| |
Abstract
Objective: To assess the efficacy and safety of extracorporeal shock wave lithotripsy with Modularis Vario Siemens in the management of patients with renal and ureteral stones.
Methods: Between 2007 and 2009, 225 outpatients were treated with Siemens Modularis Vario lithotripter at Sultan Qaboos University Hospital. Stone size, location, total number of shockwaves, stone-free rate, complications and adjunctive interventions were investigated. Chi-Square and Logistic Regression analyses were used, with p<0.05 set as the level of significance.
Results: Of the 225 initial consecutive patients who underwent extracorporeal shock wave lithotripsy, 192 (85%) had renal stones and 33 (15%) had ureteric stones. The mean±SD stone size was 11.3 ± 4.5 mm, while the mean age of the patients was 39.9 ± 12.8 years with 68.5% males. The mean renal stone size was 11.6 ± 4.7 mm; a mean of 1.3 sessions was required. The mean ureteric stone size was 9.9 ± 3 mm; and a mean of 1.3 sessions was required. Treatment success (defined as complete clearance of ureteric stones, stone-free or clinically insignificant residual fragments of <4 mm for renal stones) was 74% for renal stones and 88% for ureteric stones. Additional extracorporeal shock wave lithotripsy and ureteroscopy were the most adjunctive procedures used for stone clearance. Complications occurred in 74 patients (38.5%) with renal stones and 13 patients (39.4%) with uretetric stones. The most common complication was loin pain (experienced by 16.7% with renal stones and 21% with ureteric stones). Severe renal colic mandating admission occurred in 2% of patients with renal stones and 6% of patients with ureteric stones. In patients with renal stone, steinstrasse occurred in 3.6% and infection post extracorporeal shock wave lithotripsy in 0.5%. Using Multivariate Logistic Regression analysis, factors found to have significant effect on complete stone clearance were serum creatinine (p=0.004) and the number of shockwaves (p=0.021).
Conclusion: Siemens Modularis Vario lithotripter is a safe and effective tool for treating renal and ureteric stones.
Keywords: Extracorporeal shock-wave lithotripsy (ESWL); Kidney; Ureter; Stones.
Introduction
Since its introduction in the 1980s, extracorporeal shock wave lithotripsy (ESWL) has become the standard convenient, noninvasive outpatient procedure used for treatment of renal and proximal ureteric calculi.1 After the introduction of the original electrohydraulic Dornier HM-3 and its high-power delivery, lithotripters have been developed with new sources for generating shock waves, such as electromagnetic and piezoelectric sources. Furthermore, lithotripters have been reduced in size, and now they occupy less space. ESWL focusing and imaging devices have been modified over the years to improve the precise delivery of shock waves to the stone. Despite a decreased power delivery that often implies multiple sessions, second and third-generation machines do not require the use of anesthesia, thus achieving greater patient comfort and tolerance. Few studies have published their experience with the use of the Modularis Vario lithotripter.2 The outcome of ESWL is measured in terms of stone fragmentation and clearance. Failure of ESWL results in unnecessary exposure of renal parenchyma to shock waves and complications, invariably alternative treatments are then needed, incurring additional medical expenses.3 A number of stone characteristics such as fragility, size, location and composition are known to affect outcome.4
Methods
This study aims to assess the safety and efficacy of ESWL with Modularis Vario Siemens for the management of renal and ureteral stone. All patients with renal or ureteric stones, treated at Sultan Qaboos University Hosptial, Oman, using the Modularis Vario lithotripter (Modularis Vario; Siemens, AG Healthcare, Munich, Germany), were recorded retrospectively between May 2007 and November 2009. Complete case-notes and X-rays were evaluated, and follow-up noted in these patients. All patients had complete blood count (CBC), coagulation, Urea and Creatinine, electrolytes (K, Na, Ca), uric acid, coagulation profile (prothrombin time and concentration), urinalysis, urine culture, ECG for elderly and pregnancy test for childbearing women before ESWL. Exclusion criteria; were uncorrected coagulation and bleeding disorders, pregnancy, gross obesity (>120 kg; due to technical difficulty in placing the patient in focus), and obstructed urinary tract distal to the stones. Stone size was determined by the widest diameter for renal and ureteric stones. Stones were categorized according to stone size into ≤10, 11-20 and >20 mm diameter. Pre-treatment plain abdominal films of the kidney, ureter, and bladder (KUB), as well as IVU, ultrasonography or non-contrast-unenhanced CT were used for the initial diagnosis, and KUB and ultrasonography two weeks after each session were used to evaluate fragmentation and clearance. For patient preparation before the procedure, patients taking Aspirin or Warfarin were asked to discontinue them 7 days before ESWL, bowel preparation with Bisacodyl (Dulcolax) 10 mg single oral dose and fasting from midnight before ESWL. Double-J stent was inserted prior to ESWL for stones >2 cm.
The Modularis Vario is a mobile, fully integrated, new generation lithotripter with an electromagnetic shockwave source, and fully integrated fluoroscopic guidance. Energy levels start with E0.1 and gradually increase to a maximum of E8.0 in 38 steps. The average and maximum energy levels, as well as the total energy delivered are automatically shown at the end of each session. Patients were treated while supine; fluoroscopy or ultrasound was used to locate the stone. ESWL settings used were as follows: For the Kidney: Number of shockwaves=3000-3500, Energy level (max)=3-4, Starting: 100 shock waves with Level 0.1-1 Afterwards, maximal level: Lower calyx: 3.0 Upper and middle calyx: 3.5 Pelvis: 4.0 with Frequency SW/min=60. For the Ureter: Number of shockwaves = 3500-4500 Energy level (max)=4 (upper ureter), 6 (lower ureter) with Frequency SW/min Upper and middle ureter=90, Lower ureter=120. All treatments were administered on an outpatient basis for a maximum of three sessions. No fragmentation or residual fragments of >4 mm were considered as a failure and patients were offered alternative treatment. All treatments were carried out using intravenous analgesia in the form of Fentanyl IV (1 ug/kg/dose), Midazolam IV (0.05-0.1 mg/kg) and Granisetron IV when needed (10 ug/kg). The patients were monitored during the procedure by checking the vital signs heart rate (HR), respiratory rate (RR), blood pressure (BP) and Oxygen saturation (pulsoxymetry). At the end of treatment, patients were discharged on oral medications including Diclofenac 50 mg TID, Tamsulosin 0.4 mg OD and Ural 1 sachet BD for 2 weeks.
The stones were re-assessed initially after 10-14 days, using KUB and ultrasound to assess fragmentation. Repeat treatment was applied immediately after follow-up if there was no or inadequate fragmentation of the stone. Patients were followed up for the outcome of stone clearance for up to 3 months after the first ESWL session. The number of shock waves, intensity of shock waves, shock-wave energy, stone-free rate, auxiliary procedure rate, re-treatment rate and complication rate were assessed. Treatment success was defined as complete clearance of ureteric stones, while being stone-free or the presence of clinically insignificant residual fragments of <4 mm were considered as a success for renal stones. The success rate was correlated with the stone size and site. Patient age, sex, site of stone, size of stone, number of shock waves, power, energy delivered, number of sessions, and requirement for auxiliary procedures before or after ESWL were recorded. Chi-Square test was used for statistical evaluation, with the level of significance set as p<0.05. Univariate and Multivariate Binary Logistic Regression analysis were used to determine factors affecting complete stone clearance.
Results
Of the 225 initial consecutive patients who underwent ESWL, 85% (192/225) had renal stones and 15% (33/225) had ureteric stones. The mean±SD (range) stone size in this study was 11.3±4.5 (5-30) mm; 68.5% (154/225) of the patients were male and 31.5% (71/225) were female. The mean±SD (range) age of the patients was 39.9±12.8 (19-80) years. The commonest clinical presentations in this study were renal colic (57.6%, 51.5%) and renal colic with haematuria (20.4%, 36.4%) for renal and ureteric stones, respectively. There were no comorbidities in 80.7% (155/192) of patients with renal stone and 87.8% (29/33) of patients with ureteric stone, with diabetes and hypertension being the most associated comorbidities, if present. The history of previous renal stones, previous ESWL treatment and previous surgery were 63% (121/192), 45.8% (88/192), 18.8% (36/192) in patients with renal stone; and 15% (5/33), 24% (8/33), 18% (6/33) in patients with ureteric stone, respectively. Before ESWL, 34.9% (67/192) had double-J stent and 12% (23/192) had percutaneous nephrostomy tube in place in patients treated for renal stones compared to 36.4% (12/33) having double-J stent in patients treated for ureteric stones. The right side was the commonest side affected with renal stones 51.6% (99/192) and ureteric stones 63.6% (21/33). Renal stones were associated with hydronephrosis in 20.3% (39/192), whereas ureteric stones in 42.4% (14/33). Stone localization was achieved by fluoroscopy in 88% (169/192) of renal stones and 100% (33/33) of ureteric stones. All the patients were treated in the supine position except one patient with ureteric stone was treated in prone.
Of the 192 patients with renal stones, 20% (38/192) had pelvic stones, 14% (27/192) had upper calyceal stones, and 22% (42/192) and 44% (84/192) had middle and lower calyceal stones, respectively. The mean±SD renal stone size was 11.6±4.7 mm. A single session was required in 77.6% (149/192) of patients; the mean (range) number of sessions required for clearance of renal stones was 1.3 (1-3). The necessity for three sessions was non-significantly affected by stone size (p=0.245). However, a higher proportion of stones sized >20 mm (18%) needed three sessions, compared with only 6% of stones sized <10 mm and 2% of stones 11-20 mm in the largest diameter. The mean±SD (range) number of shocks required for renal stone was 2884.5±672 (700-4000). While the mean±SD (range) total energy delivered for renal stones per session was 103.7 ±32 (14-167) J.
In this series, 33 patients had a single ureteric stone, 94% (31/33)of them were in the upper ureter, 3% (1/33) in the middle third and 3% (1/33) in the lower third. The mean±SD ureteric stone size was 9.9±3 mm. The mean±SD (range) number of sessions required for managing ureteric stones was 1.3±0.6 (1-3). When compared with stone size, stones of <10 mm required 3 sessions in 9% of cases, and 4.5% for stones of 11-20 mm (p=0.248). For all ureteric stones, the mean±SD (range) of delivered energy per session was 119.6±48.8 (14-280) J. The highest required energy was for stones in the lower third of the ureter (155 J) and the lowest energy in middle third stones (90 J). The mean±SD number of shocks required per ureteric stone was 3006±802.6.
Table 1: Adjunctive procedure to clear the stone post ESWL.
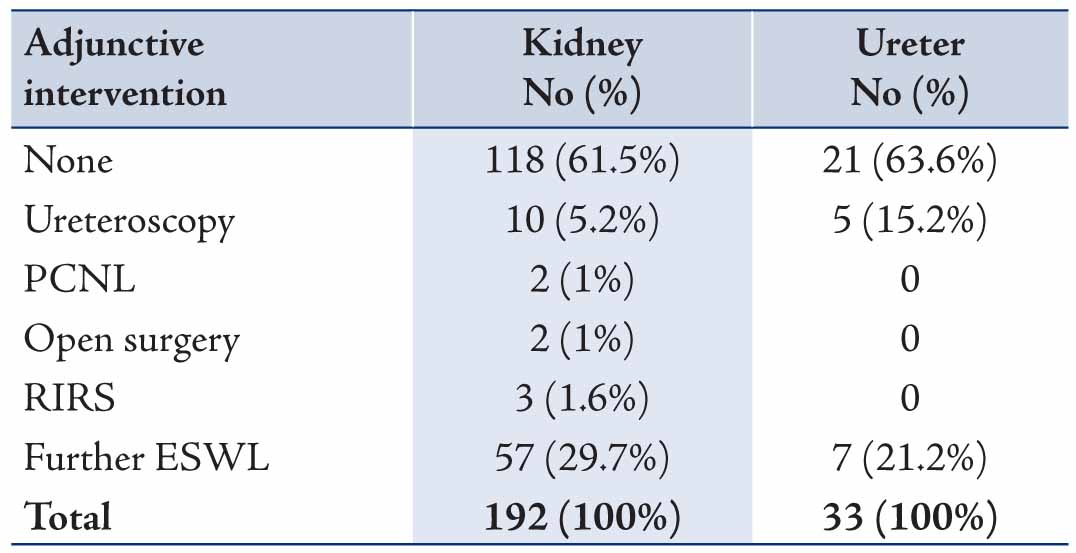
Table 2: Complications observed in the treatment of renal and ureteric stones.
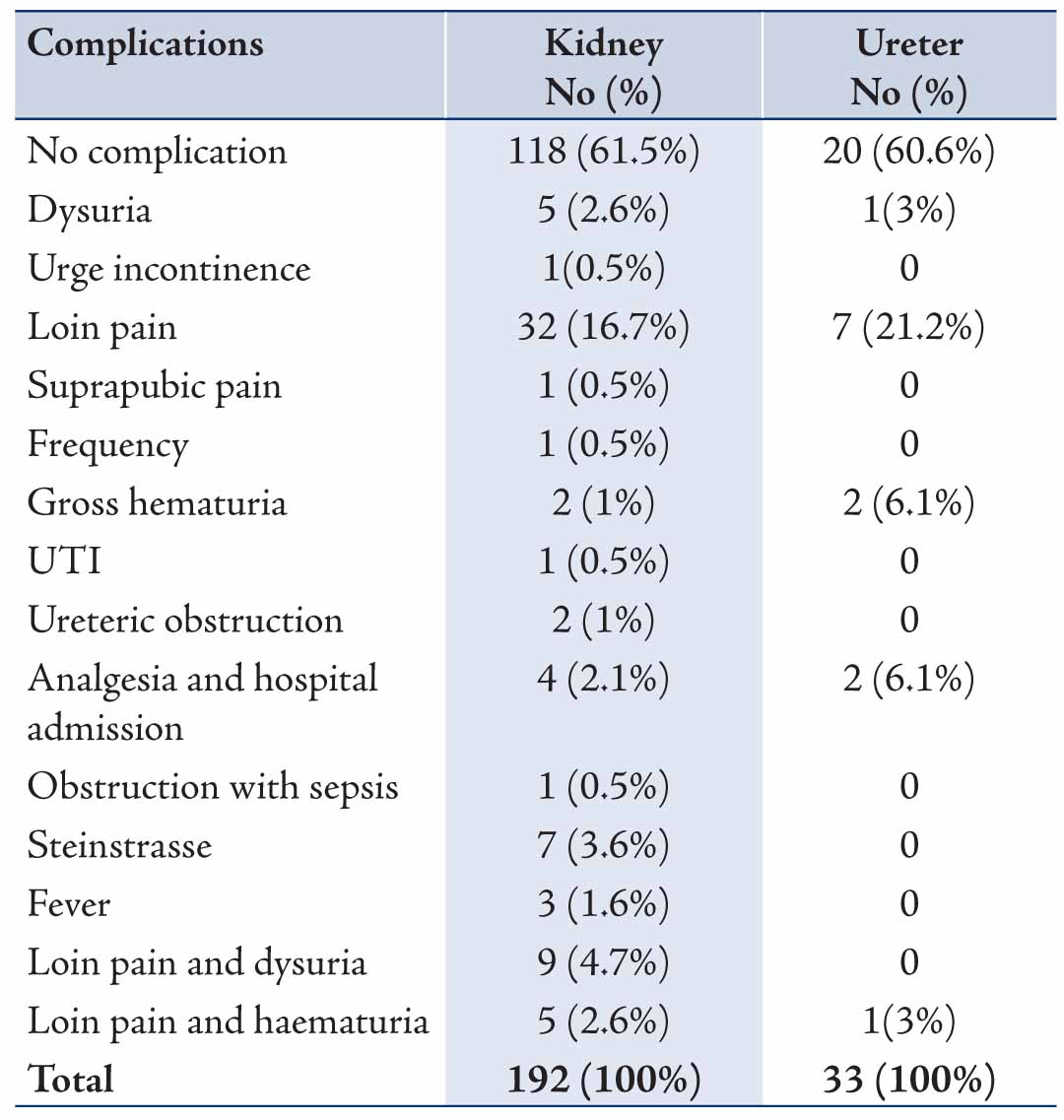
Treatment success (defined as complete clearance of ureteric stones, stone-free or clinically insignificant residual fragments of <4 mm for renal stones) was 74% (142/192) for renal stones and 88% (29/33) for ureteric stones. Additional ESWL and ureteroscopy were the most common adjunctive procedures used for stone clearance (Table 1). The overall treatment complication rate for this study was 38.7% (87/225). For the renal stones, 74 patients (38.5%) had complications, while for the uretetric stones, 13 patients (39.4%) had complications. The majority of the complications were minor with the most common being loin pain 16.7% and 21% in the treatment of renal and ureteric stones, respectively (Table 2). Severe renal colic mandating a visit to the emergency department and admission for control of pain occurred in 2% (4/192) and 6% (2/33) of patients treated for renal stones and ureteric stones, respectively. Steinstrasse (a complication of extracorporeal shock wave lithotripsy for urinary tract calculi in which stone fragments block the ureter to form a "stone street") occurred in 7 (3.6%) patients treated for renal stones: 3 patients had ureteroscopy, 1 had ESWL and 3 patients were treated conservatively.
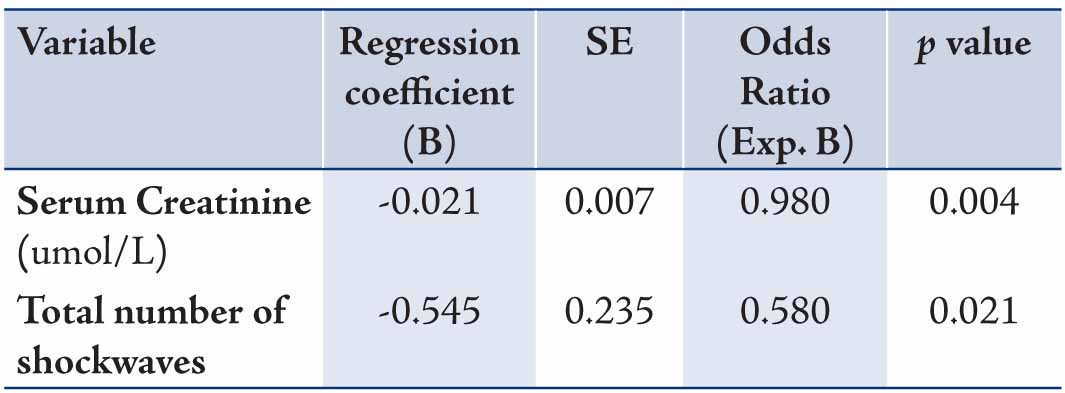
In this series the infection post ESWL was very low 0.5% and 0% in patients treated for renal and ureteric stones, respectively. Using the Univariate Binary Logistic Regression analysis, factors including: age (p=0.113), serum creatinine [umol/L] (p=0.002), total energy (p=0.504), number of shockwaves (p=0.301), stone size [mm] (p=0.739), stone site [renal pelvis, upper, middle or lower calyx] (p=1.0), number of sessions (p=0.006), sex (p=0.093), presence of double-J stent (p=0.754), stone number (single or mutltiple) (p=0.774), side of the stone (p=0.574), presence of hydronephrosis (p=0.175) and complications (p=0.999), were tested for their effect on stone clearance. However, the factors found to have significant effect on the complete stone clearance using the Multivariate Binary Logistic Regression analysis were serum creatinine (0.004) and the number of shockwaves 0.021. (Table 3)
Table 3: Factors affecting complete stone clearance (Multivariate Logistic Regression).
Discussion
The use of ESWL for the treatment of renal stones has brought a revolution in the field of urology. It has not only reduced hospitalization time and morbidity, but is also cost effective. Like any other urological procedure, ESWL is also associated with complications, mainly obstructive and infective. ESWL therapy is noninvasive, anesthesia-free and can be administered in an outpatient setting. Therefore, ESWL remains the first choice for treating renal and upper and middle ureteric stones. The newer generation of lithotripters use smaller focal zones, allowing higher peak-point pressures.5 The Modularis Vario lithotripter has the advantages of greater comfort for the patient during the procedure, better imaging because of the very high quality of the fluoroscopy, and a great comminution of the stone, achieving a success rate of 74% for renal stones and 88% for ureteric stones in our experience, and decreasing the need for auxiliary manoeuvres. These results are comparable with reported success rates of 40-91%.6
The usual limitations of ESWL studies also affect the present study. We failed to examine fragmentation and stone-free rates based exclusively on stone composition. We did not examine the causes of failure, and most patients seen after treatment were evaluated with a KUB or ultrasound methods with inherent diagnostic limitations. However, the cost associated with the reference standard CT after lithotripsy is a problem and, as such, it is rarely used. Chaussy and Bergsdorf,7 stated that a plain abdominal X-ray (KUB) is accepted as the first-line diagnostic method for follow-up examination after stone therapy, but tends to overestimates the stone-free rate. Noncontrast spiral CT seems to be the most sensitive radiological tool for detecting residual fragments after stone therapy.7 Auxiliary procedures were minimal in the present series; the auxiliary treatment rate was similar to what has been reported.8
The overall treatment complication rate of this study is 38.7% (87/225), with the majority being minor complications. No major complications were reported in the present study; however, in other studies, acute renal failure has been reported after ESWL.9 Massive retroperitoneal hemorrhage after extracorporeal shock wave lithotripsy (ESWL) leading to patient death has also been reported.10 Besides renal injury,11 ESWL is not completely free from other serious complications, such as gastrointestinal injury in 1.8% of cases, including colonic perforation or duodenal erosions.12 However, there was no association between ESWL and the subsequent long-term risk of hypertension.13
Double-J (JJ) stent insertion is an important tool in the urologist armamentarium. It has its benefits and complications. Insertion of JJs stent for shockwave lithotripsy of renal calculi may be done as a part of therapy (for obstructive pyelonephritis, renal failure, refractory colic, high grade obstruction) or as a prophylactic stenting before ESWL of renal calculi, which is at best controversial. Currently, European urologist guidelines and the American urologist Association guidelines recommend putting a JJ stent before ESWL for renal pelvic stones of 2 cm and above,14 which was implemented in the present study. A study comparing the outcome of ESWL for a renal pelvic stone measuring 2 cm ± 2 mm with and without JJ stent. With exclusion of patients with renal failure and children, found that Pre ESWL JJ stenting for a 2 cm ± 2 mm renal stone was not beneficial in terms of steinstrasse, fever, stone clearance and number of ESWL sessions. However, ureteric colic was significantly lower in the stented group. Lower urinary tract symptoms (LUTS) were also significantly high in the patients having a JJ stent. The cost of the treatment doubled in the stented group, thus JJ stenting does not prove to be a cost effective procedure when compared to the reduction in complications.15
Renal stone is a common problem in Oman because of our geographical location (Oman lies within the stone belt region extending from Indonesia to Egypt), economic and dietary factors, dehydration, exposure to heat and possible genetic factors.16 The advent of Extra Corporeal Shock Wave Lithotripsy (ESWL) in the 1980s, propelled the treatment of renal stone disease from mainly open surgery into a new era of non invasive procedures. Although the issues of stone density and the type of drinking water were not addressed in the present study, they have been addressed in other studies. Stone types can be estimated by density measurements on computerised tomography (CT). It was reported that it is not reasonable to predict ESWL success with stone densities measured on CT. These densities also cannot predict the number of sessions required during ESWL.17 However, it has been reported that stone density can help to predict the outcome of ESWL, where stones with densities <500 Hounsfield units (HU) are highly likely to result in successful ESWL. Conversely, stone densities3800 HU are less likely to do so.18 There are controversies in the literature regarding the need and the duration of antibiotic prophylaxis in patients with extracorporeal shock wave lithotripsy (ESWL), a recent study was performed to evaluate the efficacy of antibiotic prophylaxis in patients with proven sterile urine before they underwent ESWL and found that the incidence of urinary tract infections after ESWL is extremely low, as also shown by our present study, and prophylaxis antibiotics do not seem to be necessary.19 Previous investigations that attempted to find a correlation between the hardness of water (the molar sum of calcium and magnesium found in water, mg/L) and urolithiasis have yielded to contradictory results. Similarly, there is no consensus on the effects of mineral content of fresh water such as calcium and bicarbonate on the incidence of urinary calculus.20 In a recent study,21 no correlation was found between the incidence of urinary calculus and the amount of calcium, bicarbonate, or the total hardness of drinking water. In contrast, the incidence of urinary calculus was inversely related with drinking water magnesium content.
In the present study Tamsulosin was routinely used post-ESWL. The efficacy of the tamsulosin (oral 0.4 mg/d for 1 month) as an adjuvant therapy to extracorporeal shock wave lithotripsy (ESWL) for the expulsion of ureteral and renal stones was studied in 186 patients (77 ureteral and 109 renal stones).22 It was found that adjuvant treatment with tamsulosin, in addition to standard treatment with steroids and analgesics, significantly improved the stone clearance rate. In addition, Tamsulosin treatment was also associated with a significantly lower interval to the elimination of stone fragments, a significantly lower re-hospitalization rate, and a significantly lower proportion of patients with acute renal colic.
Conclusion
The Siemens Modularis Vario lithotripter is a safe and effective machine for treating renal and ureteric stones. Our initial data from this large, single-centre series shows an acceptable success rate of 74% (142/192) for renal stones and 88% (29/33) 88% for ureteric stones. Therefore, the Modularis Vario is an appropriate and effective tool for treating urinary calculi, especially up to 20 mm in diameter. In the present study, the factors found to have a significant effect on the complete stone clearance were serum creatinine and number of shockwaves.
Acknowledgements
The authors reported no conflict of interest and no funding was received for this work.
References
1. Chaussy C, Brendel W, Schmiedt E. Extracorporeally induced destruction of kidney stones by shock waves. Lancet 1980 Dec;2(8207):1265-1268.
2. Mohamed E. Hassouna SOWSAE-A. Clinical experience with shock-wave lithotripsy using the Siemens Modularis Vario lithotripter. Arab Journal of Urology 2011;9:101-105 .
3. Nomikos MS, Sowter SJ, Tolley DA. Outcomes using a fourth-generation lithotripter: a new benchmark for comparison? BJU Int 2007 Dec;100(6):1356-1360.
4. Bon D, Dore B, Irani J, Marroncle M, Aubert J. Radiographic prognostic criteria for extracorporeal shock-wave lithotripsy: a study of 485 patients. Urology 1996 Oct;48(4):556-560, discussion 560-561.
5. Augustin H. Prediction of stone-free rate after ESWL. Eur Urol 2007 Aug;52(2):318-320.
6. Jamshaid A, Ather MH, Hussain G, Khawaja KB. Single center, single operator comparative study of the effectiveness of electrohydraulic and electromagnetic lithotripters in the management of 10- to 20-mm single upper urinary tract calculi. Urology 2008 Nov;72(5):991-995.
7. Christian C, Thorsten B. The preferred treatment for upper tract stones is extracorporeal shock wave lithotripsy (ESWL) or ureteroscopic: pro ESWL. Urology 2009 Aug;74(2):259-262.
8. Lalak NJ, Moussa SA, Smith G, Tolley DA. The Dornier Compact Delta lithotripter: the first 150 ureteral calculi. J Endourol 2002 Nov;16(9):645-648.
9. Schmitt R. BJSA. Akutes Nierenversagen nach extra-korporaler Stoßwellenlithotripsie. Nephrologe 2011;6:439-442 .
10. Inoue H, Kamphausen T, Bajanowski T, Trübner K. Massive retroperitoneal haemorrhage after extracorporeal shock wave lithotripsy (ESWL). Int J Legal Med 2011 Jan;125(1):75-79.
11. Bergsdorf T, Thüroff S, Chaussy Ch. The isolated perfused kidney: an in vitro test system for evaluation of renal tissue damage induced by high-energy shockwaves sources. J Endourol 2005 Sep;19(7):883-888.
12. Maker V, Layke J. Gastrointestinal injury secondary to extracorporeal shock wave lithotripsy: a review of the literature since its inception. J Am Coll Surg 2004 Jan;198(1):128-135.
13. Krambeck AE, Rule AD, Li X, Bergstralh EJ, Gettman MT, Lieske JC. Shock wave lithotripsy is not predictive of hypertension among community stone formers at long-term followup. J Urol 2011 Jan;185(1):164-169.
14. European Association of urology. [Home page of European Association of Urology] [Online]. [Cited December 2011] Available from URL: http://www.uroweb.org/. 2011. 11-12-2011.
15. Mohayuddin N, Malik HA, Hussain M, Tipu SA, Shehzad A, Hashmi A, et al. The outcome of extracorporeal shockwave lithotripsy for renal pelvic stone with and without JJ stent–a comparative study. J Pak Med Assoc 2009 Mar;59(3):143-146.
16. Hussain M. LMABSANSAHR. Urolithiasis in Sindh: a single centre experience with a review of 10,000 cases. J Nephrol Urol Transplant 1998;1:10-13.
17. Goren MR. Buoctmiploh. Can we predict the success of shockwave lithotripsy by stone density measured with computerised tomography. Eur Urol Suppl 2006;5:186 .
18. Sanjeev Pathaka. Radiological determination of stone density and skin-to-stone distance-Can it predict the success of extracorporeal shock wave lithotripsy? Br J Med Surg Urol 2009;2:180-184 .
19. Basiri AS, Shakhssalim N, Khoshdel AR, Pakmanesh H, Radfar MH. Drinking water composition and incidence of urinary calculus: introducing a new index. Iran J Kidney Dis 2011 Jan;5(1):15-20.
20. Caudarella R, Rizzoli E, Buffa A, Bottura A, Stefoni S. Comparative study of the influence of 3 types of mineral water in patients with idiopathic calcium lithiasis. J Urol 1998 Mar;159(3):658-663.
21. Basiri A, Shakhssalim N, Khoshdel AR, Pakmanesh H, Radfar MH. Drinking water composition and incidence of urinary calculus: introducing a new index. Iran J Kidney Dis 2011 Jan;5(1):15-20.
22. Georgiev MI, Ormanov DI, Vassilev VD, Dimitrov PD, Mladenov VD, Popov EP, et al. Efficacy of tamsulosin oral controlled absorption system after extracorporeal shock wave lithotripsy to treat urolithiasis. Urology 2011 Nov;78(5):1023-1026.
|
|