Lung cancer is the most common malignancy affecting humanity today. In 2018, the International Agency for Research on Cancer (IARC) estimated that over two million new cases of lung cancer (11.6% of all cancers) were diagnosed worldwide.1 Lung cancer is also one of the deadliest among cancers, responsible for nearly 1.8 million deaths (18.4% of total global cancers).1
Lung cancer was ranked the seventh most common cancer among both genders of the Arab Gulf Cooperation Council (GCC) states (Bahrain, Kuwait, Qatar, Saudi Arabia, Oman, and the UAE) between 1998–2012, with an average of 505 new cases (4.6% of total cancers) per year.2 In Oman, although incidence data on lung cancer are published annually by the National Health Authorities, its epidemiology, associated risk factors, and trends over the past two decades have not been examined closely. In this analysis, we present an outline of various patterns of lung cancer observed among Omani nationals from 1996 to 2015.
Methods
We extracted data of subjects diagnosed with lung cancer from the Oman National Cancer Registry (ONCR). Details of registry methods and data collection processes are published elsewhere.3 In brief, the registry collects its data by active (registry personnel visiting potential sources of case reporting and abstracting data on cancer registry forms) and passive data collection methods (case notification forms sent to the registry by the attending physician or medical record personnel). The variables collected include age, gender, date of diagnosis, morphology, topography and tumor behavior with codes based on the third edition of the International Classification of Disease for Oncology (ICD-O3).4 Cases included in this analysis were subjects registered as having primary lung carcinomas of trachea, bronchi, and lung (ICD-O3 codes C33 and C34, collectively referred to as lung cancer) in the period from 1 January 1996 to 31 December 2015. Cases were grouped according to histological codes as defined in volume IX of Cancer Incidence in Five Continents.5
Our analysis is limited to Omani nationals in the ONCR database. Non-Omanis, mainly young male workers in Oman, represent a skewed population from a wide range of countries worldwide, making determining a denominator for the calculation of incidence rates among them a complex exercise.
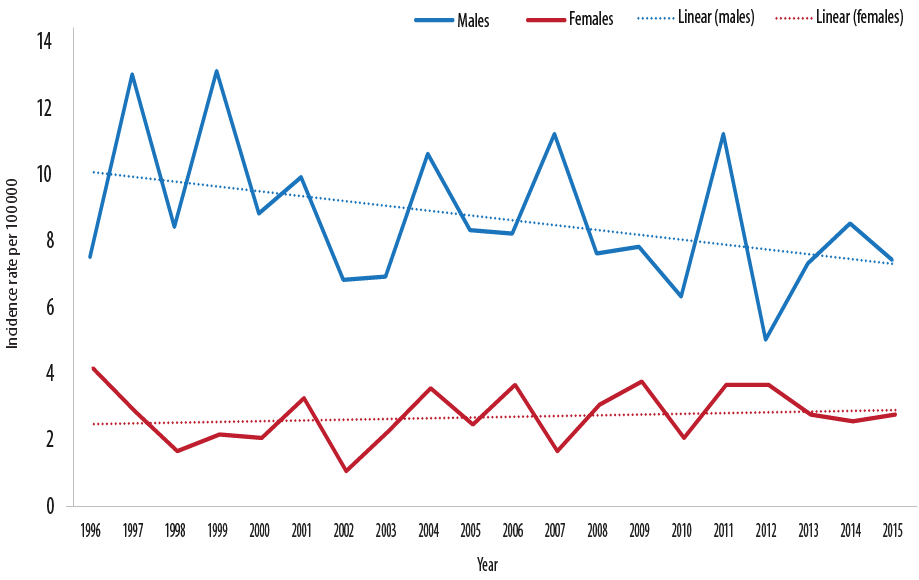
Figure 1: Trends of lung cancer incidence by gender in Oman between 1996 and 2015.
Frequency tables, crude incidence rates (CR), and age-standardized incidence rates (ASR) of lung cancer, for all ages in each year, were calculated using the CanReg5 software.6 ASR was calculated using the World Standard Population first proposed by Segi and later modified by Doll and colleagues.7,8 The average CR and ASR over each of the three calendar periods (1996–2005, 2006–2015, and 1996–2015) were calculated. The average population between 2000 and 2001, 2010 and 2011, and 2005 and 2006 was used to obtain the mid-period population and calculate the incidence rates over these three periods. Validity checks were performed for consistency between site/histology, gender/site, and age/site/histology combinations using inbuilt properties of CanReg5. Population data, used for the calculations of incidence rates by five-year age group and gender, were obtained from the Ministry of Health’s Annual Health Reports.9 Data was exported to Stata software (version 14.2, Stata Corporation, TX, USA) to obtain means and medians by gender and tumor morphology. Bar diagrams and graphs, including regression trends, were generated using Excel. The p-values for the differences in ASR between males and females as well as between 1996–2005 and 2006–2015 in males and females were generated using Poisson regression. Mortality data was obtained from the Global Cancer Observatory.10
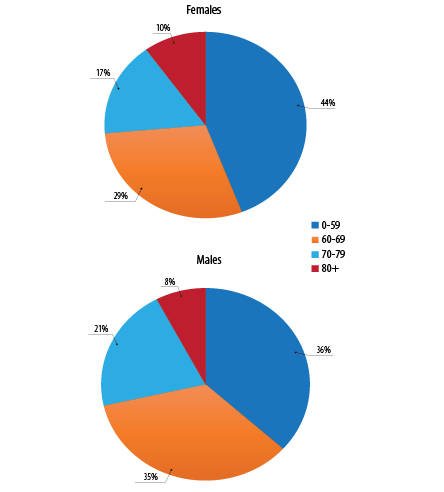
Figure 2: Age distribution of lung cancer by gender in Oman between 1996-2015 .
Results
Between 1996 and 2015, a total of 956 cases of primary lung cancer were registered in the ONCR accounting for 4.5% of all invasive cancers (including non-melanoma skin cancer), ranking it as the eighth most common cancer in Oman [Table 1]. On average, 48 cases were diagnosed per annum; 36 in males and 12 in females. The overall male to female ratio was 3:1, ranking lung cancer as the sixth most common cancer among Omani men preceded by prostate, stomach, non-Hodgkin lymphoma, leukemia, and colorectal cancers. In females, it did not reach the 10 most frequent tumors.
The ASR during 1996–2015 ranged from 5.0 to 13.0 cases per 100 000 men and 1.0 to 4.0 per 100 000 women [Figure 1]. When cases were subdivided into two calendar periods (1996–2005 and 2006–2015), men tended to have slightly higher ASR in the earlier period compared to the late period (9.1 per 100 000 vs. 7.7 per 100 000; p = 0.332), while women, on the other hand, had slightly higher rates in the late period compared to the earlier period (2.8 per 100 000 vs. 2.4 per 100 000; p = 0.577), respectively. However, the differences were not statistically significant [Table 1]. Figure 1 shows regression lines of lung cancer over the 20-years studied for males and females.
Table 1: Distribution of lung cancer by gender between 1996 and 2015, Oman.
|
1996–2005 |
|
|
|
|
|
Male |
360 |
79.5 |
4.0 |
9.1 |
|
Female |
93 |
20.5 |
1.1 |
2.4 |
|
Total |
453 |
100 |
2.4 |
5.4 |
|
2006–2015 |
|
|
|
|
|
Male |
365 |
72.6 |
3.5 |
7.7 |
|
Female |
138 |
27.4 |
1.3 |
2.8 |
|
Total |
503 |
100 |
2.5 |
4.8 |
|
1996–2015 |
|
|
|
|
|
Male |
725 |
75.8 |
3.7 |
8.2 |
|
Female |
231 |
24.2 |
1.2 |
2.6 |
CR: crude incidence rate (per 100 000 population); ASR: age-standardized incidence rate (per 100 000 population).
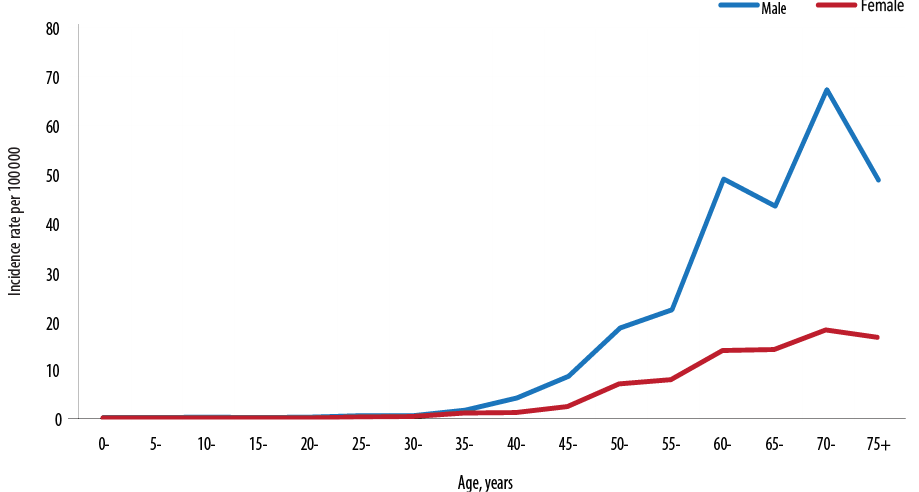
Figure 3: Age-specific incidence rates of lung cancer by gender in Oman between 1996 and 2015.
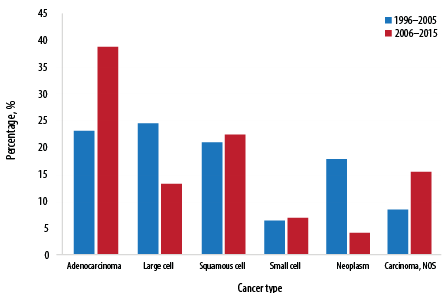
Figure 4: Comparison of lung cancer morphology recorded between 1996–2005 and 2006–2015 in Oman.
The overall age profile for men and women was similar, with the majority of men (36.0%) and women (44.0%) diagnosed under the age of 60 years [Figure 2]. A further 29.0–34.0% were diagnosed in their sixth decade while 27.0 to 29.0% were diagnosed in the seventh decades. The mean age at diagnosis for men and women was 60.0 and 61.0 years, respectively, over both time periods and the median was 61 and 59 years, respectively. In both sexes, the ASR per 100 000 increased with increasing age, peaked at 70–74 years and declined for ages 75 years and above [Figure 3].
In the earlier period (1996–2005), large cell carcinoma formed 24.0% of all primary malignant lung tumors in Oman followed by adenocarcinoma (23.0%), squamous cell carcinoma (21.0%), and small cell carcinomas (6.0%) [Figure 4]. In the latter period (2006–2015), adenocarcinoma increased by 67.0%, and squamous cell tumors increased slightly while large cell tumors decreased by 46.0% compared to the earlier period. The proportion of small cell carcinomas remained similar in both periods between (6.0–7.0%).
For both genders, the proportion of cases diagnosed from death certificates and non-microscopic means decreased dramatically from 2.4% and 13.2% between 1996 and 2005 to 0% and 1.0% between 2006 and 2015. On the other hand, cases diagnosed through microscopic means increased from 83.0% to 99.0% in the two periods, respectively. Cases identified by ‘unknown’ methods remained less than 1.0% throughout the two periods.
Of the 1681 cancer deaths that occurred in 2018 in Oman, 108 (6.4%) were attributed to lung cancer.10 Nearly 86.0% of lung cancer deaths in 2018 occurred in men making it the third leading cause of death due to cancer in men after stomach and colorectal cancers. The ASR of lung cancer mortality was estimated to be 6.7 per 100 000 in men and 1.5 per 100 000 in women in 2018 in Oman.10
Discussion
Our analysis shows that Oman had one of the lowest age-standardized lung cancer incidence rates in the world (8.2 per 100 000 for men and 2.6 per 100 000 for women) over the 20 years studied (1996–2015), and there was no evidence of changes in trend throughout this period. In an analysis by the IARC in 2018, Oman had the fourth lowest ASR of lung cancer among men (7.1 cases per 100 000) in all 48 countries of Asia studied, preceded only by Yemen (3.9), Saudi Arabia (5.8) and the UAE (7.0).1 In the same study, Omani women ranked first, with the lowest ASR rate (1.5 per 100 000) of lung cancer among Asian female populations.1
Another study of 32 291 cancer cases from six population-based registries of the GCC between 1998 and 2001, also confirmed a low ASR of lung cancer in Oman (9.2 per 100 000 in males and 2.2 per 100 000 in females).11 In contrast to the very low ASR of lung cancer in Oman, Saudi Arabia, and the UAE, higher rates were reported among men and women from Bahrain (34.3 and 12.1), Qatar (18.5 and 5.5), and Kuwait (13.8 and 4.0).11 The highest ASR of lung cancer were reported from the European region with Hungarian men and women topping the world list (77.4 per 100 000 and 41.4 per 100 000, respectively), followed by men in Serbia (71.6), Turkey (70.6), Greece (67.8), Montenegro (62.9), Bosnia and Herzegovina (62.4), French New Caledonia (59.9), and Armenia (58.5).1,10 High incidence rates of lung cancer were also reported in men from several Arab populations including Jordan (32.0), Lebanon (31.3), Gaza Strip and West Bank (26.7), and Syria (26.6) (all per 100 000 population).10 On the other hand, the lowest ASR of lung cancer in men were reported from African nations including Comoros, Tanzania, Niger, and Benin (all < 1 per 100 000 population).1,10
In a second analysis of nearly 165 000 incidence cases of cancer in six GCC countries between 1998 and 2012, statistically significant increasing trends of lung cancer were seen in men from Saudi Arabia, while statistically significant decreasing trends were reported for men in Kuwait and both sexes in Bahrain.2 No significant trends of lung cancer were reported in populations from Oman, Qatar, and the UAE.2 Wong and colleagues studied lung cancer trends in 38 countries and found a declining incidence in men in 22 countries and an increasing incidence in 19 countries in women.12 A high proportion of these countries reported a decreasing mortality trend in men (30 out of 36) and increasing trend in women (16 out of 36).12 These disparities of lung cancer incidence and mortality rates have been attributed to higher human development index, greater westernization effect, where tobacco use and air pollution due to industrialization were more common in more developed nations.12
The exceptionally low ASR of lung cancer and its mortality in Oman could be explained by Oman being one of the lowest prevalence countries for tobacco use in the world, ranked as 11th lowest among 149 countries for current age-standardized smoking rates in the world (15.6% in men, 0.5% in women, 8.1% for both genders).13 Before 1970, smoking in public places in Oman was a crime punishable by imprisonment.14 This may have led to the formation of a non-smoker-cohort with the effect of low incidence of lung cancer shown in this analysis. Additionally, the government imposes custom tariffs (at the rate of 100% valorem tax) on all tobacco products and from June 2019 an additional selective taxes, at the rate of 100% of retail prices, was imposed on all tobacco products, and energy drinks, and at a rate of 50% on most sugary drinks and alcoholic beverages in an effort to curb the burden of non-communicable diseases risk factors including cancer.15 Such fiscal policy when coupled with other tobacco control strategies (e.g., comprehensive bans on indoor smoking in public places, bans on tobacco advertisement, promotion and sponsorship, and public education on the dangers of tobacco use) are likely to reduce the likelihood of any lung cancer epidemic in Oman in the future.14
In this analysis, the risk of lung cancer began to increase, in both sexes, as early as the third decade of life (30–34 years), and most cases were diagnosed below the age of 60 years. This age was reported to commence a decade earlier (20–24 years) in Saudi Arabia, in the 25–29 year age group in Oman and the UAE, in the 30–34 year age group in Qatar, and 45–49 year age group in Bahrain and Kuwait.2 In the UK and China, the risk of lung cancer is reported to increase around the age of 45 years and above.16,17 It is not clear as to why the risk of lung cancer starts to rise in Oman, UAE, Saudi Arabia, and Qatar in or around the third decade of life while in the UK and China, for example, the risk starts to surge after the fourth decade of life (45 years and above).16,17 Whether this is due to biological variation attributed to genetic predisposition or environmental risk factor exposure remains unclear.
The peak ASR in our analysis was similar to that reported from other Gulf states and was in the 70–74 years age group,2 while the peak incidence rates in the US, UK, Australia, and China were reported to occur in the eighth decade of life (80 years and above).16–19 Furthermore, the mean age at diagnosis for lung cancer in Oman for both genders was between 59 and 61 years old. Qatar and Malaysia reported a similar mean age at diagnosis (60.8 and 61 years, respectively)11,20 while the mean age at diagnosis increased in Kuwait, Saudi Arabia, and the UAE to 63.4 years and in Bahrain it reached 68.7 years.11 In the US and Australia, the mean age at diagnosis for both sexes ranged between 70–71 years.18,19
In Kuwait and Bahrain, the age of onset of lung cancer (45–49 years) was more consistent with figures reported from other countries compared to other GCC states.16,17 This could be attributed to the fact that in these two countries, a civil registration and vital statistics system was established much earlier (Kuwait in 1952 and Bahrain in 1970)21,22 than other Gulf countries (Saudi Arabia in 1983, Qatar in 2000, and Oman in 2004).23 Consequently, this may have led to inaccuracies with underestimation of age reported by many patients, as seen by the ‘early’ age of disease onset of lung cancer by 15 years in this study compared to the age of onset reported from Bahrain and Kuwait. In Oman, we believe that significant numbers of patients, before 2004, did not report accurate age to medical records clerks at registration in health institutions mainly due to unavailability of a functioning civil registration and vital statistics system24 and reliance of the country on ‘age estimation’ methods to determine individuals age, a practice which is still ongoing, albeit on limited scale.25 From the 1980s, the Ministry of Health (at the time in-charge birth and hospital deaths registration) established several regional ‘age estimation committees’26 throughout Oman. Although the civil registration system, which includes registration of births, deaths, marriages, and divorces in Oman, began in 1999, it was not fully functional until 2004.27 Furthermore, most of the cohort currently aged 50 years and above, were born at home due to the unavailability of hospitals before 1970 (two hospitals with a total of 12 beds),28 which further compounded ‘age inaccuracies’.
The morphological patterns of lung tumors in this study are consistent with the relatively low prevalence rates of tobacco smoking in Oman, where small cell and squamous cell carcinomas’ (predominantly associated with habitual tobacco use) frequency was 6% and 19%, respectively, and similar to what was reported from other GCC states (9.4% and 18.8%, respectively).2 Internationally, higher percentages were reported for small cell (10–15%) and squamous cell tumors (25–30%).29
We observed a 67% increase in the prevalence of adenocarcinomas from 23% to 39% over two decades. This is consistent with international reports where adenocarcinomas formed up to 40% of all lung cancers.29 In the past, about 10% of all lung cancers were classified as large cell.30 However, as more exact ways of diagnosing lung cancer have come into use, many lung cancers that would have been considered large cell in the past are now being identified as adenocarcinoma or squamous cell lung cancer. This may have been the case in Oman where the increase in adenocarcinomas was coupled by a reduction of 11% in large cell carcinomas. Adenocarcinomas are also the most common of all lung cancers in both genders (but more so among females in Oman as seen from this study), in all GCC states2 and worldwide.31
The strength of this study is that it is the first report to evaluate lung cancer epidemiology in Oman and include 20-year trend data with insights about methods of diagnosis and morphology of tumors. Secondly, this study used good quality data generated by the national population-based registry covering the entire population of Oman mostly through an active data collection system. Our study has a few limitations. In addition to the wide range of data provided by the ONCR and analyzed therein, data on stages, regional distribution, survival, and modalities of treatment received by the patient were not available from the database for extraction and analysis. However, similar data were reported by a pooled analysis from all Gulf states with over 60% of lung cancer cases diagnosed in Oman and other GCC states at advanced stages (15.2% with regional and 45.5% with distant metastasis), while localized tumors were present in 9.6% of cases and in nearly one-third of cases (29.6%) the extent of disease was unknown.2
Conclusion
The incidence of lung cancer in Oman is one of the lowest rates reported worldwide with no evidence of any increasing trends. This is most likely to be due to Oman having avoided the historic tobacco epidemic, especially addiction to cigarette smoking over the past 20 years. The government and other concerned parties should capitalize on this finding and consolidate it for the years to come to avoid a Western-style lung cancer epidemic.
Disclosure
The authors declared no conflicts of interest. No funding was received for this study.