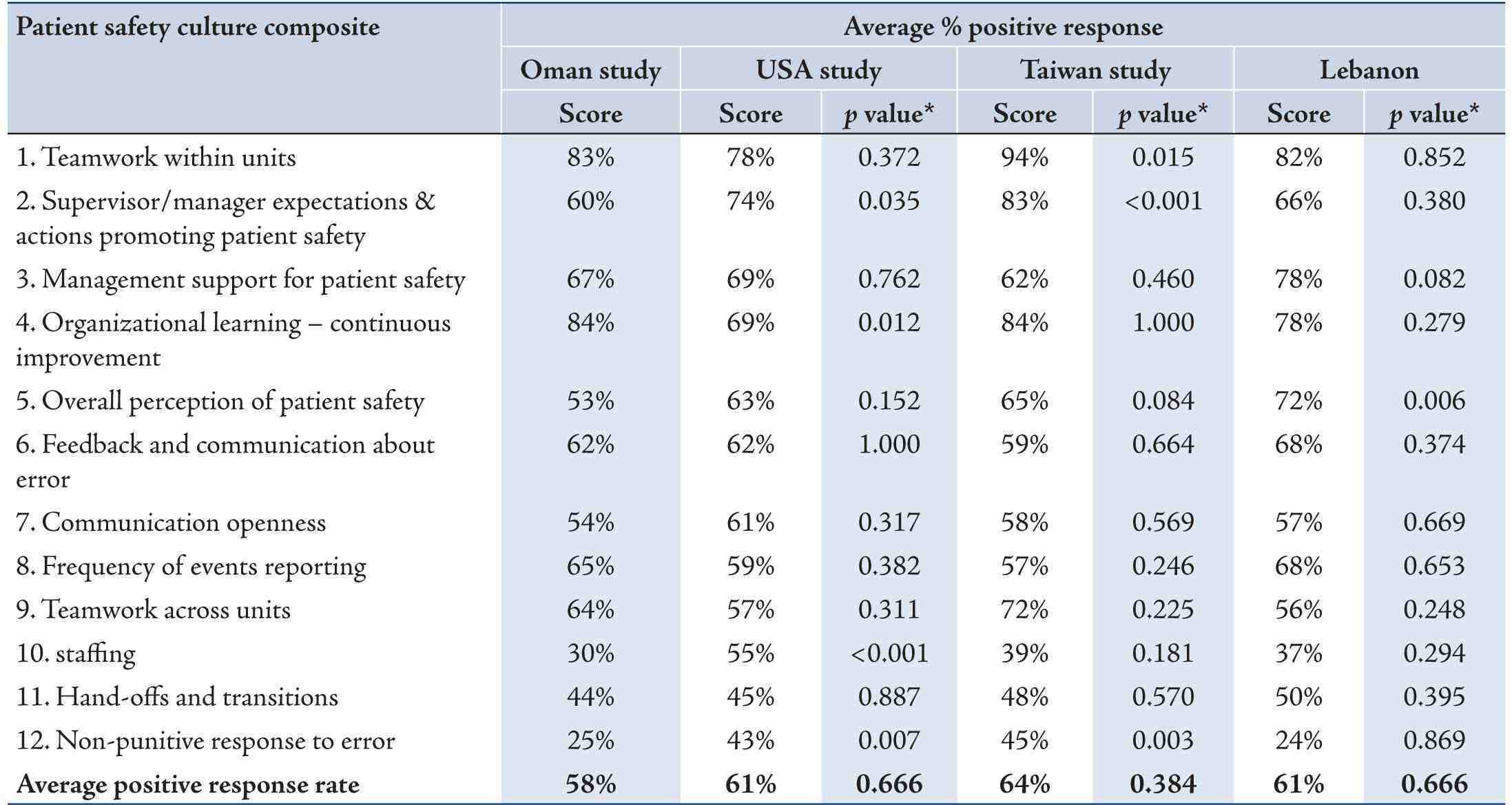
p values were against Oman study and generated using Pearson’s chi-squared and Fisher’s exact tests, wherever appropriate
USA and Taiwan’s average positive response rates were derived from the manuscript by Chen IC and Li HH; BMC Health Serv Res 2010;10:152 while Lebanon’s average positive response rates were extracted from the manuscript by El-Jardali et al; Int J Qual Health Care 2010;22:386-95.
Discussion
As the modern health care setting in Oman is a recent development, the first priority in the previous decade has been to build a healthcare infrastructure which, according to recent estimates was heralded to be ‘miracle of health’ as it has achieved tremendous success in reducing environment-related and infectious diseases.28 What was emphasized was ‘others out there’, namely the patients and diseases that need to be ‘cured’ but what was overlooked is how ‘culture’ within the health care system might be a catalyst for advancing the cause of health. Within such recognition, the World Health Assembly29 has stipulated the importance of upholding the values of patient safety. More recently, there is a concerted effort to highlight the level of patient safety care in Arabic speaking countries.15,27
Judging from some anecdotal and impressionistic observations30 there is evidence to assume that the region is not immune to fall prey to poor patient safety measures. Accordingly, the World Health Organization has suggested that approximately 10% of inpatients admitted in Arab speaking hospitals are likely to have sustained ‘unintended harm.29 In the instance of Oman, the country has also started to witness a dramatic increase in the number of people seeking litigation for malpractice or malpractice claims.31 Other issues that may have direct bearing on safety culture have also been documented in Oman.32,33 Therefore, formal quantification of safety culture using instruments that have international comparison is imperative. Oman’s workforce including healthcare infrastructure have attracted health care workers from different parts of the world. The question remains how the amalgamation of ethnicities and nationals will fare in indices of patient safety culture.
The safety culture dimensions which were endorsed more frequently in the present study were those related to ‘doing things to improve patient safety’, ‘positive changes and ‘its effectiveness’. These variables are under the umbrella of ‘organizational learning -continuous improvement’. This composite was followed by ‘teamwork within units’ and ‘management support for patient safety’. Those that received the least endorsement from health care professionals in Oman included indices of ‘hand-offs and transitions’, ‘staffing’ and ‘non-punitive response to error’. These summarize the situation in Oman but the question remains how such a stance fares in other parts of the world.
This study has also endeavored to compare the USA, Lebanon, Taiwan and Oman on the dimensions most and least endorsed. In comparison to the USA, Lebanon and Taiwan, participants in Oman gave the highest endorsement to ‘Organizational learning–Continuous improvement’. According to AHRQ, the dimension entails ‘a learning culture in which mistakes lead to positive changes and changes are evaluated for effectiveness’. Such endorsement appears to echo the situation in Oman. In its short history of the development of its health care system, Oman has developed its healthcare infrastructure to the extent that it was recently lauded26 as having one of the most efficient health care systems in the world.34 Given this background, it appears that ‘Organizational learning–Continuous improvement’ is an integral part of such a quest.35
In contrast, “Teamwork within units” characterized by the statements like ‘people support one another in this unit’, ‘when a lot of work needs to be done quickly we work together as a team to get the work done’, people treat each other with respect’ and ‘when one area in this unit gets really busy, others help out’ received highest positive response in studies coming from the USA, Taiwan and Lebanon. Again, it may be worthwhile to speculate on the cultural dimension underpinning such an endorsement. Because of its tribal origin and its recent onset, organizational culture in Oman is known to be characterized by ‘directive and paternalistic’ management styles.36 Such management styles indicate the hierarchical nature where ‘loyalty to the leader’ is a common prescription. Conceptually, paternalistic organizational culture is likely to be incompatible to team spirit. It appears that the relegation of teamwork in Oman appears to owe its origin to socio-cultural patterning. Further scrutiny on such hypotheses is therefore warranted.
It is interesting to note also that ‘non-punitive response to error’ received the lowest average positive response rate in Oman as well as for Lebanon and USA. ‘Non-punitive response to error’ encapsulates the idea that ‘staff feel like their mistakes are not held against them’. This also entails that when an event is reported, it suggests that the problem rather than the person is being subjected to scrutiny and the issue is not going to be kept in one’s personnel file. For Oman, since the loyalty to the organization is more important than merit, any errors are likely to be overlooked. More studies are needed to provide contextual information on patient safety culture. There are seminal works indicating that there are diverse national and regional cultural groups that influence organizational culture. Most notable is the work of Hofstede37 which focused on differentiating national and organizational cultures. However, Hofstede’s model has little bearing on safety culture. One aim of this study is to further elucidate the safety culture in different countries and to substantiate whether there are specific cultural underpinnings to patient safety culture. Such findings would likely lead to the understanding of the mechanisms that go to improve patient safety culture. It is obvious that other thing would also have to come to the forefront. For example, according to Al-Abri, “key concerns in Health care management is management of change and health care professionals are obligated both to acquire and to maintain the expertise needed to undertake their professional tasks (p. 9).38 This hospital survey on patient safety culture represents a compilation of large hospital safety data currently available in Oman, and therefore provides a useful reference for comparison. However, several limitations to this study are noteworthy. Firstly, the assessment was given in English. English may not necessarily be the native language, though the ‘lingua Franca’ in Oman among hospital staff is mostly English. Most of the medical schools and technical schools in the Arab world are taught in English. Therefore, it was assumed that the English version of the assessment measure would be adequate for this population. On the other hand, despite protracted sciences of translation, there is indication that although assessments may be translated to achieve conceptual equivalence, they could still be hampered by linguistic and conceptual obstacles which, in turn, could hamper much needed international comparison. Secondly, some critics would contend that it would have been more fruitful to have also employed other assessment measures designed for eliciting patient safety culture such as Safety Attitudes Questionnaire. This scale has been noted to have similar psychometric outcomes to the presently employed HSPSC.6 The rationale for employing HSPSC appears to be its culture-free credential by virtue of having achieved required psychometric properties in various populations including Arab speaking ones.15 However this was not specifically tested in this study. Thirdly, the title of this study ostensibly suggests that this study is about Omanis. However, many technical staffs in Oman hail from different parts of the world, and thus the results may not necessarily be generalizable to only Omanis. Fourthly, only government hospitals in northern Oman were included in this study. This may introduce some bias in as much as private hospitals and smaller hospitals are concerned. Fifthly one aim of the present study is to compare the performance on indices of safety culture as indexed by HSPSC and used in the three other countries noted. Such comparison could be marred with the fact that background information and methodology employed in the studies from Lebanon, Taiwan and USA may not be parallel. It is also worthwhile to note that even in Oman there is difference in indices of safely culture in the hospitals, as this study testifies. It is possible that urban-rural dichotomy may play role in such divergent views within one country. Lastly, but not least, one of the best approaches to adequacy of loading of the survey questions is to employ Cronbach’s coefficient. Generally, Cronbach alpha equal or above 0.70 is thought be to be acceptable.39 However, some studies have failed to reach such loading.15 This study did not set out to check the psychometric properties of this instrument. This is the subject of a future study.
Conclusion
This study explored patient safety culture, using a standardized tool, the Hospital Survey on Patient Safety Culture (HSPSC). The sample consisted of health workers from five secondary and tertiary care hospitals in the northern region of Oman. The study compared the average positive scores on the HSPSC in Oman with similar scores from the USA, Taiwan, and Lebanon. The overall average positive response rate for the patient safety culture dimensions of the HSPSC survey in Oman was 58%. The indices from HSPSC that were endorsed the highest included ‘organizational learning and continuous improvement’ while conversely, ‘non-punitive response to errors’ was ranked the least. Oman appears to fare well on the international indices of patient safety culture. This study indicates the merit of exploring cross-cultural differences in indices of patient safety culture.
Acknowledgements
The authors would like to express their sincere thanks and appreciation to the administration of the five hospitals and staff who participated in the survey. Furthermore, preliminary study findings have already been presented as a poster at the International Forum on Quality and Safety in Healthcare, Paris, France, and April 17-20, 2012. The work was supported by the Eastern Mediterranean Regional Office of the World Health Organization as part of a project carried out to develop patient safety system for the Ministry of Health in Oman. Ethics approval was provided by the local institutional review board (IRB), Research and Ethics Committee of College of Medicine and Health Sciences, Sultan Qaboos University. A-AM was the PI. A-AM, JT and M-AK conceived the idea of the study and were responsible for the design of the study and the acquisition of the data. I-AZ and S-AA provided input into the data analysis. A-AM, I-AZ, M-AK, JT and ASSD contributed to analysis and the interpretation of the results. The initial draft of the manuscript was prepared by A-AM, I-AZ, M-AK and S-AA then circulated repeatedly among all authors for critical revision. All authors helped plan the study, evolve analysis plans, interpret data and critically revise successive drafts of the manuscript.
References
1. Ann Myers SA. Patient Safety and Hospital Accreditation: A Model for Ensuring Success. New York: Springer Publishing Company 2011.
2. Cox SJ, Cox T. The structure of employee attitude to safety: a European example. Work Stress 1991;5:93-106 .
3. Nieva VF, Sorra J. Safety culture assessment: a tool for improving patient safety in healthcare organizations. Qual Saf Health Care 2003 Dec;12(Suppl 2):ii17-ii23.
4. HSC (Health and Safety Commission). 1993. Third report: organizing for safety. ACSNI Study Group on Human Factors. HMSO, London.
5. Alahmadi HA. Assessment of patient safety culture in Saudi Arabian hospitals. Qual Saf Health Care 2010;19:e17.
6. Etchegaray JM, Thomas EJ. Comparing two safety culture surveys: safety attitudes questionnaire and hospital survey on patient safety. BMJ Qual Saf 2012 Jun;21(6):490-498.
7. Moghri J, Arab M, Saari AA, Nateqi E, Forooshani AR, Ghiasvand H, et al. The psychometric properties of the Farsi version of “Hospital survey on patient safety culture” in Iran’s hospitals. Iran J Public Health 2012;41(4):80-86.
8. Sarac C, Flin R, Mearns K, Jackson J. Hospital survey on patient safety culture: psychometric analysis on a Scottish sample. BMJ Qual Saf 2011 Oct;20(10):842-848.
9. Ito S, Seto K, Kigawa M, Fujita S, Hasegawa T, Hasegawa T. Development and applicability of Hospital Survey on Patient Safety Culture (HSOPS) in Japan. BMC Health Serv Res 2011;11:28.
10. Pfeiffer Y, Manser T. Development of the German version of the Hospital Survey on Patient Safety Culture: Dimensionality and psychometric properties. Saf Sci 2010 Dec;48(10):1452-1462 .
11. Singer S, Meterko M, Baker L, Gaba D, Falwell A, Rosen A. Workforce perceptions of hospital safety culture: development and validation of the patient safety climate in healthcare organizations survey. Health Serv Res 2007 Oct;42(5):1999-2021.
12. Smits M, Christiaans-Dingelhoff I, Wagner C, Wal Gv, Groenewegen PP. The psychometric properties of the ‘Hospital Survey on Patient Safety Culture’ in Dutch hospitals. BMC Health Serv Res 2008;8:230.
13. Bodur S, Filiz E. Validity and reliability of Turkish version of “Hospital Survey on Patient Safety Culture” and perception of patient safety in public hospitals in Turkey. BMC Health Serv Res 2010;10:28.
14. Waterson P, Griffiths P, Stride C, Murphy J, Hignett S. Psychometric properties of the Hospital Survey on Patient Safety Culture: findings from the UK. Qual Saf Health Care 2010 Oct;19(5):e2.
15. El-Jardali F, Jaafar M, Dimassi H, Jamal D, Hamdan R. The current state of patient safety culture in Lebanese hospitals: a study at baseline. Int J Qual Health Care 2010 Oct;22(5):386-395.
16. Vlayen A, Hellings J, Claes N, Peleman H, Schrooten W. A nationwide hospital survey on patient safety culture in Belgian hospitals: setting priorities at the launch of a 5-year patient safety plan. BMJ Qual Saf 2012 Sep;21(9):760-767.
17. Sorra JS, Nieva VF. Hospital Survey on Patient Safety Culture. Rockville, MD: AHRQ Publication No. 04-0041; 2004. http://www.ahrq.gov/qual/patientsafetyculture/hospcult.pdf.
18. Al-Awa B, Al Mazrooa A, Rayes O, El Hati T, Devreux I, Al-Noury K, et al. Benchmarking the post-accreditation patient safety culture at King Abdulaziz University Hospital. Ann Saudi Med 2012 Mar-Apr;32(2):143-150.
19. Mwachofi A, Walston SL, Al-Omar BA. Factors affecting nurses’ perceptions of patient safety. Int J Health Care Qual Assur 2011;24(4):274-283.
20. Walston SL, Al-Omar BA, Al-Mutari FA. Factors affecting the climate of hospital patient safety: a study of hospitals in Saudi Arabia. Int J Health Care Qual Assur 2010;23(1):35-50.
21. Parand A, Burnett S, Benn J, Pinto A, Iskander S, Vincent C. The disparity of frontline clinical staff and managers’ perceptions of a quality and patient safety initiative. J Eval Clin Pract 2011 Dec;17(6):1184-1190.
22. Aboul-Fotouh AM, Ismail NA, Ez Elarab HS, Wassif GO. Assessment of patient safety culture among healthcare providers at a teaching hospital in Cairo, Egypt. East Mediterr Health J 2012 Apr;18(4):372-377.
23. Hafez S, Saied T, Hasan E, Elnawasany M, Ahmad E, Lloyd L, et al. Incidence and modifiable risk factors of surveillance of surgical site infections in Egypt: a prospective study. Am J Infect Control 2012 Jun;40(5):426-430.
24. Ahmed NG, Adam SM, Al-Moniem II. Patient safety: Assessing nurses’ perception and developing an improvement plan. Life Science Journal 2011;8:53-64.
25. Zohar D, Livne Y, Tenne-Gazit O, Admi H, Donchin Y. Healthcare climate: a framework for measuring and improving patient safety. Crit Care Med 2007 May;35(5):1312-1317.
26. Health Systems Profile- Oman. Health care financing and expenditure. GIShttp://gis.emro.who.int/HealthSystemObservatory/PDF/Oman/Health%20care%20financing%20and%20expenditure.pdf. Accessed April, 2013
27. El-Jardali F, Dimassi H, Jamal D, Jaafar M, Hemadeh N. Predictors and outcomes of patient safety culture in hospitals. BMC Health Serv Res 2011; 24; 11:45.
28. Al-Sinawi H, Al-Alawi M, Al-Lawati R, Al-Harrasi A, Al-Shafaee M, Al-Adawi S. Emerging Burden of Frail Young and Elderly Persons in Oman: For whom the bell tolls? Sultan Qaboos Univ Med J 2012 May;12(2):169-176.
29. Regional strategy for enhancing patient safety: Technical paper. Regional Committee for the EM/RC52/4 Eastern Mediterranean September 2005. Fifty-second Sessions.
30. Al-Aameri AS. Job satisfaction and organizational commitment for nurses. Saudi Med J 2000 Jun;21(6):531-535.
31. Al-Mandhari A. Report of the situational analysis of patient safety system in Ministry of Health institutions. WHO-EMRO. 2009; February – May.
32. Levin AV, Ganesh A, Al-Busaidi A. Fee splitting in ophthalmology. Can J Ophthalmol 2011 Feb;46(1):21-27.
33. Kp P, Arora V, Pp G. Bloodstream Bacterial Pathogens and their Antibiotic Resistance Pattern in Dhahira Region, Oman. Oman Med J 2011 Jul;26(4):240-279.
34. Alshishtawy MM. Four Decades of Progress: Evolution of the health system in Oman. Sultan Qaboos Univ Med J 2010 Apr;10(1):12-22.
35. Alhatmi Y. Safety as a hospital organizational priority: A case study. Clin Gov 2011;16:203-219 .
36. Common R. Administrative change in the Gulf: Modernization in Bahrain and Oman. International Review of Administrative Sciences 2008;74:177-193 .
37. Hofstede G. Cultures and Organizations: Software of the Mind. Adm Sci Q 1993;38:132-134 .
38. Al-Abri R. Managing change in healthcare. Oman Med J 2007 Oct;22(3):9-10.
39. Bowling A. Research Methods in Health: Investigating Health and Health Services. Buckingham: Open University Press, 1997.
|