|
Abstract
Objective: The present study aims to determine the diagnostic significance of signs and symptoms of Small Bowel Obstruction (SBO) and to ascertain if there was any delay in presentation of the patients to the hospital.
Methods: This retrospective case study spanning 3 years was conducted at Riyadh Medical Complex, Saudi Arabia. All adult patients admitted from the ER with a diagnosis of SBO were included in the study. The medical records of the patients with International Classification of Diseases (ICD) 9 codes 552.8, 560, 560.8, 560.81 and 560.9 were searched and retrieved.
Results: A total of 195 patients were included in the study out of which 174 patients had a definitive diagnosis of SBO. The study group was composed of 76.4% males and 71.8% were aged between 20 years to 60 years. The mean duration of symptoms was 4.8 days, ranging from 6 hours to 17 days. The cardinal signs and symptoms of obstruction had low sensitivity (Range: 56-75), and specificity (Range: 28-61), but relatively high positive predictive value (PPV) (Range: 86-93). The morbidity was 13.8% while mortality was 3.4%.
Conclusion: The cardinal features of SBO are neither specific nor sensitive, and though they may have an acceptable PPV, the predicted rate of false positive diagnosis is unacceptable. Therefore, the clinician may not rely on the clinical picture alone for the diagnosis of SBO. The presentation of the studied patients was delayed compared to the literature and it may be an important factor in increasing morbidity and mortality, but this aspect needs to be studied further.
Keywords: Small Bowel Obstruction; Clinical Diagnosis; Signs and Symptoms.
Introduction
Small Bowel Obstruction (SBO) is characterized by complete or partial cessation of intestinal transit.1 It is the most common surgical disorder of the small intestine,2 so much so that 60-80% of all intestinal obstruction is in the small bowel.3 Twenty percent of all surgical admissions for acute abdominal pain are due to adhesive obstruction of the small bowel.4 Its timely diagnosis and appropriate management is critical to preventing complications; particularly perforation and ischemia. The traditional basis of diagnosis has been the presenting signs and symptoms. This has been complemented with a vast array of investigations ranging from plain radiography to video capsule endoscopy.5 However, many clinicians still largely depend on the clinical picture when they diagnose SBO.
The aim of the present study is to determine the relevance of presenting signs and symptoms of the small bowel obstruction to the final diagnosis and to determine the time period between onset of symptoms and presentation to the hospital to see if there was any delay in seeking treatment.
Methods
This retrospective case study was undertaken at the Department of General Surgery, Riyadh Medical Complex, Riyadh, Saudi Arabia, spanning a period of three years from January 2000 to December 2003. All patients admitted from the ER with an initial working diagnosis of SBO were included in the study. Pediatric age group was excluded as were all those patients who had peritonitis or other evidence of abdominal sepsis. In the presence of suggestive clinical picture, significant dilatation and air fluid levels on plain radiographs complemented with contrast enhanced CT scan in ambiguous cases were used to diagnose SBO. The clinical findings were elicited by the general surgical specialist on call as per the hospital policy for such cases. However, patients with a non organic cause or with a final diagnosis of paralytic ileus were excluded.
Initially, the patients were managed conservatively. Deep venous thrombosis (DVT) prophylaxis was initiated in all cases, while antibiotics were initiated in selected cases where there was clinical or hematological evidence of infection or the patient underwent surgery. Intravenous fluid requirement was assessed by clinical and biochemical parameters of dehydration. After initial bolus of 1-1.5 lit of Ringer’s Lactate, further resuscitation was carried out according to urine output. Non operative therapy included classical drip & suck or undiluted Gastrografin follow though. If a patient failed to respond to conservative treatment for ≥24 to 36 hours, surgery was then considered. A patient was considered to have failed conservative treatment if he/she did not pass flatus or faeces along with cessation of vomiting/significant decrease of NGT aspiration and/or did not have decreased abdominal distention.
ICD 9 codes (International Classification of Diseases Version 9) 552.8, 560, 560.8, 560.81 and 560.9 were used to search for and retrieve the medical records. Demographic information, clinical presentation, laboratory and imaging studies were recorded. Treatment offered, final diagnosis and outcome were also reviewed. The data was tabulated and processed using MS Excel 2002. Appropriate statistical tests were applied where applicable.
Results
A total of 195 patients were admitted with an initial diagnosis of SBO, during the study period. Twenty one were diagnosed to have extraintestinal causes for their abdominal symptoms and were used as controls, leaving 174 patients with a definitive diagnosis of SBO. Among them, 133 (76.4%) patients were males and 41 (23.6%) females. One hundred and twenty five (71.8%) were aged between 20 years to 60 years. Although elderly patients (³60 years) were one fifth of the total 33 (18.9%), there were no cases of malignant obstruction.
The mean duration of symptoms was 4.8 days, ranging from 6 hours to 17 days. But more than half 97 (55.8%) patients presented within 3 days of the onset of symptoms, while 22 (12.6%) patients delayed seeking medical help for more than a week. Abdominal pain was the commonest symptom reported by 143 (82.2%) patients, followed by vomiting 117 (67.2%) and constipation 111 (63.8%). However, only 69 (39%) patients had obstipation. For these four cardinal features of SBO, sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated. (Table 1)
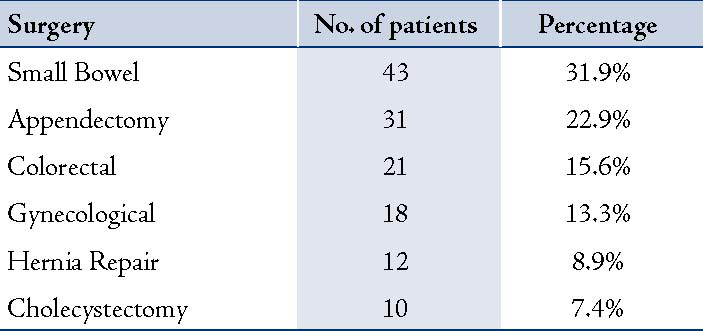
Bowel sounds were exaggerated in 88 (45.4%) patients and appeared sluggish in 11 (6.4%) patients, but unexpectedly 75 (42.9%) patients had normal sounds. Patients reporting previous episodes of vague abdominal pain ± constipation were not considered to have had an obstructive event. Fifty nine (33.9%) patients had documented previous admissions for SBO, and for the rest 115 (66.1%) this was the first episode. One hundred and thirty five (77.6%) patients had previous abdominal surgery.
Table 1: Sensitivity, Specificity, PPV and NPV of Signs and Symptoms of Small Bowel Obstruction.
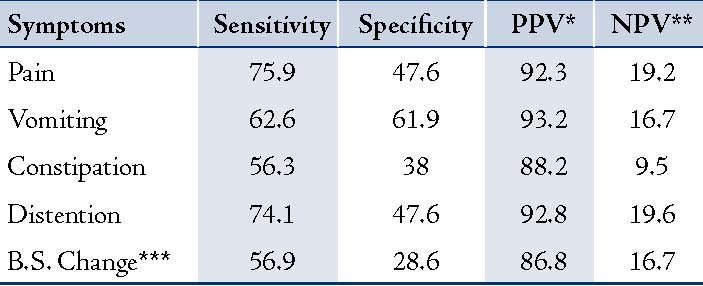
Table 2: Nature of Preceding Abdominal Surgery. (n=135)
One hundred and seventeen patients (67.2%) had a normal leucocyte count (4-11000 /ml), while 57 (32.8%) had an elevated count. Plain radiology was the primary imaging modality used. Significant air fluid levels were seen in 168 (96.6%) patients. One hundred and forty nine (88.7%) of these 168 patients had dilated loops of small intestine only. While 16 patients had colonic dilatation as well as small bowel dilatation. These patients underwent full colonoscopy and were found to have a normal colon. In the remaining 19 patients, it was difficult to determine unequivocally the level of intestine dilated but demonstrated significant air fluid levels. Contrast enhanced CT was ordered in 7 patients in whom no previous surgery or external hernias were found. Two were diagnosed with caecal volvulus and 5 had ileocaecal tuberculosis as diagnosed by CT findings.
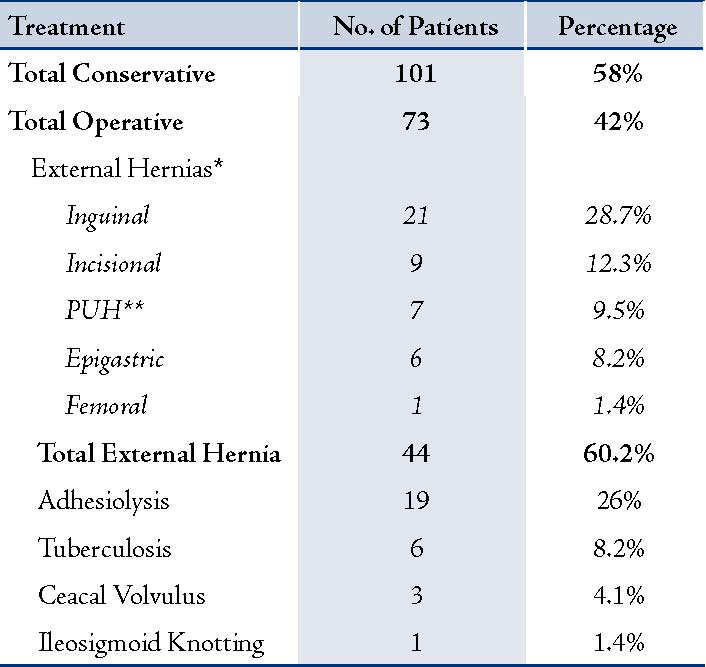
One hundred and one (58%) of the patients resolved with non-operative therapy. Following the failure of conservative therapy 73 (42%) patients required surgery, (Table 3). Among them, 23 patients had previous abdominal surgery. Four of these patients had iatrogenic bowel injuries which were repaired per-operatively, but only one went on to develop enterocutaneous fistulas.
Significant morbidity was seen in 24 (13.8%) patients. Seven patients developed wound infection requiring drainage of pus and antibiotics. Atelectasis and/or pneumonia were seen in 6 patients. Two patients developed symptomatic intraabdominal collection, 5 patients had enterocutaneous fistulae while 4 patients had symptomatic deep venous thrombosis (DVT). Six patients expired due to various causes which included DVT and pulmonary embolism (PE),1 Gastrointestinal (GI) fistulas/sepsis,3 and hospital acquired pneumonia.2
Table 3: Treatment Offered to the Patients. (n=174)
Discussion
Intestinal obstruction is a very common presentation in the ER, accounting for a large proportion of emergency surgical admissions.6 The complication of perforation and vascular compromise are potentially fatal if not diagnosed and treated early.7 By and large SBO presents with a well-recognized clinical picture comprising characteristic signs and symptoms, even though sometimes, the clinical examination may be rendered difficult under certain conditions like obesity or pregnancy.7 But are they really as helpful as they have been considered to be in reaching a diagnosis? This is the question that needs to be examined.
Traditionally, SBO is said to present with four cardinal features: abdominal pain, vomiting, abdominal distention and absolute constipation.8,9 However, it has been noted that patients may have any or all of these symptoms from extra intestinal causes or conversely, those with small bowel obstruction may be relatively symptomless. Absolute constipation is unusual with patients who may continue to pass small amounts of flatus and stool, and this does not exclude SBO.10,11 Some authors find the symptoms and signs so unreliable that they deem it difficult to diagnose intestinal obstruction on the basis of history and physical alone.12,13 Overall, we found a sensitivity ranging from 56-76% and an even lower specificity. The PPV however was clustered around 90%, while the NPV was dismally low. Other studies have found similar results. Jang et al.14 have also reported sensitivity of these symptoms ranging from 36 to 88 while specificity being much lower ranging from 16 to 74. All this indicates that a diagnosis of SBO based on symptomatology alone will have a high false positive rate. Hence it is imperative that adjuncts like contrast radiography and even CT scan may be used to enhance the diagnostic yield.
The common causes of SBO are adhesions, obstructed hernias, volvulus not due to adhesions, intussusseption, carcinoma and others.7 Some rare causes have also been reported which include Schistosomiasis,15 torsion of appendix epiploicae,16 pregnancy,17 ileosigmoid knotting,18 Meckel’s diverticulum enterolith,19 or even an intramural hematoma due to anticoagulant therapy.20 In the current series, we also found adhesions and hernias to be the most common causes of SBO. However, no cases of malignant obstruction were encountered. This may be due to the fact that in our area, patients with malignancy are treated in specialized oncology centers. This is considered a limitation of the current study that a significant subset of patients is not included. Another limitation may be that it is a retrospective study. Additionally, a longer study period would have given more robust results.
The morbidity rate of 13.8% in the current series was a bit on the higher side. The time from onset of symptoms and admission to the hospital has been found to vary from 3 hours to 3 days in one study.17 A treatment delay of more than 24 hours is a reported risk factor for increasing mortality and complication rate.21 In this series, the patients seem to have delayed seeking medical help with a mean interval of 4.8 days; the maximum being 17 days. One fifth of the patients delayed seeking help for more than a week. We believe that the most common reasons for the delay may be logistic and eligibility problems, followed by misdiagnosis by primary physicians. This delay between the first complaints of the patient and the final treatment may be an important cause of morbidity and mortality.2 However, there is need for further studies conducted in our local setting dealing with the effect of delay in presentation on the outcome of SBO.
Conclusion
The cardinal features of SBO are neither very specific, nor sensitive for the diagnosis, though they may have an acceptable PPV, the predicted rate false positive diagnoses is unacceptable. Hence generally, the clinician may not rely on the clinical picture alone for the diagnosis of SBO. We found our patients presenting after a long delay, which has been postulated by some authors to be a factor in increasing morbidity and mortality. Further studies, however are required to determine the effect of delay on the outcome of SBO.
Acknowledgements
The authors reported no conflict of interest and no funding was received in this work.
References
1. Miller G, Boman J, Shrier I, Gordon PH. Etiology of small bowel obstruction. Am J Surg 2000 Jul;180(1):33-36.
2. Hauspy J, Roofthooft N, Meulyzer P, Leyman P. Small bowel obstruction during pregnancy. Acta Chir Belg 2004 Oct;104(5):588-590.
3. Maglinte DD, Balthazar EJ, Kelvin FM, Megibow AJ. The role of radiology in the diagnosis of small-bowel obstruction. AJR Am J Roentgenol 1997 May;168(5):1171-1180.
4. Welch JP. General Considerations and mortality in bowel obstruction. In: Welch JP, ed. Bowel Obstruction: Differential diagnosis and clinical management. Philadelphia: Saunders 1990: p. 59-95.
5. Stock TR. Small Intestine. In: Way LW, Current Surgical Diagnosis and Treatment, eds. Appleton and Lange, 1994: p. 623.
6. Delabrousse E, Destrumelle N, Brunelle S, Clair C, Mantion G, Kastler B. CT of small bowel obstruction in adults. Abdom Imaging 2003 Mar-Apr;28(2):257-266.
7. Chang YT, Huang YS, Chan HM, Huang CJ, Hsieh JS, Huang TJ. Intestinal obstruction during pregnancy. Kaohsiung J Med Sci 2006 Jan;22(1):20-23.
8. Rains AJ, Capper WM, Charnley J, Cleland WP, Knight G. Bailey and Love’s Short Practisce of Surgery. Lippincott Company, Philadelphia. 13th Edition, 1965.Chapter 42, p. 963-964
9. Chapple KS, Hartley JE. Intestinal Obstruction. Br J Hosp Med 2006;67:5-6.
10. Sykes PA, Schofield PF. Early postoperative small bowel obstruction. Br J Surg 1974 Aug;61(8):594-600.
11. Frykberg ER, Phillips JW. Obstruction of the small bowel in the early postoperative period. South Med J 1989 Feb;82(2):169-173.
12. Herlinger H, Maglinte D, Birnbaum BA. Clinical imaging of the small intestine. 2nd ed. New York: Springer 1999: p. 94-95.
13. Ha HK, Rha SE, Kim AY, Auh YH. CT and MR diagnoses of intestinal ischemia. Semin Ultrasound CT MR 2000 Feb;21(1):40-55.
14. Jang TB, Schindler D, Kaji AH. Predictive value of signs and symptoms for small bowel obstruction in patients with prior surgery. Emerg Med J. 2011 Jan 6.
15. Lamyman MJ, Noble DJ, Narang S, Dehalvi N. Small bowel obstruction secondary to intestinal schistosomiasis. Trans R Soc Trop Med Hyg 2006 Sep;100(9):885-887.
16. Osadchy A, Shapiro-Feinberg M, Zissin R. Strangulated small bowel obstruction related to chronic torsion of an epiploic appendix: CT findings. Br J Radiol 2001 Nov;74(887):1062-1064.
17. Meyerson S, Holtz T, Ehrinpreis M, Dhar R. Small bowel obstruction in pregnancy. Am J Gastroenterol 1995 Feb;90(2):299-302.
18. Hashimoto T, Yamaguchi J, Fujioka H, Okada H, Izawa K, Kanematsu T. Two cases of ileosigmoid knot: the youngest reported patient and CT findings. Hepatogastroenterology 2004 May-Jun;51(57):771-773.
19. Gamblin TC, Glenn J, Herring D, McKinney WB. Bowel obstruction caused by a Meckel’s diverticulum enterolith: a case report and review of the literature. Curr Surg 2003 Jan-Feb;60(1):63-64.
20. D’Abbicco D, Margari A, Amoruso M, Notarnicola A, Casagranda B, Basile R, et al. Small bowel obstruction due to intramural hematoma during anticoagulant therapy. With regard to two cases treated conservatively. Chir Ital 2003 Jul-Aug;55(4):565-569.
21. Fevang BT, Fevang J, Stangeland L, Soreide O, Svanes K, Viste A. Complications and death after surgical treatment of small bowel obstruction: A 35-year institutional experience. Ann Surg 2000 Apr;231(4):529-537.
|