Injuries from the spines of sea urchin may cause important morbidity in humans ranging from immediate and transient episodes of local pain, bleeding, edema, and erythema1,2 (which typically resolves within hours) to vomiting, respiratory distress, and even death3 (which are uncommon). Long-term granulomatous complications from the spines are unusual and rarely reported in the literature.2
Sea urchin granuloma is believed to be a delayed reaction as a result of spine remnants in the wound. Clinically, it manifests as a firm, painless, nonsuppurative nodule with a central depression and hyperkeratotic surface, especially when localized to the hands.1,2 Histologically, the granuloma has different morphological patterns. The most frequent granulomatous type described by many pathologists is sarcoidal.4 Granulomas in soft tissues usually heal spontaneously within years without interference.5
We describe a typical case of sea urchin granuloma, the types of histological pattern found, and its therapeutic implications in a diver gathering the sea snail Haliotis mariae.
Case report
Our patient, a 45-year-old man residing in Dhofar, was a keen diver with an interest in harvesting Haliotis mariae during the traditional fishing season. Occasionally, he injured his hands with sea urchin spines with the injuries usually resolving within hours to days. He presented to the dermatology clinic two months after his last injury with multiple swellings over the dorsum of both hands. Few swellings were set over joints, but there was no joint pain or impairment of joints mobility. According to the patient, the sites of injury were initially red and painful and became infected a few days later. However, it subsided following administration of oral antibiotic prescribed by the local health center.

Figure 1: Multiple slightly hyperkeratotic nodular swellings with central hypopigmentation on the dorsum of the patient’s hands.
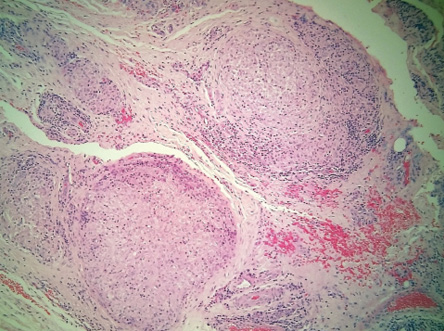
Figure 2: Epithelioid sarcoid type granuloma. Hematoxylin and eosin stain, magnification = 100 ×.
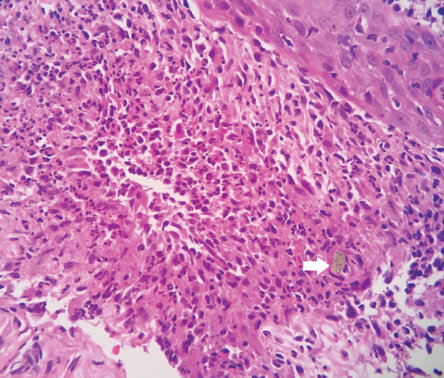
Figure 3: Non-specific chronic inflammation with focal suppuration and some foreign material
(white arrow). Hematoxylin and eosin stain, magnification = 400 ×.
His general condition was good. Dermatological examination of dorsum of hands revealed 11 nodular swellings. They were brown, 3–5 mm in diameter, non-tender, firm in consistency, and slightly hyperkeratotic with central hypopigmentation [Figure 1]. Both hand joints examination showed non-painful, normal range of active and passive motions. X-ray examination did not reveal any radiopaque spine fragments. Skin biopsies were taken from two of the granulomas. Hematoxylin and eosin stained sections of one biopsy showed non-specific chronic inflammation with focal suppuration along with foreign body material. The other specimen showed epithelioid sarcoid type granuloma [Figure 2 and 3].
The patient was managed by intralesional steroid (triamcinolone) injections every month, most of the nodules resolved after two months. However, three nodules needed an additional two months to resolve. Subsequent follow-up after five months showed complete recovery.
Discussion
Wild abalone fishing along the eastern Dhofar coast of Oman has formed part of traditional fishing culture for decades. The fishing season takes place in the winter months, usually between October and December. The preferred habitats by > 97% of Haliotis mariae include boulders and urchins as urchins are utilized as shelter, supporting the recruitment of Haliotis mariae.6
Sea urchins are one species of phylum Echinodermata, class Echinoidea.7 About 80 species are known to be toxic to humans; they are prickly rigid-shelled marine animals that live on rocky seafloor and in deep water.1,7 They have a hard outer bony structure of calcium carbonate with a thin epithelium coating on the shell and spines.8 The epithelium may contain toxic substances including serotonin, histamines, steroid, cholinergic substances, glycosides, and bradykinin-like substances.1,9
Injuries by urchin’s spines are usually seen in divers, bathers, and fishermen. Feet, ankles, and hands are the most commonly affected areas.7,8 Reactions related to sea urchin injuries can be classified into immediate and delayed.1,7
The immediate reaction is caused by sea urchin spines penetration, which causes intense local pain, erythema, edema, bleeding, and local myalgia, and resolves within a few hours to one week.1,2 Systemic manifestations are common especially if toxins injection occurs from 15 or more spines. They range from dizziness, lightheadedness, and paresthesia to aphonia, paralysis, coma, and death.3 Spine fragments embedded in soft tissues generally remain asymptomatic. However, secondary infection may occur.10
The delayed reaction may arise in the form of granulomatous nodular lesions, which slowly develop within two to 12 months.2 In our case, granulomas developed two months after penetration injury from sea urchin spines of dorsum of hands. Clinically, they are firm, flesh-colored papules and nodules that are centrally umbilicated with a hyperkeratotic surface.1,2 Histologically, sea urchin granulomas have a wide morphological spectrum. A predominant granulomatous inflammatory reaction formed of foreign body type and/or sarcoidal type are most commonly seen. Other histological patterns are suppurative, tuberculoid, necrobiotic, and non-specific inflammatory reaction.4 Most researchers suggested that granulomas are due to an immunologic response to the epithelial covering or slime of the spine, as the calcium carbonate skeleton is immunologically inert.5 Few studies described detection of Mycobacterium marinum infection in association with sea urchin granuloma.11
Tenosynovitis can occur if joints or tendon sheaths are penetrated. Impairment of joints function and occasionally severe destructive effects with functional loss may result when the inflammation takes the form of granulomatous synovitis or chronic chemical synovitis, which develops due to a reaction to either toxic substances or foreign proteins found within the spines.7,12 The spine fragments may or may not be radiopaque by X-ray. However, with a positive history of injury, presence of granulomas over joints and disability, surgical exploration under aseptic conditions is indicated. Ultrasound or magnetic resonance imaging may be helpful in doubtful cases.10,12
Neuropathy as a consequence of inflammatory reaction to sea urchin spine injuries and the dramatic restoration of normal sensation after surgical exploration and removal of sea urchin spine has also been reported.10
Treatment of sea urchin spine injuries in the vast majority of cases is conservative. Immediate immersion in hot water relieves the pain and inactivates the toxins.7,9,10,12 Observation and supportive treatment for allergic reactions, muscular paralysis, and respiratory distress, which may be associated with envenomation, are essential.10 Tetanus prophylaxis must be current.7,10 Local or systemic antibiotic administration is recommended for secondary infections.1,3,5,9 Removal of visible and/or palpable spine fragments immediately using limited elliptical incisions with magnification will cause the local reaction to subside. However, removing spines is difficult, and spines left in place will usually gradually dissolve or extruded within one or two years.5,13,14 Ablation of granulomas by erbium YAG laser has also been reported.13
Spines that have entered the joint space should be surgically removed by an experienced surgeon to avoid reactive arthritis or synovitis. If surgical exploration is indicated, it must be undertaken with all the precautions that hand surgery requires. An operating microscope may even be required.10
In general, granulomas that rest in soft tissues usually flatten without medical or surgical interventions and become replaced with scar tissue within a few years.5 However, tender granuloma can be injected with corticosteroids to help resolution, and if the lesion is small enough, excision might be preferred.1,15
Conclusion
Initial clinical manifestations of sea urchin sting are generally mild and can go unnoticed. Apart from local inflammation and pain, vomiting, respiratory distress, and even death are uncommonly occurring. Granulomas, tenosynovitis, and arthritis are chronic complications that may develop due to neglected sea urchin injuries and are rarely seen. Several histological forms of sea urchin granulomas have been described in the literature. Our case report revealed a sarcoidal pattern and a non-specific chronic inflammatory pattern with focal suppuration. These granulomas resolved after intralesional injections of steroids. Increased awareness of sea urchin granuloma when treating chronic skin nodules of unknown etiology in habitats along the coast should lead to a more rapid diagnosis.
Disclosure
The authors declared no conflicts of interest.
references
- Caputo V, Fiorella S. Sea urchin granuloma. Dermatology 2005;210(3):254-256.
- 2. Rocha G, Fraga S. Sea urchin granuloma of the skin. Arch Dermatol 1962 Mar;85:406-408.
- 3. Mebs D. A toxin from the sea urchin Tripneustes gratilla. Toxicon 1984;22(2):306-307.
- De La Torre C, Toribio J. Sea-urchin granuloma: histologic profile. A pathologic study of 50 biopsies. J Cutan Pathol 2001 May;28(5):223-228.
- 5. Surfing Medical staff. Wanna pee on my Wana? Sea urchin injuries, a literature review. Journal of the Surfers Medical Association [internet]. 2015 Aug [cited 22/12/2017]. Available from: http://journal.surfersmedicalassociation.org/wanna-pee-on-my-wana-sea-urchin-injuries-a-literature-review/.
- 6. De Waal S, Balkhair M, Al-Mashikhi A, Khoom S. Habitat preferences of juvenile abalone (haliotis marae wood, 1828) along the Dhofar coast of Oman and implications for conservation. Agricultural and marine sciences 2012; (17):45-52.
- 7. Rossetto AL, de Macedo Mora J, Haddad Junior V. Sea urchin granuloma. Rev Inst Med Trop Sao Paulo 2006 Sep-Oct;48(5):303-306.
- 8. Kinmont PD. Sea-urchin sarcoidal granuloma. Br J Dermatol 1965 Jul;77:335-343.
- 9. Dahl WJ, Jebson P, Louis DS. Sea urchin injuries to the hand: a case report and review of the literature. Iowa Orthop J 2010;30:153-156.
- Strauss MB, MacDonald RI. Hand injuries from sea urchin spines. Clin Orthop Relat Res 1976 Jan-Feb;(114):216-218.
- 11. Molina-Ruiz AM, Requena L. Foreign body granulomas. Dermatol Clin 2015 Jul;33(3):497-523.
- 12. Ahmad R, Mccann PA. Barakat M, Astle L. Sea urchin spine injuries of the hands. J Hand Surg Am 2008;(33):670-671.
- 13. Nassab R, Rayatt S, Peart F. The management of hand injuries caused by sea urchin spines. J Hand Surg Br 2005 Aug;30(4):432-433.
- 14. Cracchiolo A III, Goldberg L. Local and systemic reactions to puncture injuries by the sea urchin spine and the date palm thorn. Arthritis Rheum 1977 Jul-Aug;20(6):1206-1212.
- 15. Warin AP. Sea-urchin granuloma. Clin Exp Dermatol 1977 Dec;2(4):405-407.