Snow Storm Pattern
A 23 year old Yemeni female presented with 6 month history of progressive shortness of breath. Her chest X-ray (Fig. 1) and chest computed tomography (CT) scan (Fig.1) are shown.

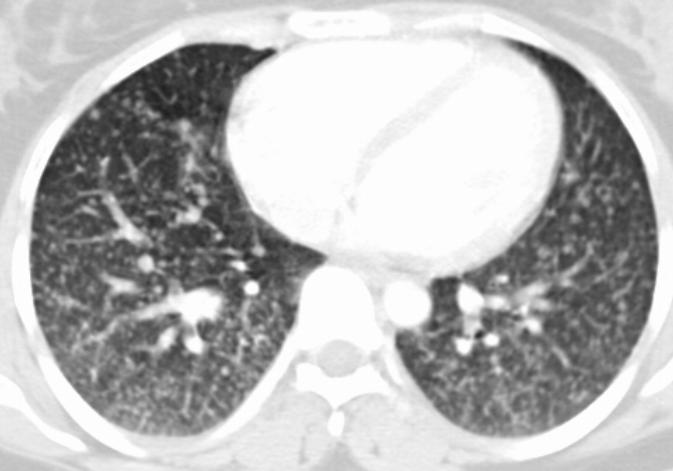
Fig. 1: Chest film (PA view) and axial computed tomography of the chest
show numerous bilateral miliary lung nodules.

Fig. 2: Thyroid scan using I131 shows high uptake within the thyroid gland,
cervical lymph nodes and diffuse uptake in both lungs due to metastasis.
Question
What is the most likely diagnosis?
- Miliary Tuberculosis
- Metastatic carcinoma
- Calcified Varicella infection
- Sarcoidosis
- Alveolar Microlithiasis
Answer
The correct diagnosis of the “Snow Storm” or miliary pattern is compatible with metastatic papillary thyroid carcinoma.
Discussion
The evaluation of diffuse fine nodular patterns on plain films may be difficult because of the small size of the nodules. When they are truly miliary in size (1-2mm), they are marginally detectable radiographically and may require high resolution computed tomography (HRCT) for confirmation. These very small nodules are sometimes more easily appreciated on the PA film in the costophrenic angle and on the lateral film in the retrosternal clear space.
The sharpness of the borders of the nodules is an important criterion for narrowing the differential. If the nodules are ill defined they are more likely to represent involvement of the distal air spaces (acinar rosettes). In such cases, alveolar edema, exudates, or hemorrhage must be considered. In contrast, the pattern of very small but sharply defined or discrete opacities denote that these nodules are more likely interstitial and the above mentioned differential should be considered.
Miliary tuberculosis is the classic example of a disease producing a fine nodular interstitial pattern on radiographic examination of the chest. The most common fungal infection to produce a fine nodular interstitial pattern are histoplasmosis, coccidioidomycosis, and blastomycosis. The development of fine nodular patterns in a patient with a known distant primary tumor, such as a thyroid tumor, strongly suggests disseminated metastatic disease. These patients often have signs of severe systemic illness but careful clinical correlation is required, since many patients with malignant tumors receive chemotherapy with potent immunosuppressing agents. The possibility of opportunistic infection must be ruled out. Other primary tumors that have been observed to lead to this pattern include melanoma, breast carcinoma, and gastrointestinal tumors, including pancreatic carcinoma.
Sarcoidosis and eosinophilic granuloma may produce a fine nodular interstitial pattern, although the patient may have only minimal symptoms of shortness of breath or easy fatigability. Associated bilateral adenopathy or even previous films revealing hilar adenopathy are virtually diagnostic of Sacoidosis.
References
- Radiology Review Manual, 5th Edition, Wolfgang Dahnert
- Chest Radiology: Plain Film Patterns and Differential Diagnosis, 4th Edition, James C. Reed