Right atrial myxoma extending to the inferior vena cava (IVC) with right-to-left shunting resulting in systemic desaturation is rare. The correlation between myxoma and significant right-to-left shunting at the atrial level is not common.1 Here, we present a right atrial myxoma with IVC extension with cyanosis in a 45-year-old female.
Case report
A 45-year-old female was referred to our center with symptoms of shortness of breath, easy fatigability, generalized weakness, and bluish discoloration of lips, fingers, and skin lasting about four months. On general examination, patient was malnourished and thin-built. Central cyanosis was present. On auscultation grade III/IV diastolic murmur was audible at the tricuspid region. Other systems were normal.
Polycythemia was detected in a routine blood investigation. Arterial blood gas analysis showed PO2 of 32 mmHg and SpO2 of 68% at room air and 72% on oxygen (nasal prong/face mask). Chest X-ray revealed no abnormalities. The diagnosis of right atrial mass was confirmed using 2D-transthoracic echocardiography [Figure 1] but the reason for cyanosis could not be explained. A tumor thrombus in a branch of the right lower pulmonary artery with a small locoregional pulmonary infarct along with right atrial myxoma was reported in computed tomography (CT) angiography of heart and great vessels and CT pulmonary angiography (done at another institution). A cardiac catheterization study was not possible due to the ongoing COVID-19 pandemic and institutional COVID-19 testing protocol. We still had a diagnostic dilemma between right atrial myxoma with right-to-left shunting and pulmonary thromboembolism.
 Figure 1: 2D-transthoracic echocardiography showing right atrial mass (red arrow).
Figure 1: 2D-transthoracic echocardiography showing right atrial mass (red arrow).
We planned surgical resection of the myxoma on an earlier basis. On-table intraoperative transesophageal echocardiography done under anesthesia, showed patent foramen ovale (PFO) with right-to-left shunting because of raised right atrial pressure and dynamic obstruction of the tricuspid valve by the right atrial myxoma. Our approach was via median sternotomy. Standard aorto-bicaval cannulation was done. Cardiopulmonary bypass was established. The myxoma was pedunculated and it was attached to anteromedial aspect of the right atrial-IVC junction with extension to IVC [Figure 2]. The myxoma was resected via trans-right atrial approach. IVC extension of the tumor was removed by going into total circulatory arrest. The PFO was closed primarily [Figure 3]. The surgical specimen was sent for histopathological examination and was found to be a myxoma.
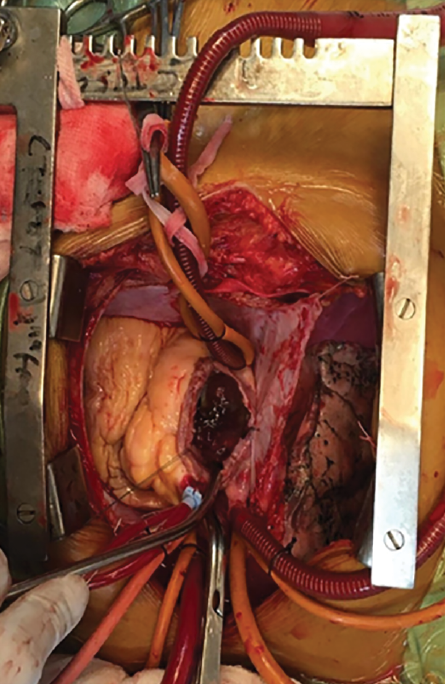 Figure 2: The right atrial myxoma.
Figure 2: The right atrial myxoma.
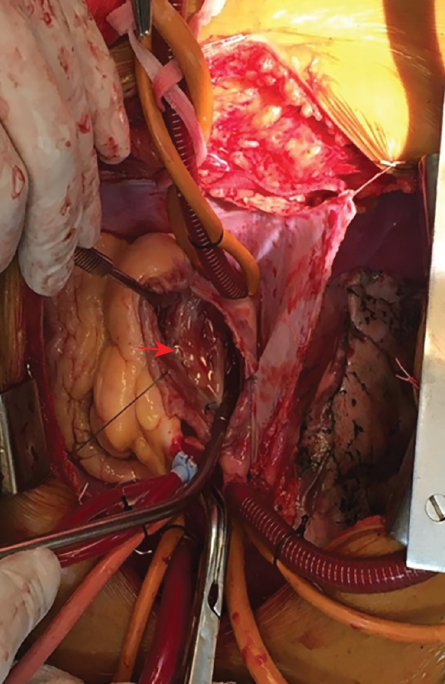 Figure 3: Patent foramen ovale (red-arrow).
Figure 3: Patent foramen ovale (red-arrow).
Discussion
Myxomas are the most encountered primary cardiac tumor in adults; the left atrium is the most common site. Right atrial myxomas are more sessile and solid than left atrial myxomas, with wider attachment to the septum or atrial wall. Left atrial myxomas produce symptoms of dyspnea and hemoptysis resembling features of mitral stenosis, commonly of short duration, episodic, and with syncope, and rapidly progressive to heart failure. Right atrial myxomas may present with episodic symptoms and may progress rapidly. Abdominal distension from hepatomegaly and ascites and peripheral edema are often presenting complaints. Embolic manifestations are neurologic deficits, coldness and pain in an extremity, angina (coronary), and dyspnea (pulmonary). Constitutional symptoms are often subtle or even absent when the tumor bulk is small, but occasionally become the only presenting symptom complex.2 A review of 312 cases of right and left atrial myxomas revealed that only two were associated with atrial septal defect.3 Natarajan et al,4 reported one case. Right atrial myxoma is rare and the usual signs are right-sided heart failure and pulmonary embolism.5 The association between a myxoma and significant right-to-left shunting at atrial level in adults is exceedingly rare.1 Our patient was cyanotic at the time of presentation because of the right-to-left shunting at the level of atria via PFO because of raised right atrial pressure in the background of dynamic obstruction of the tricuspid valve by the right atrial myxoma.
Conclusion
This rare correlation between myxoma and cyanosis must be kept in mind or it will create diagnostic dilemma and undue confusion while managing this subset of patients.
Disclosure
The authors declared no conflicts of interest. Written informed consent was obtained from the patient.
references
- 1. Chamsi-Pasha MA, Anwar AM, Nosir YF, Abukhudair W, Ashmeg A, Chamsi-Pasha H. Right atrial myxoma associated with an atrial septal defect by real-time three-dimensional echocardiography. Eur J Echocardiogr 2009 Mar;10(2):362-364.
- 2. Kirklin J, Blackstone E. Kirklin/Barratt-Boyes cardiac surgery. 4th ed; 2013.
- 3. Newman HA, Cordell AR, Prichard RW. Intracardiac myxomas. Literature review and report of six cases, one successfully treated. Am Surg 1966 Apr;32(4):219-230.
- 4. Natarajan P, Vijayanagar RR, Eckstein PF, Bognolo DA, Toole JC. Right atrial myxoma with atrial septal defect: a case report and review of the literature. Cathet Cardiovasc Diagn 1982;8(3):267-272.
- 5. Murayama H, Tamaki S, Kato N, Yuji N, Yokote J, Mutsuga M, et al. Right atrial myxoma associated with atrial septal defect: a case report and review of the literature. Ann Thorac Cardiovasc Surg 2001 Jun;7(3):166-169.