| |
Abstract
Objective: Micronutrient deficiency during pregnancy is associated with several complications. This study was designed to determine the effects of received multivitamin-mineral vs. multivitamin supplements on maternal, newborns' biochemical indicators, and birth size.
Methods: This double-blind randomized-controlled clinical trial was conducted among 48 Iranian pregnant women, primigravida, aged 18-35 years old in their second and third trimester from December 2011 to September 2012. Subjects were randomly assigned to receive either the multivitamin-mineral (n=24) or multivitamin supplements (n=24) for 20 weeks. Fasting blood samples were taken at baseline and after a 20-week intervention of pregnant women as well as umbilical cord blood of the babies immediately after delivery to measure serum calcium, vitamin D, iron, magnesium, zinc and biomarkers of oxidative stress including plasma total antioxidant capacity and total glutathione.
Results: Multivitamin-mineral compared to multivitamin supplementation resulted in a significant increase in maternal serum calcium (0.5 vs. -0.1 mg/dL, p=0.04) and magnesium levels (0.1 vs. -0.2 mg/dL, p<0.001). Furthermore, mean plasma total glutathione levels (1791 ± 566 vs. 1434 ± 622 µmol/l, p=0.04) of the newborns whose mothers received multivitamin-mineral were higher than those whose mothers received multivitamin supplements.
Conclusions: Overall, multivitamin-mineral compared to multivitamin supplementation for 20 weeks during pregnancy resulted in a significant increase in maternal serum calcium and magnesium levels as well as a significant elevation of newborn plasma total glutathione levels.
Keywords: Micronutrient; Supplementation; Pregnancy outcomes; Oxidative stress.
Introduction
Owing to increased requirements for micronutrients during pregnancy, pregnant women are one of the most susceptible groups for nutritional insufficiency.1,2 In Kashan, Iran, it has been reported that 96, 7 and 9% of pregnant women have low levels of vitamin D,3 zinc and hemoglobin.4 Furthermore, about 16% of all live births worldwide are low birth weight babies (LBW); 90% of whom are born in low-income countries.5 This rate is considerably high in Asian countries.6 Increased metabolic demands for micronutrients during pregnancy occur mainly due to changes in the women's physiology and the requirements of the growing fetus.7 Micronutrient deficiencies during pregnancy may result in spontaneous abortion, fetal malformation,8 placental abruption,9 increased maternal morbidity,10 pre-eclampsia, increased oxidative stress,11 as well as LBW.12
Several studies have evaluated the effects of multiple micronutrients supplementation on pregnancy outcomes.13,14 In a systematic review, it has been reported that multiple micronutrient supplementation as compared to the usual iron-folate supplements during pregnancy have beneficial effects in reducing LBW and small for gestational age (SGA) births.15 However, there was no significant difference seen in the overall risk of preterm birth, stillbirth, and maternal or neonatal mortality following the intake of multiple micronutrients compared with iron-folate after the first trimester.16 Furthermore, multiple micronutrient supplementation during pregnancy did not reduce early infant mortality17; however, it has resulted in improved folate status and reduced the prevalence of riboflavin, vitamin B6, vitamin B12, folate, and vitamin D deficiencies.18 In another study, improved vitamin E and A status was also seen with consuming multiple micronutrient supplements (consisted of 15 vitamins and minerals) compared to controls from 20 to 32 weeks of gestation.19 Most previous studies have been performed in communities with a high prevalence of maternal malnutrition and it remains unknown if these supplementations improved pregnancy outcomes in other populations. Evidence for the impact of multiple micronutrient supplementations on a number of outcomes is still inadequate and further research is required before a switch from iron-folate supplementation is implemented.20 In addition, earlier studies have mostly compared micronutrient supplementation with the placebo or iron-folate intake. To date, few studies have shown the impact of multiple micronutrient supplementations during pregnancy on biochemical indicators of pregnant women and especially their newborns. Furthermore, there are insufficient evidences whether different types of multiple micronutrient supplements may have had differential benefits for pregnant women. This study was therefore, conducted to investigate the effects of two types of multiple micronutrient (multivitamin-mineral vs. multivitamin) supplementations on maternal, newborn biochemical indicators, and birth size in pregnant Iranian women.
Methods
This randomized double-blind controlled clinical trial was conducted in Kashan, Iran during December 2011 to September 2012. A detailed description of multiple micronutrient supplementations, the intervention, data collection and primary results had been published previously worldwide.21-23 The methods were reviewed briefly, with emphasis on those that are relevant to the assessment of micronutrients status. On the basis of that sample size formula suggested for randomized clinical trials,24 the type I error of 5% (α=0.05) and type II error of 20% (β=0.20; Power=80%) and maternal serum iron as a key variable were considered and the sample size of 24 persons was reached for each group. The study was conducted at the Naghavi Maternity Clinic, Shaheed Beheshti Subspecialty Polyclinic and 20 antenatal centers affiliated with Kashan University of Medical Sciences. A total of 90 pregnant women were screened for this study wherein 54 met the inclusion criteria (25 women due to multiparous and 11 women because of not living in Kashan were excluded). Inclusion criteria were as follows: primigravidity, singleton pregnancy and age between 18-35 years. Women with hypertension, gestational diabetes mellitus (GDM), complete bed rest (CBR), intrauterine fetal death (IUFD), intrauterine growth retardation (IUGR), placental abruption, preterm delivery, hospitalization, signs of malabsorption and maldigestion, history or evidence of rheumatoid arthritis, thyroid, parathyroid or adrenal diseases, hepatic or renal failure and metabolic bone disease were excluded from the study. All pregnant women took 400 µg/d folic acid supplements from the beginning of pregnancy as well as 60 mg/d ferrous sulfate (before bedtime) from the second trimester to delivery time. The study was performed according to the guidelines expressed in the Declaration of Helsinki and approved by the Ethics Committee of Kashan University of Medical Sciences (P/29/5/1/1384, 21 May 2012). All participants provided informed written consent. The trial was registered in the Iranian website (www.irct.ir) for registration of clinical trials (IRCT code: IRCT201204065623N3).
Subjects were randomly assigned to receive either a multivitamin-mineral (n=24) or multivitamin supplements (n=24) from week 17 to 37 of gestation. All participants were asked to take one supplement a day (after lunch). Random assignment was done by the use of computer-generated random numbers. A trained midwife at the maternity clinic performed randomization. They were also asked not to alter their routine physical activity and usual diet throughout the study. Dietary intakes of participants were assessed by means of three-day dietary records completed at run-in period and throughout the study. Run-in period is a period before a clinical trial is commenced when no treatment is given. The dietary records were based on estimated values in household measurements. The multivitamin-mineral and multivitamin supplements were provided by Shahre Daru Co, Tehran, Iran. Supplements were provided to subjects monthly. The multivitamin-mineral supplement consisted of 13 micronutrients. The multivitamin supplement (the same substance without elements of iron, magnesium and calcium) was packed in identical tablets and coded by the producer to guarantee blinding. All supplements were kept under cool temperature before use. Compliance with the supplement consumption was monitored once per month through phone interviews. The compositions of the supplements are provided in Table 1. Data on anthropometric and biochemical measures were collected at the maternity clinic and Kashan reference laboratory affiliated to Kashan University of Medical Sciences, respectively. Gestational age was calculated from the date of last menstrual period and concurrent clinical assessment.25
Maternal anthropometric measurements were assessed at baseline and after 20 weeks of intervention. Maternal weight was assessed by trained midwives at maternity clinic in an overnight fasting status, without shoes and in minimal clothing using a digital scale (Seca, Hamburg, Germany) to the nearest 0.1 kg. Height was measured using a non-stretched tape measure (Seca, Hamburg, Germany) to the nearest 0.1 cm. BMI was calculated as weight in kg divided by height in meters squared. The pre-pregnancy weight and height were taken from the existing records of patients in the clinic.26 Newborn height and weight were measured using standard methods (Seca 155 Scale, Hamburg, Germany) during the first 24 hours after birth and were recorded to the nearest 1 mm and 10 g, respectively.4 Newborn head circumference was measured to the nearest 1 mm with a Seca girth measuring tape.4
For the biochemical assessment, maternal fasting blood samples (10 mL) were taken at baseline and after a 20-week intervention early in the morning at a Kashan reference laboratory after an overnight fast.27 Furthermore, 5 mL cord blood was collected from the umbilical cord of the babies immediately after delivery by clamping and cutting the babies' end of the cord. Serum samples were analyzed for serum calcium, magnesium, zinc, iron and 25-hydroxy vitamin D levels. Serum calcium, iron and magnesium concentrations were assayed using mentioned kits (Pars Azmoon, Tehran, Iran) by automatic biochemistry analyzer (BT 3000, Monsano, Italy). A serum zinc concentration was assayed using zinc kit (Elitech, Puteaux, France) by automatic biochemistry analyzer (BT 3000, Monsano, Italy). Serum 25-hydroxy vitamin D was assayed by ELISA (Awareness Stat Fax 2100, Bohemia, USA) using available kits (IDS, Boldon, UK). Plasma samples were determined for total antioxidant capacity (TAC) and total glutathione (GSH) levels. TAC was assessed using the FRAP method developed by Benzie and Strain.26 The plasma total GSH was measured using Beutler et al. method.28 Plasma TAC and total GSH were determined using spectrophotometry method (Cecil 2021, Cambridge, England).
To ensure normal distribution of variables, Kolmogrov-Smirnov test was applied for statistical analysis. The paired-samples t-test was used to identify within group differences (before and after intervention). Student’s t-test was used to detect differences between the two groups (multivitamin-mineral and multivitamin supplements). Distribution of participants in terms of categorical variables was examined through the use of chi-square test. A p-value of <0.05 was considered as statistically significant. All statistical analyses were done using the Statistical Package for Social Science version 17 (SPSS Inc, Chicago, USA).
Results
The exclusions in the multivitamin-mineral group were three persons (hospitalization [n=1], GDM [n=1] and placenta abruption [n=1]) Among individuals in the multivitamin group, three women (CBR [n=1], IUGR [n=1] and severe pre-eclampsia [n=1]) were excluded. Finally, 48 participants (a multivitamin-mineral group [n=24] and a multivitamin [=24]) completed the trial. Mean age, pre-pregnancy weight and BMI were not statistically different between the two groups (Table 2). There were no significant differences as to the baseline weight and BMI as well as post-intervention means for these variables between the multivitamin-mineral and multivitamin groups. Gestational age and the rate of cesarean section were not significant between the two groups. Based on three-day dietary records, no significant difference between the two groups was found in terms of dietary intakes of energy, calcium, iron, magnesium, zinc and dietary fiber (data not shown).
A significant rise in maternal plasma total GSH (changes from baseline: +109 ± 420 vs. -163 ± 270 µmol/L, p=0.01) was observed following the consumption of multivitamin-mineral vs. multivitamin supplements. Multivitamin-mineral compared to multivitamin supplementation led to a significant increase in maternal serum calcium (0.5 vs. -0.1 mg/dL, p=0.04) and magnesium levels (0.1 vs. -0.2 mg/dL, p<0.001) (Table 3). No significant differences were seen comparing multivitamin-mineral and multivitamin in terms of their effects on maternal serum iron, zinc and vitamin D levels.
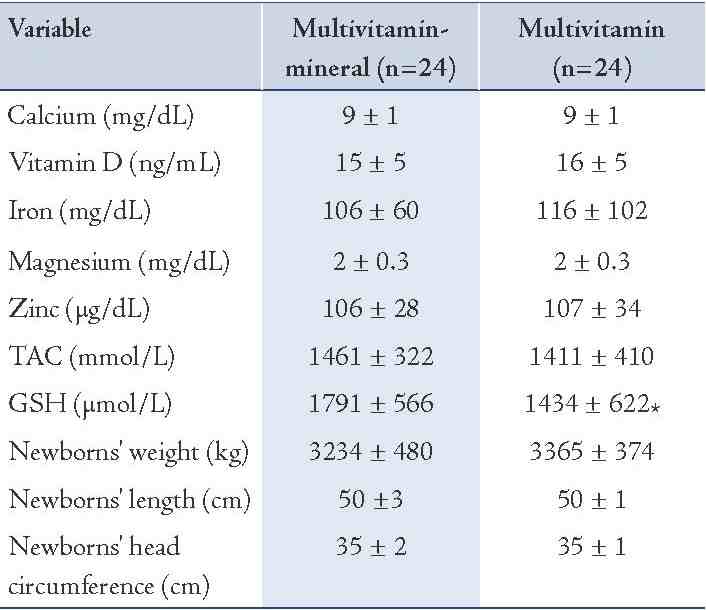
Although no significant difference was seen in newborn weight, height, head circumference, serum calcium, vitamin D, iron, magnesium, zinc and plasma TAC concentrations between the two groups, mean plasma total GSH levels (1791 ± 566 vs. 1434 ± 622 µmol/L, p=0.04) of the newborns whose mothers received multivitamin-mineral were higher than those whose mothers received multivitamin supplements. (Table 4)
Table 1: Composition of dietary supplements used in the study.
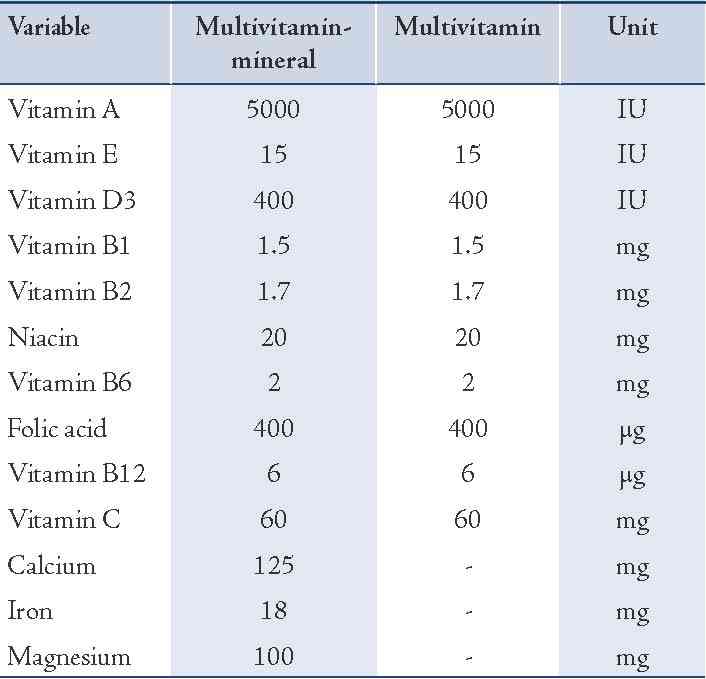
Table 2: General characteristics of the study participants.
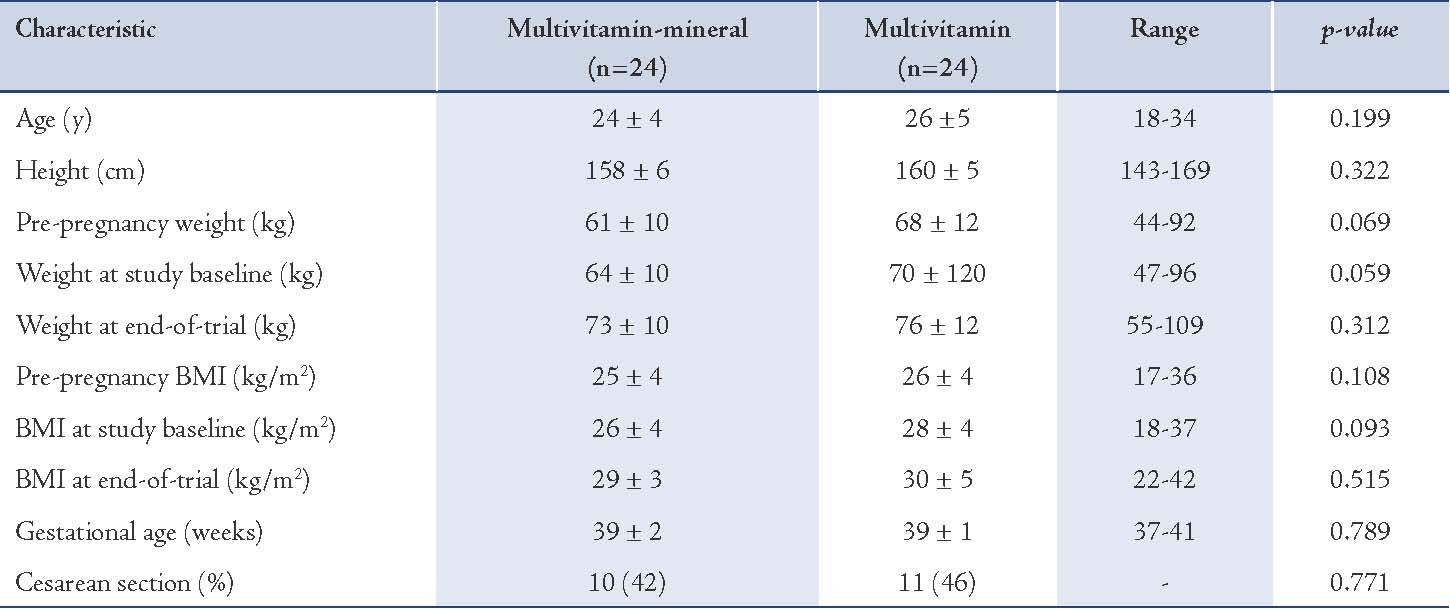
Table 3: Mean (±standard deviation) of maternal biochemical indicators at baseline and after the intervention.
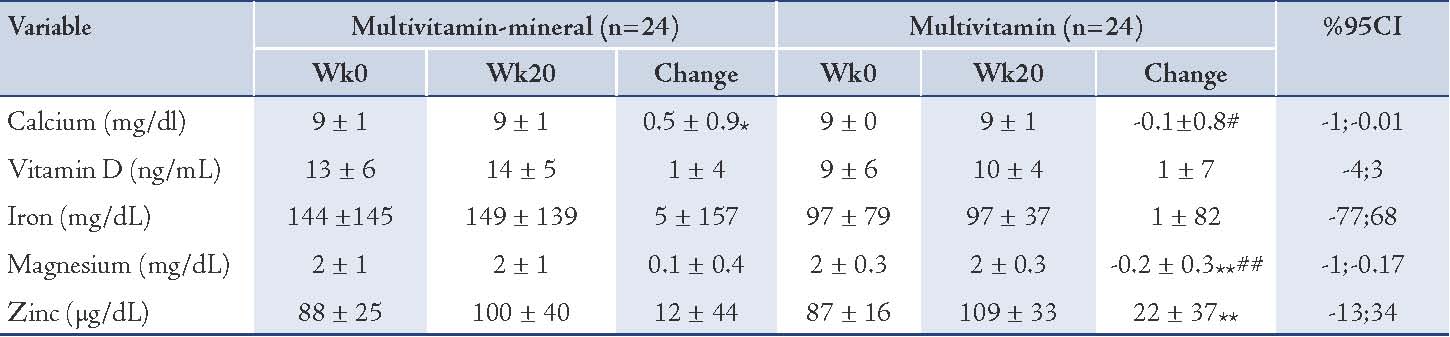
Table 4: The effect of multivitamin-mineral vs. multivitamin supplementation on newborn biochemical indicators and birth size.
Discussion
The present study showed that multivitamin-mineral vs. multivitamin supplementation for 20 weeks among pregnant women had beneficial effects on maternal serum calcium and magnesium as well as newborn plasma total GSH levels. No favorable effects were found with the patients who received multivitamin-mineral on maternal serum iron, zinc and vitamin D levels as well as on newborn serum calcium, vitamin D, iron, magnesium, zinc, plasma TAC levels and birth size compared to multivitamin supplements. Pregnant women are susceptible to nutritional micronutrients deficiency. It was reported that multiple micronutrients deficiency during pregnancy would result in several aberrations in maternal and fetal health.9,11,29,30
The current study demonstrated that multivitamin-mineral vs. multivitamin supplementation for 20 weeks during pregnancy increased maternal serum calcium and magnesium levels but could not affect maternal serum iron, zinc, vitamin D as well as newborn serum calcium, vitamin D, iron, magnesium and zinc levels. In line with this study, maternal increased levels of serum calcium has been reported with consumption of orange juice fortified with calcium in adolescent pregnant mothers but could not affect newborn serum calcium status.31 Multiple micronutrient supplementations during pregnancy also decreased the prevalence of serum riboflavin, vitamin B6, vitamin B12, folate and vitamin D deficiencies compared to controls for 32 weeks.18 Firouzabadi et al.32 has also shown increased levels of serum calcium and vitamin D with 1000 mg/day calcium plus vitamin D 100000 IU/month supplementation for 6 months in infertile women with polycystic ovary syndrome (PCOS). Similar increase in maternal serum calcium status was also seen with consuming calcium during pregnancy.33 Supplementation with multiple micronutrients has also resulted in improved folate, vitamin B12, B6 and riboflavin status between baseline and the third trimester compared to controls receiving vitamin C only.18 However, supplementation with multiple micronutrients during pregnancy could not improve maternal or newborn serum zinc or vitamin A status compared to supplementation with iron only for 9 weeks.21 Micronutrient malnutrition during pregnancy, particularly iron deficiency, continues to be an important public health problem among the poor in Iran. Although the prevalence of calcium, magnesium and iron deficiency was low and deficiency is rare, it is still of concern due to the important implications for pregnancy outcomes. The difference between the current findings and other studies might be explained by the different study designs, sample sizes, duration and dosage of supplementation as well as composition of nutrients used in the supplements. Furthermore, it is possible that the lack of impact observed in other studies is related to compliance with the supplementation. Compliance in this study was high (over 90% in both groups) and began at an average of 20 weeks of pregnancy, leaving ample time for impact.
There was no significant effect found with multivitamin-mineral vs. multivitamin supplementation after 20 weeks during pregnancy on newborns' birth size. In agreement with this study, Ramakrishnan et al.23 has shown that multiple micronutrient supplementation from 13 weeks of gestation until delivery does not lead to greater newborn birth size when compared to iron-only supplementation. The administration of multimicronutrients to undernourished pregnant women could not affect newborn birth size compared to the placebo for 2 months.34 Similar findings were seen in a cluster-randomized controlled trial among pregnant women found receiving multiple micronutrients supplements for 5 days per weeks compared with iron-folic acid supplements.35 However, prenatal supplementation with multiple micronutrients after 150 days had a greater positive impact on birth weight than supplementation with iron/folic acid.36 Multiple micronutrient supplementations from weeks 12-16 of gestation to delivery also led to a significant increase in birth size compared with placebo but could not affect head circumference.37 The inconsistency in the present findings with other studies may be due to the lack of a unique cutoff level for defining deficiency of micronutrient in pregnancy or because of considering deficiency of micronutrient regardless of the overall nutritional status of the pregnant women. Small sample size might also provide further reasons for multiple micronutrients supplementation's effects on birth size.
The present study showed that consuming multivitamin-mineral vs. multivitamin supplements for 20 weeks during pregnancy led to a significant increase in newborn plasma total GSH levels, but could not affect TAC levels. In a study by Adams et al.38 vitamin/mineral supplementation in children and adults with autism resulted in significant improvements of metabolic status including total sulfate, reduced glutathione and ratio of oxidized glutathione to reduced glutathione (GSSG: GSH). A significant increase of GSH and uric acid levels with moderate multivitamin-mineral supplementation was also seen in athletes after three weeks.39 The same findings have been documented with administration of multiple micronutrients in Chinese children after 3 weeks.40 In addition, calcium supplementation (0.9%) in the nutrition of high-fat diet (HFD) mice after 9 weeks showed increased duodenal glutathione and oxidized glutathione (GSH/GSSG) ratios but could not affect TAC levels.41 Magnesium supplementation (40 mg/kg) has also shown a significant increase in total GSH and TAC levels in male Wistar rats after four weeks.42 Several mechanisms may explain the favorable effects of multivitamin-mineral supplementation on newborn biomarkers of oxidative stress. The calcium elements of multivitamin-mineral supplements may act as direct antioxidants and DNA damage reducing agents resulting in maternal free radical scavenging,43 and then might lead to decreased transfer of free radicals from mother to fetus and thus increase the status of newborn plasma total GSH. Increased maternal plasma GSH levels following the consumption of multivitamin-mineral compared with multivitamin supplements may elevate its transfer to the fetus and then lead to increased newborn plasma GSH levels. In a study by Kuster et al.44 a strong correlation was observed between maternal and fetal GSH and cysteine (precursor of GSH biosynthesis). Nonetheless, little evidence from trials exists to evaluate the effect of micronutrients supplementation during pregnancy on biomarkers of oxidative stress in pregnant women and their newborns. In addition, increased levels of maternal serum magnesium from multivitamin-minerals supplementation might result in elevated total GSH levels in newborns by restoring the activity of anti-oxidative enzymes and scavenging oxygen radicals.45,46
Several limitations must be considered in the interpretation of the findings of this study. Due to budget limitations, maternal systemic inflammatory factors, insulin resistance and other biomarkers of oxidative stress were not assessed. In addition, the beneficial effects of multivitamin-mineral and multivitamin supplementation on the other biochemical indicators of newborns could not be assessed. Small sample size could potentially account for lack of detecting significant difference on birth size despite the significant increase in maternal serum calcium and magnesium levels. Furthermore, the effect of water retention on biochemical markers was not assessed due to lack of resources and technical difficulties.
Conclusion
Multivitamin-mineral compared to multivitamin supplementation after 20 weeks during pregnancy resulted in improved biochemical indicators of pregnant women and their newborns including maternal serum calcium and magnesium levels as well as newborn plasma total GSH, but had no effect on maternal serum iron, zinc and vitamin D levels as well as newborns' serum calcium, vitamin D, iron, magnesium, zinc, plasma TAC levels and birth size. Further studies are recommended to assess the effects of multivitamin-mineral and multivitamin supplementation on lipid profiles, insulin resistance and inflammatory factors in pregnant women and their newborns as well as other pregnancy outcomes including neonatal hyperbilirubinemia and respiratory distress syndrome.
Acknowledgements
The present study was supported by a grant from the Vice-chancellor for Research, KUMS, and Iran. The authors would like to thank the staff of Naghavi and Shaheed Beheshti Clinics, Kashan, Iran for their assistance in this project. No conflict of interest to declare.
References
1. Allen LH. Multiple micronutrients in pregnancy and lactation: an overview. Am J Clin Nutr 2005 May;81(5):1206S-1212S.
2. Shah PS, Ohlsson A; Knowledge Synthesis Group on Determinants of Low Birth Weight and Preterm Births. Effects of prenatal multimicronutrient supplementation on pregnancy outcomes: a meta-analysis. CMAJ 2009 Jun;180(12):E99-E108.
3. Asemi Z, Taghizadeh M, Sarahroodi S, Jazayeri S, Tabasi Z, Seyyedi F. Assessment of the relationship of vitamin D with serum antioxidant vitamins E and A and their deficiencies in Iranian pregnant women. Saudi Med J 2010 Oct;31(10):1119-1123.
4. Samimi M, Asemi Z, Taghizadeh M, Azarbad Z, Rahimi-Foroushani A, Sarahroodi S. Concentrations of Serum Zinc, Hemoglobin and Ferritin among Pregnant Women and their Effects on Birth Outcomes in Kashan, Iran. Oman Med J 2012 Jan;27(1):40-45.
5. Kositamongkol S, Suthutvoravut U, Chongviriyaphan N, Feungpean B, Nuntnarumit P. Vitamin A and E status in very low birth weight infants. J Perinatol 2011 Jul;31(7):471-476.
6. Roberfroid D, Huybregts L, Lanou H, Henry MC, Meda N, Menten J, et al; MISAME Study Group. Effects of maternal multiple micronutrient supplementation on fetal growth: a double-blind randomized controlled trial in rural Burkina Faso. Am J Clin Nutr 2008 Nov;88(5):1330-1340.
7. Hess SY, King JC. Effects of maternal zinc supplementation on pregnancy and lactation outcomes. Food Nutr Bull 2009 Mar;30(1)(Suppl):S60-S78.
8. Molloy AM, Kirke PN, Brody LC, Scott JM, Mills JL. Effects of folate and vitamin B12 deficiencies during pregnancy on fetal, infant, and child development. Food Nutr Bull. 2008;29(2 Suppl):S101-11; discussion S12-5.
9. Pathak P, Kapil U. Role of trace elements zinc, copper and magnesium during pregnancy and its outcome. Indian J Pediatr 2004 Nov;71(11):1003-1005.
10. Haider BA, Yakoob MY, Bhutta ZA. Effect of multiple micronutrient supplementation during pregnancy on maternal and birth outcomes. BMC Public Health 2011;11(Suppl 3):S19.
11. Rumiris D, Purwosunu Y, Wibowo N, Farina A, Sekizawa A. Lower rate of preeclampsia after antioxidant supplementation in pregnant women with low antioxidant status. Hypertens Pregnancy 2006;25(3):241-253.
12. Pathak P, Kapil U, Kapoor SK, Saxena R, Kumar A, Gupta N, et al. Prevalence of multiple micronutrient deficiencies amongst pregnant women in a rural area of Haryana. Indian J Pediatr 2004 Nov;71(11):1007-1014.
13. Bo S, Pisu E. Role of dietary magnesium in cardiovascular disease prevention, insulin sensitivity and diabetes. Curr Opin Lipidol 2008 Feb;19(1):50-56.
14. Saker M, Soulimane Mokhtari N, Merzouk SA, Merzouk H, Belarbi B, Narce M. Oxidant and antioxidant status in mothers and their newborns according to birthweight. Eur J Obstet Gynecol Reprod Biol 2008 Dec;141(2):95-99.
15. Zerfu TA, Ayele HT. Micronutrients and pregnancy; effect of supplementation on pregnancy and pregnancy outcomes: a systematic review. Nutr J 2013;12(1):20.
16. Ramakrishnan U, Grant FK, Goldenberg T, Bui V, Imdad A, Bhutta ZA. Effect of multiple micronutrient supplementation on pregnancy and infant outcomes: a systematic review. Paediatr Perinat Epidemiol 2012 Jul;26(Suppl 1):153-167.
17. Christian P, Osrin D, Manandhar DS, Khatry SK, de L Costello AM, West KP Jr. Antenatal micronutrient supplements in Nepal. Lancet 2005 Aug;366(9487):711-712.
18. Christian P, Jiang T, Khatry SK, LeClerq SC, Shrestha SR, West KP Jr. Antenatal supplementation with micronutrients and biochemical indicators of status and subclinical infection in rural Nepal. Am J Clin Nutr 2006 Apr;83(4):788-794.
19. Osrin D, Vaidya A, Shrestha Y, Baniya RB, Manandhar DS, Adhikari RK, et al. Effects of antenatal multiple micronutrient supplementation on birthweight and gestational duration in Nepal: double-blind, randomised controlled trial. Lancet 2005 Mar;365(9463):955-962.
20. Haider B, Bhutta Z. Multiple-micronutrient supplementation for women during pregnancy. status and date: Edited (no change to conclusions), published in. 2006;1.
21. García-Guerra A, Neufeld LM, Hernández-Cordero S, Rivera J, Martorell R, Ramakrishnan U. Prenatal multiple micronutrient supplementation impact on biochemical indicators during pregnancy and postpartum. Salud Publica Mex 2009 Jul-Aug;51(4):327-335.
22. Ramakrishnan U, Aburto N, McCabe G, Martorell R. Multimicronutrient interventions but not vitamin a or iron interventions alone improve child growth: results of 3 meta-analyses. J Nutr 2004 Oct;134(10):2592-2602.
23. Ramakrishnan U, González-Cossío T, Neufeld LM, Rivera J, Martorell R. Multiple micronutrient supplementation during pregnancy does not lead to greater infant birth size than does iron-only supplementation: a randomized controlled trial in a semirural community in Mexico. Am J Clin Nutr 2003 Mar;77(3):720-725.
24. Allen LH, Peerson JM; Maternal Micronutrient Supplementation Study Group. Impact of multiple micronutrient versus iron-folic acid supplements on maternal anemia and micronutrient status in pregnancy. Food Nutr Bull 2009 Dec;30(4)(Suppl):S527-S532.
25. Gupta P, Narang M, Banerjee BD, Basu S. Oxidative stress in term small for gestational age neonates born to undernourished mothers: a case control study. BMC Pediatr 2004 Jul;4(1):14.
26. Asemi Z, Jazayeri S, Najafi M, Samimi M, Tabasi Z, Shidfar F, et al. Plasma total antioxidant capacity and its related factors in Iranian pregnant women. Saudi Med J 2011 Dec;32(12):1246-1250.
27. Tworoger SS, Hankinson SE. Collection, processing, and storage of biological samples in epidemiologic studies: sex hormones, carotenoids, inflammatory markers, and proteomics as examples. Cancer Epidemiol Biomarkers Prev 2006 Sep;15(9):1578-1581.
28. Surapaneni KM, Venkataramana G. Status of lipid peroxidation, glutathione, ascorbic acid, vitamin E and antioxidant enzymes in patients with osteoarthritis. Indian J Med Sci 2007 Jan;61(1):9-14.
29. Gasim T. Gestational diabetes mellitus: maternal and perinatal outcomes in 220 saudi women. Oman Med J 2012 Mar;27(2):140-144.
30. Kamil A, Khorshid E. Maternal perceptions of antenatal care provision at a tertiary level hospital, riyadh. Oman Med J 2013 Jan;28(1):33-35.
31. Chan GM, McElligott K, McNaught T, Gill G. Effects of dietary calcium intervention on adolescent mothers and newborns: A randomized controlled trial. Obstet Gynecol 2006 Sep;108(3 Pt 1):565-571.
32. Firouzabadi Rd, Aflatoonian A, Modarresi S, Sekhavat L, MohammadTaheri S. Therapeutic effects of calcium & vitamin D supplementation in women with PCOS. Complement Ther Clin Pract 2012 May;18(2):85-88.
33. Chung M, Balk EM, Brendel M, Ip S, Lau J, Lee J, et al. Vitamin D and calcium: a systematic review of health outcomes. Evid Rep Technol Assess (Full Rep) 2009 Aug;(183):1-420.
34. Gupta P, Ray M, Dua T, Radhakrishnan G, Kumar R, Sachdev HP. Multimicronutrient supplementation for undernourished pregnant women and the birth size of their offspring: a double-blind, randomized, placebo-controlled trial. Arch Pediatr Adolesc Med 2007 Jan;161(1):58-64.
35. Sunawang UB, Utomo B, Hidayat A, Kusharisupeni, Subarkah. Preventing low birthweight through maternal multiple micronutrient supplementation: a cluster-randomized, controlled trial in Indramayu, West Java. Food Nutr Bull 2009 Dec;30(4)(Suppl):S488-S495.
36. Zagré NM, Desplats G, Adou P, Mamadoultaibou A, Aguayo VM. Prenatal multiple micronutrient supplementation has greater impact on birthweight than supplementation with iron and folic acid: a cluster-randomized, double-blind, controlled programmatic study in rural Niger. Food Nutr Bull 2007 Sep;28(3):317-327.
37. Hininger I, Favier M, Arnaud J, Faure H, Thoulon JM, Hariveau E, et al. Effects of a combined micronutrient supplementation on maternal biological status and newborn anthropometrics measurements: a randomized double-blind, placebo-controlled trial in apparently healthy pregnant women. Eur J Clin Nutr 2004 Jan;58(1):52-59.
38. Adams JB, Audhya T, McDonough-Means S, Rubin RA, Quig D, Geis E, et al. Effect of a vitamin/mineral supplement on children and adults with autism. BMC Pediatr 2011;11:111.
39. Machefer G, Groussard C, Vincent S, Zouhal H, Faure H, Cillard J, et al. Multivitamin-mineral supplementation prevents lipid peroxidation during "the Marathon des Sables". J Am Coll Nutr 2007 Apr;26(2):111-120.
40. Zhang M, Ma AG, Zhang XZ, Ge S, Shi XX. [Effect of multiple micronutrients supplementation on anti-oxidative activity and oxidized DNA damage of lymphocytes in children]. Zhonghua Liu Xing Bing Xue Za Zhi 2005 Apr;26(4):268-272.
41. Xiao Y, Cui J, Shi YH, Sun J, Wang ZP, Le GW. Effects of duodenal redox status on calcium absorption and related genes expression in high-fat diet-fed mice. Nutrition 2010 Nov-Dec;26(11-12):1188-1194.
42. Safar MM, Abdallah DM, Arafa NM, Abdel-Aziz MT. Magnesium supplementation enhances the anticonvulsant potential of valproate in pentylenetetrazol-treated rats. Brain Res 2010 Jun;1334:58-64.
43. Fedirko V, Bostick RM, Long Q, Flanders WD, McCullough ML, Sidelnikov E, et al. Effects of supplemental vitamin D and calcium on oxidative DNA damage marker in normal colorectal mucosa: a randomized clinical trial. Cancer Epidemiol Biomarkers Prev 2010 Jan;19(1):280-291.
44. Küster A, Tea I, Ferchaud-Roucher V, Le Borgne S, Plouzennec C, Winer N, et al. Cord blood glutathione depletion in preterm infants: correlation with maternal cysteine depletion. PLoS One 2011;6(11):e27626.
45. Yang Y, Gao M, Nie W, Yuan J, Zhang B, Wang Z, et al. Dietary magnesium sulfate supplementation protects heat stress-induced oxidative damage by restoring the activities of anti-oxidative enzymes in broilers. Biol Trace Elem Res 2012 Apr;146(1):53-58.
46. Hans CP, Chaudhary DP, Bansal DD. Effect of magnesium supplementation on oxidative stress in alloxanic diabetic rats. Magnes Res 2003 Mar;16(1):13-19.
|