Modern college life imposes multiple stressors on students. These include academic pressure, social media pressure, sexual tensions, pressure to win, rivalry with peers, paucity of leisure time, long hours in front of electronic screens, poor sleep quality and duration, decreased time spent with families, anxiety about higher studies and employment prospects, and financial constraints.1 Such stressors can be particularly problematic for college students in developing countries such as India with no reliable social security systems. The impact of these stressors on students varies greatly. On the one end of the spectrum are students who thrive on such stressors, and on the other are those who develop chronic stress, anxiety, and depression, leading to poor quality of life (QoL).
Stress can be described as the multi-system response of the body to any threat that overwhelms or is considered likely to overwhelm selective homeostatic reaction mechanisms.2 According to the American Association of Anxiety and Depression, 70% of adults in the US claim to experience mild to moderate stress, which is particularly prevalent among college students.3 The consequence of sustained stress over time manifest most often as chronic anxiety and depression. The World Health Organization (WHO) has indicated depression as the principal cause of disability in the world. This has been reported to affect over 280 million people worldwide and one in seven college students. Depressed students may feel a variety of negative effects that diminish their QoL, such as intense exhaustion, remorse, and despair.4 In India, depression affects roughly two-fifths of the medical undergraduates while stress affects more than half of the students.5 It is also associated with anxiety.6
The psychological costs of modern life have increased the demand and supply of a wide spectrum of therapies.7 Pharmacological interventions are popular but not always effective and some have adverse effects; therefore research is increasingly turning to noninvasive alternatives.8 Several complementary and alternative treatment systems have been found to mitigate moderate depression.9 It is known that a healthy lifestyle that includes regular physical exercise and healthy diet improves symptoms of depressive disorders.10,11 Physical exercise is also suggested as an affordable, low-cost, non-pharmacological treatment for depression and an overall booster of QoL.12
The physical benefits of training on a whole-body vibrating (WBV) platform have been investigated and endorsed and it has lately been adopted in many health and wellness centers as an enhanced form of workout. However, the psychological benefits of WBV is still an emerging research field. The available evidence suggests that WBV training may have a beneficial effect on depression in normal individuals.13–15 Modern antidepressants, being selective serotonin reuptake inhibitors, reduce depression by increasing serotonin availability. The outcomes of exercise on blood serotonin concentrations are comparable to those of selective serotonin reuptake inhibitors, which explains its antidepressive effect.16
Severe depression is reported to be associated with hypercortisolemia which leads to lower immunity to infections.17 After the WBV treatment, cortisol levels decreased significantly in subjects, and it also induced an increased concentration of blood testosterone and growth hormone levels.18 The impact of physical exercise on depressive symptoms in healthy individuals (i.e., those who are within the normal range for depressive symptoms) has received limited recognition.12 Therefore, this study aims to find whether WBV training as an external exercise method is capable of enhancing psychosocial factors in college students.
Methods
A total of 50 college students of both sexes were checked for eligibility on the Depression, Anxiety Stress Scale (DASS) (depression > 10, anxiety > 8, stress > 15). Exclusion criteria required non-inclusion of those involved in any routine exercises, taking medication for mental health, having any lower limb prosthesis, history of any orthopedic injury, or neurological disorders like neuropathy or seizures. Eight students did not fulfill the criteria, and 12 declined to participate due to their schedules. Thus, 30 students (male = 9, female = 21) were included in the study. Their mean age was 24.1±1.2 years and the body mass index was 21.5±3.4 kg/m2. Demographic details are shown in Table 1. Ethical approval was taken from the Institutional Ethical Committee of Jamia Millia Islamia, reference no.: 26/11/263/ JMI/IEC/2019. Written informed consent was taken from each participant. The allocation of the participants was done by computer randomization method, and the participants were blinded and allocated to either of the two equal groups: WBV group (n = 15) or exercise group (n = 15) [Figure 1].
Table 1: Comparison of demographic characteristics and outcome variables at baseline.
|
Age, year
|
24.0 ± 1.2
|
24.3 ± 1.3
|
-
|
|
Sex, male/female
|
6/9
|
3/12
|
-
|
|
Height, cm
|
165.8 ± 8.9
|
160.6 ± 9.8
|
-
|
|
Weight, kg
|
60.0 ± 11.4
|
56.0 ± 14.7
|
-
|
|
BMI, kg/m2
|
21.6 ± 2.9
|
21.5 ± 3.9
|
-
|
|
DASS
|
|
|
|
|
Depression
|
19.4 ± 9.1
|
15.9 ± 6.6
|
0.230
|
|
Anxiety
|
15.5 ± 7.3
|
12.1 ± 5.6
|
0.170
|
|
Stress
|
23.4 ± 7.8
|
20.7 ± 6.2
|
0.310
|
|
SF-36
|
|
|
|
|
General health
|
55.2 ± 22.6
|
56.1 ± 18.4
|
0.910
|
|
Physical functioning
|
83.0 ± 12.5
|
70.6 ± 17.7
|
0.030*
|
|
Role limitation due to physical health
|
58.3 ± 36.1
|
25.0 ± 31.3
|
0.010*
|
|
Role limitation due to emotional problems
|
37.7 ± 30.5
|
15.5 ± 30.5
|
0.030*
|
|
Social functioning
|
55.0 ± 23.0
|
59.1 ± 12.0
|
0.540
|
|
Pain
|
67 .0 ± 21.8
|
55.6 ± 21.1
|
0.160
|
|
Energy/fatigue
|
47.3 ± 16.9
|
44.6 ± 12.1
|
0.625
|
WBV: whole-body vibration; BMI: body mass index; DASS: Depression Anxiety Stress Scale; SF-36: Medical Outcomes Study Short Form 36.
*Significant difference between the groups.

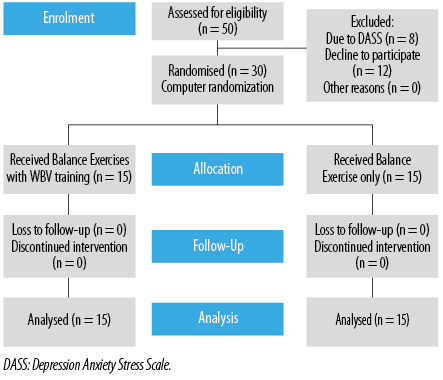 Figure 1: Flow chart of the study.
Figure 1: Flow chart of the study.
Baseline measurements of DASS and the Medical Outcomes Study Short Form 36 (SF-36) were taken for all participants. A familiarization session was given after the randomization. The warm-up session included five minutes of jogging and stretching the lower limb muscles. The participants in the WBV group performed exercises on the vibration platform, and participants in the exercise group performed the same exercises but without vibration.
The equipment used to produce WBV was Whole Body Vibrating Platform KH 75 unit manufactured by Crazy Fit VIVA Fitness, India. The unit has a horizontal rectangular platform (53 × 37 cm) with supporting bars for holding with both hands. The platform is mechanically vibrated whose intensity was chosen based on recommendations in the literature. For the current study, the frequency was fixed at 30 Hz with 2 mm amplitude. The frequency level was chosen with the understanding that > 20 Hz might evoke muscular relaxation, while ≥ 50 Hz could cause muscle soreness and unpleasant sensations.19 The participants were asked to grip the supporting bars while standing on the platform.
Participants in the WBV group performed (a) static squat at 100° of knee flexion, (b) dynamic squat between 90° and 130° knee flexion for each leg, (c) dynamic squat from 90° to 130° of knee flexion for both legs, and (d) squat at 100° of knee flexion, shifting body weight from one leg to another, while standing on the vibrating platform. They were required to maintain each squat position for 30 seconds with 30 seconds of rest between each squat. Three sets of each exercise were performed with three minutes rest between each set. In the exercise group, participants performed the same set of exercises on the leveled surface without vibration.
At the end of each session, a cool-down period was given, including a self-paced slow walk for at least 5 minutes. The duration of the intervention was four weeks, two sessions per week, after which the DASS and the SF-36 scoring were done for each participant.
The DASS is a 42-item summary of three self-reporting interventions that measure the negative emotional symptoms of depression, anxiety, and stress. The scale consists of 14 items, separated into two to five subscales of similar content. Respondents use a 4-point intensity scale to measure the degree to which they have undergone each condition during the past week. The score results of depression, anxiety, and stress are calculated by adding the points for each relevant scale. The reliability scores of the scales in terms of Cronbach’s alpha scores rate the depression scale at 0.91, the anxiety scale at 0.84, and the stress scale at 0.90 in the normative sample.20,21
SF-36 involves eight domains of general health: physical function, social function, role-emotional, role-physical, mental health, vitality, pain, and general health. The maximum score in each domain is 100, and a high score is desirable and indicative of better well-being or less pain. Changes in the score of five units are clinically relevant.22 SF-36 has shown consistently high levels of reliability (test-retest, and internal consistency) and validity (content, concurrent, criterion, construct, and predictive).23
We calculated the optimum number of participants using software G*Power version 3.1.9.2 following the methodology adopted by Atlantis et al,24 where the pre (10.6±8.8) and post (4.0±3.4) stress scores were analyzed by using the difference between two dependent means (matched pairs) and effect size came out to be 0.858. A total of 30 subjects (15 subjects in each group), including 15% dropouts, were shown to be necessary with the effect size of 0.858, α = 0.05, and power (1-β) = 0.80.
Data were analyzed with SPSS (IBM Corp. Released 2015. IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp.). The normality distribution of all outcome measures was verified using the Shapiro-Wilk test, skewness, and histogram. The outcome variables which show non-normal distribution were analyzed using a non-parametric test or log-transformed. Baseline measures and demographic variables between the two groups were determined using the independent sample t-test or Mann-Whitney U test. A 2 × 2 repeated measure analysis of variance was used for outcome measures to find out between-group effect (Exercise group and WBV group), within-group effect (pre-values and post-values), and time × intervention interaction effect. If the baseline measures between groups were found to be significant, then 2 × 2 repeated measure analysis of covariance was used, considering pre-values as covariate. In addition, the change between the pre and post-values was analyzed using the independent t-test to find out the significant difference between the groups. All comparisons were considered significant at p ≤ 0.050, and the CI was set at 95%.
Results
A total of 50 participants were assessed for eligibility. Eight were excluded due to higher scores on DASS, and 12 participants declined to participate. Of the 30 participants included, 21 were female (70.0%), and nine were male (30.0%). There were 12 women and three men in the WBV group and nine women and six men in the exercise group.
Depression, anxiety, and stress were non-significant at baseline (p > 0.050). The physical functioning component of SF-36 was significant at baseline comparison between the groups (p = 0.040) [Table 1]. Role limitation due to physical health (p = 0.010) and emotional problems (p = 0.030) was analyzed using the Mann-Witney U test showed a significant difference between the groups at baseline [Table 1].
Depression (F(1,28) = 95.28, p < 0.001), anxiety (F(1,28) = 45.58, p < 0.001), and stress (F(1,28) = 30.81, p < 0.001) were found to be significant for within-group effects while between-group effect was found to be non-significant for all components of DASS. Time × intervention interaction effect was found significant for depression (F(1,28) = 10.58, p = 0.003) and stress (F(1,28) = 4.96, p = 0.030), whereas anxiety F(1,28) = 2.46, p = 0.120) showed non-significant [Table 2]. The change (pre-post) in depression (p = 0.003) and stress (p = 0.034) was found to be significant difference whereas the anxiety (p = 0.128) showed non-significant difference between exercise and WBV groups [Table 2].
General health (F(1,28) = 44.18, p < 0.001), physical functioning (F(1,27) = 181.58, p < 0.001), role limitations due to physical health (F(1,27) = 151.9, p < 0.001), role limitations due to emotional problems (F(1,27) = 169.68, p < 0.001), social functioning (F(1,28) = 62.31, p < 0.001), pain (F(1,28) = 103.36, p < 0.001), energy/fatigue (F(1,28) = 129.73,
p < 0.001), and emotional well-being (F(1,28) = 114.8, p < 0.001) were found to be significant for within group effect whereas between group effect was found to be non-significant for all SF-36 component except role limitation due to emotional problems (F(1,27) = 5.43, p = 0.040) [Table 3]. Time × intervention interaction effect was found to be significant only for role limitations due to physical health (F(1,27) = 5.42, p = 0.030), energy/fatigue (F(1,28) = 8.84, p = 0.006), and emotional wellbeing (F(1,28) = 7.52, p = 0.010) (Table 3). Role limitations due to physical health (p < 0.001), role limitations due to emotional problems (p = 0.050), energy/fatigue (p = 0.007), and emotional well-being (p = 0.010) were significantly different between the exercise and WBV group whereas other domains of SF-36 were non-significant between the groups.
Table 2: Comparison of DASS scores at baseline (pre) and after four weeks (post) of intervention.
|
Depression
|
|
|
|
|
|
|
|
Pre
|
19.4 ± 9.1
|
15.9 ± 6.6
|
|
0.77 (< 0.001)*
|
0.09 (0.09)
|
0.27 (0.003)*
|
|
Post
|
16.5 ± 8.16.5 ± 8.7
|
10.0 ± 7.2
|
|
|
Pre-post (Change)
|
2.9 ± 1.9
|
5.8 ± 2.8
|
3.25 (0.003)*
|
|
|
|
|
Anxiety
|
|
|
|
|
|
|
|
Pre
|
15.5 ± 7.3
|
12.1 ± 5.6
|
|
0.61 (< 0.001)*
|
0.10 (0.08)
|
0.08 (0.120)
|
|
Post
|
12.9 ± 7.2
|
8.0 ± 5.4
|
|
|
Pre-post (Change)
|
2.5 ± 1.9
|
4.0 ± 3.2
|
1.56 (0.128)
|
|
|
|
|
Stress
|
|
|
|
|
|
|
|
Pre
|
23.4 ± 7.8
|
20.7 ± 6.2
|
|
0.52 (< 0.001)*
|
0.10 (0.07)
|
0.15 (0.030)*
|
|
Post
|
20.6 ± 6.1
|
14.3 ± 7.9
|
|
DASS: Depression Anxiety Stress Scale; WBV: whole-body vibration.
Table 3: Comparison of values of SF-36 at baseline and after four weeks of intervention.
|
General health
|
|
|
|
|
|
|
|
Pre
|
55.2 ± 22.6
|
56.1 ± 18.4
|
|
0.61 (< 0.001)*
|
0.04 (0.280)
|
0.11 (0.060)
|
|
Post
|
69.4 ± 21.3
|
81.9 ± 8.4
|
|
|
|
|
|
Post-pre (Change)
|
14.1 ± 16.9
|
25.83 ± 15.9
|
1.93 (0.063)
|
|
|
|
|
Physical functioning
|
|
Pre
|
83.0 ± 12.5
|
70.6 ± 17.7
|
|
0.87 (< 0.001)*
|
0.0001 (0.990)
|
0.0001 (0.990)
|
|
Post
|
95.3 ± 6.9
|
92.6 ± 6.5
|
|
|
|
|
|
Post-pre (Change)
|
12.3 ± 10.1
|
22.0 ± 15.9
|
1.98 (0.057)
|
|
|
|
|
Role limitation due to physical healtha
|
|
Pre
|
58.3 ± 36.1
|
25.0 ± 31.3
|
|
0.89 (< 0.001)*
|
0.09 (0.200)
|
0.24 (0.030)*
|
|
Post
|
83.3 ± 27.8
|
88.3 ± 18.5
|
|
|
|
|
|
Post-pre (Change)
|
25.0 ± 23.1
|
63.3 ± 29.6
|
3.94 (< 0.001)*
|
|
|
|
|
Role limitation due to emotional problemsa
|
|
Pre
|
37.7 ± 30.5
|
15.5 ± 30.5
|
|
0.93 (< 0.001)*
|
0.33 (0.040)*
|
0.09 (0.310)
|
|
Post
|
68.8 ± 38.7
|
64.4 ± 29.4
|
|
|
|
|
|
Post-pre (Change)
|
31.1 ± 15.2
|
48.8 ± 30.5
|
2.01 (0.050)*
|
|
|
|
|
Social functioning
|
|
|
|
|
|
|
|
Pre
|
55.0 ± 23.0
|
59.1 ± 12.0
|
|
0.69 (< 0.001)*
|
0.06 (0.160)
|
0.07 (0.130)
|
|
Post
|
74.1 ± 24.7
|
87.5 ± 9.4
|
|
|
|
|
|
Post-pre (Change)
|
19.1 ± 21.5
|
28.3 ± 8.7
|
1.52 (0.139)
|
|
|
|
|
Pain
|
|
|
|
|
|
|
|
Pre
|
67.0 ± 21.8
|
55.6 ± 21.1
|
|
0.78 (< 0.001)*
|
0.06 (0.180)
|
0.05 (0.200)
|
|
Post
|
87.6 ± 15.0
|
82.3 ± 11.5
|
|
|
|
|
|
Post-pre (Change)
|
20.6 ± 11.7
|
26.6 ± 13.6
|
1.28 (0.208)
|
|
|
|
|
Energy/fatigue
|
|
|
|
|
|
|
|
Pre
|
47.3 ± 16.9
|
44.6 ± 12.1
|
|
0.82 (< 0.001)*
|
0.02 (0.370)
|
0.24 (0.006)*
|
|
Post
|
66.6 ± 18.2
|
77.6 ± 5.6
|
|
|
|
|
|
Post-pre (Change)
|
19.3 ± 15.7
|
33.0 ± 8.1
|
2.97 (0.007)*
|
|
|
|
|
Emotional well being
|
|
Pre
|
49.8 ± 19.8
|
54.1 ± 14.4
|
|
0.80 (< 0.001)*
|
0.09 (0.100)
|
0.21 (0.010)*
|
|
Post
|
66.1 ± 21.7
|
81.6 ± 9.4
|
|
|
|
|
WBV: whole-body vibration; DASS: Depression Anxiety Stress Scale; SF-36: Medical Outcomes Study Short Form 36 .
aanalyses were done using log transformed values;*Significant difference.
Discussion
The study’s main objective was to compare the effects of exercise with WBV and exercise without WBV on depression, anxiety, and stress and the overall QoL in college students. There were no baseline differences between the groups in the domains of DASS (depression, anxiety, and stress) or SF-36 except for physical functioning, role limitation due to physical health, and role limitation due to emotional problems.
After four weeks of intervention, there was improvement in all the components of DASS and SF-36 in both the WBV and exercise groups. We found more significant improvement in the WBV group in comparison with the exercise group for depression, stress, role limitations due to physical health, role limitations due to emotional problems, energy/fatigue, and emotional wellbeing.
In contrast to our results, Aksoy13 reported the difference between both the WBV training group’s pre- and post-test scores and the control group’s post-test Beck Depression Inventory scores at the end of the 12th week as being statistically significant. It was ascertained that consistent 12-week WBV training was effective in lowering the symptoms of depression. He observed that as short sessions of WBV were beneficial, the technique could be used to minimize depression rates among those with low exercise motivation.
According to our findings, there was a significant difference between the pre- and post-test scores of both groups. However, there was no statistically significant difference in the post-test depression scores between the WBV and exercise groups. This could be attributed to the reduced training duration of four weeks only.
Parallel to our findings, Wunram et al,14 reported that aerobic exercise (endurance cycling) and WBV training were both beneficial for depressed adolescents and were preferable to mainstream therapy. They found the easy-to-perform strength conditioning with WBV had results comparable to the more rigorous cycling program. As per Carter,25 more passive training will be necessary when the depressive symptoms become more severe. Wunram et al,14 also reported that the WBV group felt more motivated than the cycling group to continue exercising even after the experiment had ended. So, this type of training seems to be feasible as part of everyday routine for young people. This suggests that the shorter the exercise time needed to produce beneficial effects, the more the motivation to train further. This should be positive for WBV as it takes only a few minutes and is easy to perform. Thus, WBV could be used as a ‘bridging’ technique when more active exercise due to the depressive condition is still not possible.
According to Smits et al,26 there is significant correlation between physical inactivity and susceptibility to anxiety, possibly due to increased emotional sensitivity in inactive people to bodily perceptions that aid in sustaining panic disorder. In a research conducted by Wipfli et al,16 both the study group (who were assigned aerobic exercises) and the control group (who did only stretching exercises) achieved reduction in anxiety. Though the aerobic exercise group did achieve better anxiety reduction, the difference was not statistically significant. A systematic review concluded that exercise alone was less effective than antidepressant therapy, but beneficial as an adjunctive intervention for anxiety disorders, and that both aerobic and non-aerobic activities may reduce signs of acute anxiety.27 According to our findings, there was a significant difference between the pre- and post-test scores of both training groups, but the difference in the post-test depression scores between the WBV and exercise group was not statistically significant. A caveat is Rebar et al’s28 finding that exercise was correlated with anxiety reduction in healthy people, but not in clinically diagnosed anxiety cases.
Research into exercise and stress has usually concentrated on aerobic exercises. Various studies have consistently reported that participants felt more relaxed after a 20–30 minutes aerobic workout and the relaxation lasted many hours thereafter.29 Human and animal studies revealed physical activity facilitates optimal response to stress hormones and increases the availability of neurotransmitters such as serotonin and dopamine that influence mood and behavior.30
Arslan et al,31 reported that depression was widespread among Turkish university students, negatively affecting their health-related QoL (HRQoL). Niemeier et al,32 revealed that negative correlations existed between depression and QoL in students. Similar to our findings, pre-intervention DASS scores were quite high in our cohort, and as seen in earlier studies their SF-36 results were poor. Post-intervention there were significant differences in the DASS scores in two domains (depression and stress) within time and group, and in anxiety with time. QoL improved in all domains of SF-36 with time and four domains improved significantly within the group (role limitation due to physical health, role limitation due to emotional problems, energy/fatigue, and emotional well-being).
Olivares et al,33 conducted a 12-week course of WBV therapy (on a tilting platform) for 21 sedentary middle-aged women with fibromyalgia. They experienced significant improvement in HRQoL compared to the control group. The beneficial results of WBV may have been partially due to a ‘reconditioning’ effect of the vibration on their sedentary musculature. The long 12-week long duration of the treatment may have helped compared to our four-week-long course. However, any relative advantage of the tilting platform to our horizontal one is not known, calling for studies that compare the two methods. The researchers concluded that WBV was a cost-effective treatment, deserving increased attention from political decision-makers to make it part of health and social policies.
In elderly patients with falling risk, Bruyere et al,34 found that controlled WBV can reduce such risk and improve HRQoL. With the vibration intervention, there was improvement in the physical function measurement and was well correlated with the Timed Up and Go test. However, there was no improvement in the intervention group from baseline in the health change component. Similarly, in the present study, physical functioning was the only domain of SF-36 which improved significantly between the groups and with the time that can be because of effects on muscular performance. Álvarez-Barbosa et al,35 also reported enhanced physical balance and QoL among their elderly subject post WBV training. In elderly patients, as more motor units are triggered in reaction to the vibration stimuli (tonic vibration stimulus), strong neuromuscular responses may be expected to occur. WBV enhances biomechanical variables such as muscle power, flexibility, and strength, resulting in a positive impact on the dynamic efficiency (as demonstrated by the improvements in lower limb muscle performance and the improvements shown in the study’s Timed Up and Go score). All these factors may have together improved the QoL.
Alev et al,36 found in their study on fibromyalgia patients that Fibromyalgia Impact Questionnaire score was significantly higher than visual analog scale and Beck Depression Inventory at the 6th month of WBV training. It may have happened because WBV can be readily practiced by untrained people with minimal training compared to conventional exercises. Pain relief may be a consequence of the neuronal adaptive response to the vibrational impulse. Fibromyalgia Impact Questionnaire was the only variable in the study which showed significant changes after three months and longer duration training effect or residual effect is shown in the 6th month.
In the current study, almost all the domains of SF-36 improved from pre-post intervention with time within the group. The results were not significant between the groups as they might be because of no significant difference was found in DASS scores between the groups. The most likely reason for this is the too short duration of the training period. As interaction with time is seen in all the variables of DASS and SF-36, if the same protocol could be followed for a longer period, the improvement in depression and QoL (compared to the exercise-only group) is likely to become significant. While physical functioning was the only domain in SF-36 which revealed a significant difference between groups, it was not significantly similar at the baseline in both the groups. We can see that the WBV group improved with time as compared to the exercise training group. Hence, time could also be a reason for the significant difference.
One of the limitations of the study was the short duration of intervention (eight sessions over four weeks) and the absence of follow-up after the study. Secondly, comparison was not made between the male and female students on the effects of WBV. As per literature, there are gender differences in the proneness and levels of depression and anxiety. Our sample size was small and baseline characteristics differences are other limitations which may not allow generalization of our results to the Indian college student population. Future studies need to recruit larger numbers of participants and study variables such as gender differences.
Conclusion
Based on our results, the addition of WBV training is suggested for college students to help them manage depression, anxiety, and stress to facilitate overall improvement in their QoL. The WBV therapeutic model is inexpensive, simple to use, safe, each session takes only a few minutes, and the results are achieved fairly quickly, rendering it potentially attractive to the student population. We recommend that WBV units are made available in higher education institutions.
Disclosure
The study was approved by the Institutional Ethical Committee, Jamia Millia Islamia, New Delhi, India with Ref. 26/11/263/JMI/IEC/2019. Informed written consent was obtained from each participant included in the study and the study protocol conforms to the ethical guidelines. The authors declared no conflicts of interest. The study was supported by the Jamia Millia Islamia, New Delhi. No funding was received for this study.
Acknowledgments
The authors express their gratitude to the participants of the study.
references
- 1. Mikolajczyk RT, Brzoska P, Maier C, Ottova V, Meier S, Dudziak U, et al. Factors associated with self-rated health status in university students: a cross-sectional study in three European countries. BMC Public Health 2008 Jun;8:215.
- 2. Day TA. Defining stress as a prelude to mapping its neurocircuitry: no help from allostasis. Prog Neuropsychopharmacol Biol Psychiatry 2005 Dec;29(8):1195-1200.
- 3. Beiter R, Nash R, McCrady M, Rhoades D, Linscomb M, Clarahan M, et al. The prevalence and correlates of depression, anxiety, and stress in a sample of college students. J Affect Disord 2015 Mar;173:90-96.
- 4. WHO. int. Depression. 2022 [cited 2022 May 31]. Available from: https://www.who.int/news-room/fact-sheets/detail/depression.
- 5. Sarkar S, Gupta R, Menon V. A systematic review of depression, anxiety, and stress among medical students in India. Journal of Mental Health and Human Behaviour 2017 Jul;22(2):88.
- 6. Andrews B, Wilding JM. The relation of depression and anxiety to life-stress and achievement in students. Br J Psychol 2004 Nov;95(Pt 4):509-521.
- 7. Hidaka BH. Depression as a disease of modernity: explanations for increasing prevalence. J Affect Disord 2012 Nov;140(3):205-214.
- 8. Davoudi-Kiakalayeh A, Mohammadi R, Pourfathollah AA, Siery Z, Davoudi-Kiakalayeh S. Alloimmunization in thalassemia patients: new insight for healthcare. Int J Prev Med 2017 Dec;8(1):101.
- 9. Naveen GH, Thirthalli J, Rao MG, Varambally S, Christopher R, Gangadhar BN. Positive therapeutic and neurotropic effects of yoga in depression: a comparative study. Indian J Psychiatry 2013 Jul;55(7)(Suppl 3):S400-S404.
- 10. Cooney GM, Dwan K, Greig CA, Lawlor DA, Rimer J, Waugh FR, et al. Exercise for depression. Cochrane Libr 2013;9(9):1-123.
- 11. Martinsen EW. Physical activity in the prevention and treatment of anxiety and depression. Nord J Psychiatry 2008;62(Suppl 47):25-29.
- 12. Phillips WT, Kiernan M, King AC. Physical activity as a non-pharmacological treatment for depression: a review. Complement Health Pract Rev 2003;8(2):139-152 .
- 13. Aksoy D. Effect of whole body vibration training on depression level. J Educ Train Stud 2019;7(3):65 .
- 14. Wunram HL, Hamacher S, Hellmich M, Volk M, Jänicke F, Reinhard F, et al. Whole body vibration added to treatment as usual is effective in adolescents with depression: a partly randomized, three-armed clinical trial in inpatients. Eur Child Adolesc Psychiatry 2018 May;27(5):645-662.
- 15. Oberste M, Großheinrich N, Wunram HL, Graf JL, Ziemendorff A, Meinhardt A, et al. Effects of a 6-week, whole-body vibration strength-training on depression symptoms, endocrinological and neurobiological parameters in adolescent inpatients experiencing a major depressive episode (the “Balancing Vibrations Study”): study protocol for a randomized placebo-controlled trial. Trials 2018 Jul;19(1):347.
- 16. Wipfli B, Landers D, Nagoshi C, Ringenbach S. An examination of serotonin and psychological variables in the relationship between exercise and mental health. Scand J Med Sci Sports 2011 Jun;21(3):474-481.
- 17. Hasler G. Pathophysiology of depression: do we have any solid evidence of interest to clinicians? World Psychiatry 2010 Oct;9(3):155-161.
- 18. Bosco C, Iacovelli M, Tsarpela O, Cardinale M, Bonifazi M, Tihanyi J, et al. Hormonal responses to whole-body vibration in men. Eur J Appl Physiol 2000 Apr;81(6):449-454.
- 19. Alentorn-Geli E, Padilla J, Moras G, Lázaro Haro C, Fernández-Solà J. Six weeks of whole-body vibration exercise improves pain and fatigue in women with fibromyalgia. J Altern Complement Med 2008 Oct;14(8):975-981.
- 20. Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther 1995 Mar;33(3):335-343.
- 21. Crawford JR, Henry JD. The Depression anxiety stress scales (DASS): normative data and latent structure in a large non-clinical sample. Br J Clin Psychol 2003 Jun;42(Pt 2):111-131.
- 22. White CA, Pilkey RM, Lam M, Holland DC. Pre-dialysis clinic attendance improves quality of life among hemodialysis patients. BMC Nephrol 2002 Apr;3(1):3.
- 23. McHorney CA, Ware JE Jr, Lu JF, Sherbourne CD. The MOS 36-item Short-Form Health Survey (SF-36): III. Tests of data quality, scaling assumptions, and reliability across diverse patient groups. Med Care 1994 Jan;32(1):40-66.
- 24. Atlantis E, Chow CM, Kirby A, Singh MF. An effective exercise-based intervention for improving mental health and quality of life measures: a randomized controlled trial. Prev Med 2004 Aug;39(2):424-434.
- 25. Carter T, Morres I, Repper J, Callaghan P. Exercise for adolescents with depression: valued aspects and perceived change. J Psychiatr Ment Health Nurs 2016 Feb;23(1):37-44.
- 26. Smits JA, Zvolensky MJ. Emotional vulnerability as a function of physical activity among individuals with panic disorder. Depress Anxiety 2006;23(2):102-106.
- 27. Jayakody K, Gunadasa S, Hosker C. Exercise for anxiety disorders: systematic review. Br J Sports Med 2014 Feb;48(3):187-196.
- 28. Rebar AL, Stanton R, Geard D, Short C, Duncan MJ, Vandelanotte C. A meta-meta-analysis of the effect of physical activity on depression and anxiety in non-clinical adult populations. Health Psychol Rev 2015;9(3):366-378.
- 29. Jackson EM. Stress relief: The role of exercise in stress management. ACSM’s Health Fit J 2013 May;17(3):14-19 .
- 30. Greenwood BN, Fleshner M. Exercise, stress resistance, and central serotonergic systems. Exerc Sport Sci Rev 2011 Jul;39(3):140-149.
- 31. Arslan G, Ayranci U, Unsal A, Arslantas D. Prevalence of depression, its correlates among students, and its effect on health-related quality of life in a Turkish university. Ups J Med Sci 2009;114(3):170-177.
- 32. Niemeier V, Kupfer J, Gieler U. Acne vulgaris - Psychosomatische aspekte. JDDG - J Ger Soc Dermatology. 2006 Dec;4(12):1027–36.
- 33. Olivares PR, Gusi N, Parraca JA, Adsuar JC, Del Pozo-Cruz B. Tilting Whole Body Vibration improves quality of life in women with fibromyalgia: a randomized controlled trial. J Altern Complement Med 2011 Aug;17(8):723-728.
- 34. Bruyere O, Wuidart MA, Di Palma E, Gourlay M, Ethgen O, Richy F, et al. Controlled whole body vibration to decrease fall risk and improve health-related quality of life of nursing home residents. Arch Phys Med Rehabil 2005 Feb;86(2):303-307.
- 35. Álvarez-Barbosa F, del Pozo-Cruz J, del Pozo-Cruz B, Alfonso-Rosa RM, Rogers ME, Zhang Y. Effects of supervised whole body vibration exercise on fall risk factors, functional dependence and health-related quality of life in nursing home residents aged 80+. Maturitas 2014 Dec;79(4):456-463.
- 36. Alev A, Mihriban A, Bilge E, Ayça E, Merve K, Şeyma C, et al. Effects of whole body vibration therapy in pain, function and depression of the patients with fibromyalgia. Complement Ther Clin Pract 2017 Aug;28(28):200-203.