Road traffic accidents are considered the ninth leading cause of death and account for 2.2% of all deaths globally. Approximately, 1.3 million people die in road traffic accidents each year an average of 3287 deaths/day. It is one of the leading cause of death among young people aged 15–29. In addition, 20–50 million people are injured or disabled. Road traffic accidents cost USD$518 billion globally, costing individual countries from 1–2% of their annual gross domestic product.1
The World Health Organization (WHO) ranked Oman at fourth in the Arabian Gulf Co-operation Council (GCC) states and 57th worldwide as far as the occurrence of traffic accidents, injuries, and deaths.2–4 Oman has the most number of road accidents in the Gulf region. According to 2016 statistics at the GCC secretariat information office based in Muscat, Oman led the way with 4721 accidents followed by Saudi Arabia with 4609, and Qatar with 4322. The number of accidents in Oman was 8.89 per 100 000 people in 2016 compared to 8.71 per 100 000 people in 2015.2–4
In 2010, 820 men, women, and children were killed (30.4 deaths per 100 000 population) due to serious injuries in 50–74% of patients even after transporting by ambulance. 4 There have been nearly 45 000 injured since 2000. The more alarming issue is that the ratio of deaths in a road accident to permanent disability in young people is 2:3.4 Traffic accidents cause great human and economic suffering in Oman putting an immense burden on hospitals and health systems.5 Therefore, prevention of road traffic accidents and associated injuries as well as fatalities has long been a priority issue.5 The Royal Oman Police has engaged in educating the public by organizing GCC traffic week, traffic safety contests, a traffic safety expo, and visiting schools to raise awareness among the people of Oman to drive safely. Accidents rates dropped to 32.8%, from 6279 in 2015 to 4721 in 2016. However, compared to the 675 people who lost their life in road accidents in 2015, 692 died in 2016. However, the number injured fell by 19.2%, from 3624 in 2015 to 2929 in 2016.6 The National Centre for Statistics and Information, reported that the number of road accidents in Oman during the first three months of 2017 declined by 28.8% to 895 from 1257 during the same period in 2016. The number of deaths stood at 150, which is a decrease of 6.3% compared to the same period last year. In March, the governorate of Muscat recorded the highest number of road accidents (27.6%) followed by the governorate of South Al Batinah (20.3%). The governorates of A’Dhahirah and South A’Sharqiyah recorded 11.7% of the total road accidents in Oman.6
The risk factors majorly blamed for road traffic accidents includes high speed, alcohol, talking on cell phones, rash driving, and poor road infrastructures.7,8 However, studies in Oman on the impact of medical conditions and medications on the road traffic safety are limited. This is due to the fact that not all medical conditions increase the risk for road accidents to the same extent and vice versa. The severity of the condition and other characteristics of the disorder are likely to be important determinants of crash risk.7–9 Driving a car under the influence of medication can be unsafe not only for the driver, but also passengers and others who share the road. The coordination, judgment, reaction time, attention, and perception of the driver may be disturbed depending on how specific drugs act on the brain.10,11 About 10% of all people killed or injured in traffic accidents take some type of medicinal agent. However, there is still little evidence that medicinal drugs are causally related to traffic accidents; the percentage of drivers killed and have traces of medicinal drugs in their systems has stayed at about 5%.12
The use of antidepressants, anxiolytics, hypnotics, and psychotropic medications affects the central nervous system and drivers on these medications are at a higher risk for traffic accidents.13 A French study reported that drivers using medications to manage their disabilities increased the risk of compromising traffic safety by 27%.14 A study carried out in West Virginia, USA among elderly drivers showed that the safe driving skills of more than 30% of drivers were effected driving under the influence of medications (such as analgesics and drugs acting on cardiovascular and gastrointestinal systems).15 A registry based cohort study among Norwegians concluded that the risk of road traffic accidents was increased in medication users the first seven days after dispensing.16 A study carried out on prescription medication usage and their influence on road traffic accidents noticed that drivers who used centrally acting drugs had 2.16-times increased risk of accidents.17 Similarly, driving skills are compromised in drivers with chronic medical conditions.18
It is hypothesized that there is an increase in the number of road accidents due to uncontrolled medical conditions and inappropriate medication use. The primary purpose of this study was to retrospectively assess the extent of medical conditions and medications influencing road traffic safety among drivers involved in road accidents who reported to Khoula and Nizwa hospitals, Oman.
Methods
We conducted a hospital-based retrospective study among Omani drivers (injured or non-injured) who reported to the Khoula and Nizwa hospitals following an accident. Information on past medical conditions and medications used by patients before the accident was recorded. All participants aged over 18-years were included in the study. We excluded patients who had an accident due to consumption of alcohol or marijuana as these are not legal medications in Oman.
Information was collected from 951 traffic incident victims admitted from November 2016 to June 2017 (i.e., a period of eight months including the holy month of Ramadan) using the Al-Shifa database available at Accident and Emergency Departments of the selected hospitals. We collected information on the patient’s medication, medical conditions, and other demographics. About 2% of randomly selected patients were contacted over the phone to confirm their health state and what medications were taken before the accident.
The study was initiated after getting the permission from the Ministry of Health Oman Ethics Committee, and the ethical committees of Khoula Hospital, Nizwa Hospital, and Oman Medical College. The identity of the participants and findings were treated with the highest possible degree of confidentiality and privacy.
The data was collected on monthly basis and each case was given a number when it was entered into the Excel sheet. Statistical analyses of data were performed using SPSS (Statistics IBM Corp. Released 2015. IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp). Distribution of medical conditions and medications in patients involved in traffic accidents were determined. The correlation of these factors with the traffic accident was also determined. The frequency and percent of data was computed and presented in the form of tables and charts.
Results
The majority of victims in the study population were from Khoula Hospital (78.0%) while 22.0% were from Nizwa Hospital. Accident cases were greater in Khoula Hospital because it is located in the capital of Oman where the population is larger compared to Nizwa. In addition, the study period in Khoula Hospital was eight months and in Nizwa Hospital was only five months due to transportation difficulties. The majority (72.0%) of the study population was male while 28.0% were female. The majority (95.6%) of accidents were recorded in car drivers, and 4.3% in commercial motor vehicles.
The study results show that 92.4% of the victims had no any prior medical conditions; 7.6% of the victimized drivers had a history of medical conditions. Hypertension and diabetes mellitus were equally counting for 72.2% of total cases followed by asthma (12.5%) and anemia (6.9%). Hypertension and diabetes mellitus (lifestyle diseases) are known to be the most threatening diseases in Oman [Figure 1].
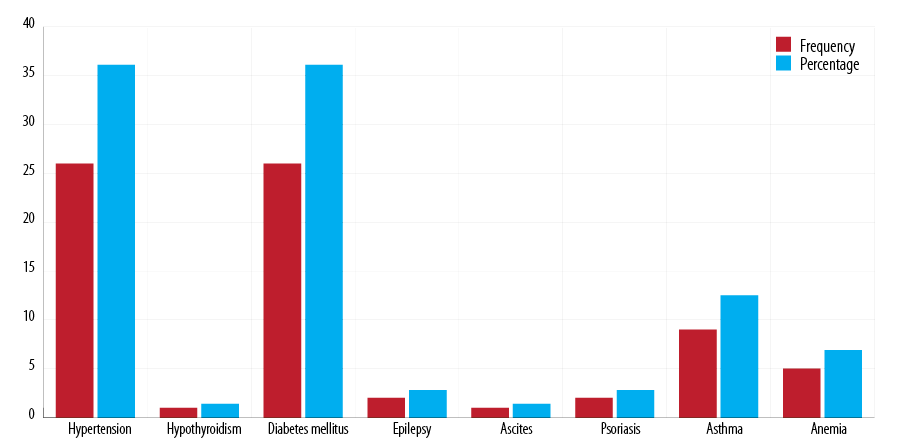
Figure 1: Frequency of medical condition associated with road traffic accident victims.
The study population was divided into four age groups. The total cases were correlated to the medical conditions with respect to age groups. The percentage of total medical conditions in young drivers (18–29 years) was 2.9%. The 30–39 year age group showed a percentage of 2.8%. The drivers who belonging to the 40–49 year age group accounted for 15.7% of cases. Older victimized drivers (≥ 50 years) showed the highest percentage of the medical conditions (45.1%) with a correlation found between this age group and road traffic accidents. Diabetes mellitus (46.9%) and hypertension (40.6%) were the most common medical conditions in this age group [Table 1]. Overall, 96% of victimized drivers were reported to take no prior medications. The remaining 4% were on medications; insulin (9.4%) and metoclopramide, thyroxine, and amlodipine (6.3% each). Other medications (not specified due to the lack of information on Al-Shifa database) contributed to 40.6% of cases, and medications such as gabapentin, fentanyl, heparin, eltroxin, warfarin, cortisol, lisinopril, atorvastatin, carvidelol, and salbutamol were 3.1% each [Figure 2].
Table 1: Relative risk in study group.
|
18–29 |
15/510 × 100 = 2.9% |
|
30–39 |
7/246 × 100 = 2.8% |
|
40–49 |
18/115 × 100 =15.7% |
|
> 50 |
32/71 × 100 = 45.1% |
|
Hypertension |
13/32 × 100 = 40.6% |
|
Diabetes mellitus |
15/32 × 100 = 46.9% |
|
Epilepsy |
1/32 × 100 = 3.1% |
RTA: road traffic accidents.
In 4.1% of cases symptoms were felt by the drivers prior to the accident; loss of control was the major symptom (38.5%) followed by dizziness (25.6%), sleep amnesia (10.3%), and blurred vision (7.7%). Other effects blamed by drivers include vertigo, phonophobia, photophobia, back pain, loss of sensation, and headache accounting for 17.9% of cases. Loss of control and dizziness could be related to unmanaged or uncontrolled diabetes mellitus. Hypertension can be linked to migraine-like attack (photophobia, phonophobia, headache, and vertigo) [Figure 3].
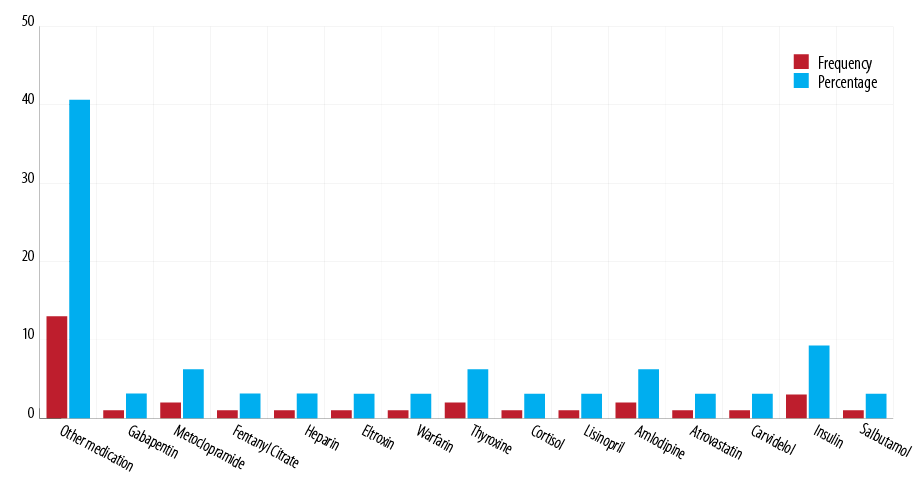
Figure 2: Frequency and percentage of medications taken by road accident victims.
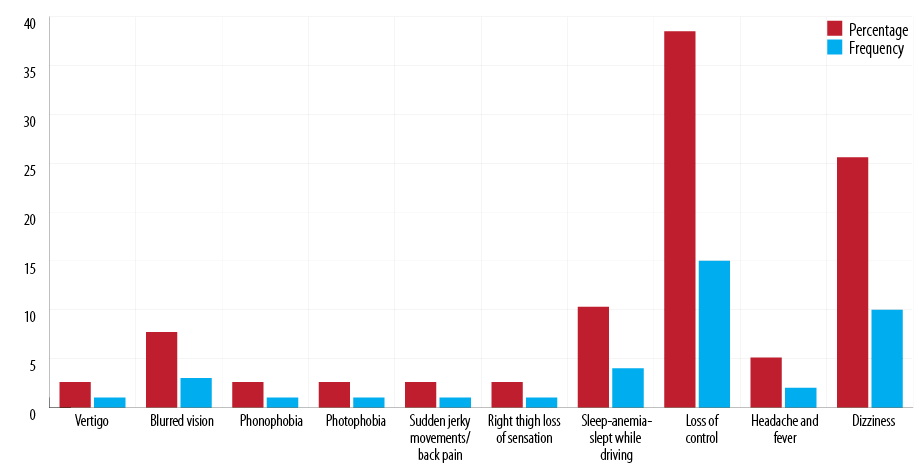
Figure 3: Frequency of symptoms reported by drivers involved in road accidents.
Discussion
The objective of this study was to know the influence of medications and medical conditions among victimized drivers. However, further extension of this study involving more cases, prospectively and retrospectively, will provide concrete evidence on the impact of medical conditions and medications on road traffic safety. The present study is an extension of previous studies carried out in Oman to understand the pattern, type, and severity of accident injuries and utilization of medicines among patients with road traffic accident injuries.19–21
Most of the study population reported to Khoula Hospital (78%), which is likely due to the fact that accident cases are greater in the capital. Results show that 72.0% of the study population were males, similar to the numbers reported in earlier studies.22 The majority (95.6%) of accidents were recorded in car drivers as cars are the preferred mode of transportation in Oman.23
There is a concern on growing incidence of road traffic accidents due to medical diseases and disorders.24 In a US study, 8% of the study population was reported to have prior medical conditions whereas 92% had no prior medical conditions. These results support a Canadian study, which reported that an increasing trend in the incidence of chronic medical conditions, their combinations, and severity will compromise road traffic safety.25
A study carried out in Finland revealed a higher incidence of road traffic accidents among drivers with a history of arterial hypertension.25 Multiple studies have shown an increase in the risk of road traffic accidents in drivers with a history of diabetes and its complications.26,27 The chronicity of diabetes is known to be associated with retinopathy, neuropathy, hypoglycemia, hyperglycemia, cataract, and cardiovascular complications, which affect driving skills.28,29 In our study, 2% of the study population had a history of hypertension and 3% had a history of diabetes mellitus followed by asthma supporting earlier studies30,31 correlating the medical conditions to road traffic accidents in the > 50 age group. The effect of these medical conditions on driving could be due to their complications such as fatigue, visual problems, or numbness in the extremities.28,32
Another important part of the study was to investigate the influence of medications on driving skills and road traffic safety. Only 4% of drivers were on medications. The most common medication was insulin followed by antihypertensives. Other medications were thyroxin, atorvastatin, asthma inhalers, anticoagulants, metoclopramide, cortisol, fentanyl citrate, and gabapentin. A study carried out in Norway reported an increase in risk of road traffic accident due to use of insulin.33 The risk of insulin use in relation to its influence on road traffic safety is thought to be due to hypoglycemic side effects.26
Road accident drivers have reported symptoms prior to accidents such as loss of control, dizziness, migraine-like attack, and sleep amnesia. Loss of control, dizziness, and sleep amnesia could be related to unmanaged or uncontrolled diabetes. Hypertension could be linked to onset of a migraine-like attack (photophobia, phonophobia, headache, and vertigo) and headache affecting driving skills. These results substantiate earlier studies28–29,32–34 and supports educating drivers to the risks of taking medications before dispensing them and using appropriate labeling.34,35 The relative risk analysis among the population indicates that the drivers in the 40–49 year age group36 make up 15.6% of the medical condition cases, and those ≥ 50 years old have the highest percentage of medical conditions (45%).
There are some limitations that should be considered with this study: the study was carried out over different time periods (over a short period) in selected study centers; the study was retrospective; data was analyzed by correlation analysis ( which does not establish causal relationships); cases were reported at selected hospitals not the nearest residential health institute; limited number of cases considered; and we were missing large amount of data on medication use.
Conclusion
Diabetes and hypertension were the most common medical conditions, and insulin and antihypertensives were the most common category of medications influencing safe driving skills of Omani drivers. Possibly due to loss of control, dizziness, migraine-like attack, and sleep amnesia as the symptoms of medical conditions and/or side effects of medications use.
Disclosure
The authors declared no conflict of interest. No funding was received for this study.
Acknowledgements
We would like to thank Ms. Zakia and Ms. Zwaina the chief nurse in the Accident and Emergency Department of Khoula Hospital for their help in collecting the data. We also appreciate the help of other clinical, paraclinical, and non-clinical staff from Nizwa Hospital in the Emergency Department for their timely support in collecting the data.
references
- 1. Salari M, Kazemnejad A, Zayeri F. Using Growth Mixture Modeling for Clustering Asian and North African Countries on the Road Injury Death Trend (1990-2010). Oman Med J 2017 Sep;32(5):417-424.
- 2. World Health Organization. Violence and Injury Prevention. Global status report on road safety. WHO, Geneva, Switzerland. 2009 [cited 2017 December]. Available from: http://www.who.int/violence_injury_prevention/road_safety_status/2009/en/.
- 3. Al Harrasi EH, Jrew B, Abojaradeh M. Development of traffic accident models in Sultanate of Oman. 7th Traffic Safety Conference; 2015 May 12-13; Amman, Jordan.
- 4. World Health Organization. Department of Violence and Injury Prevention and Disability. Global status report on road safety 2013: Supporting a decade of action. Geneva; 2013.
- 5. Al-Riyami A. Health vision 2050 Oman: A committed step towards reforms. Oman Med J 2012 May;27(3):190-191.
- 6. Bhattacharjee M. 33.3% Decline in road accidents till march: National Centre for Statistics and Information, Royal Omani Polices 2018. Muscat Daily [cited 2018 April 23]. Available from: https://www.muscatdaily.com/Archive/Oman/33.3-decline-in-road-accidents-till-March-NCSI-58ks.
- 7. Peden M, Toryan T, Harvey A, Bartolomeos Ki, Laych K. Global status report on road safety: Time for action. World Health Organization: Geneva; 2015.
- 8. Moafian G, Aghabeigi MR, Heydari ST, Hoseinzadeh A, Lankarani KB, Sarikhani Y. An epidemiologic survey of road traffic accidents in Iran: analysis of driver-related factors. Chin J Traumatol 2013;16(3):140-144.
- 9. Charlton J, Koppel S, O’Hare M, Andrea D, Smith G, Khodr B, et al. Influence of chronic illness on crash involvement of motor vehicle drivers. 2nd ed. Monash University, Accident Research Centre. Wellington Road: Clayton, Australia; 2010.
- 10. Orriols L, Salmi LR, Philip P, Moore N, Delorme B, Castot A, et al. The impact of medicinal drugs on traffic safety: a systematic review of epidemiological studies. Pharmacoepidemiol Drug Saf 2009 Aug;18(8):647-658.
- 11. National Institute on Drug Abuse. Drugged Driving, Drug Facts. 2016 [cited 2017 December 12]; p. 1-6. Available from: https://www.drugabuse.gov/publications/drugfacts/drugged-driving.
- 12. Gemmell C, Moran R, Crowley J, Courtney R. Literature review on the relation between drug use, impaired driving and traffic accidents. EMCDDA Final Report, European Monitoring Centre for Drugs and Drug Addiction; 1999. p. 12-50.
- 13. Ravera S, van Rein N, de Gier JJ, de Jong-van den Berg LT. Road traffic accidents and psychotropic medication use in The Netherlands: a case-control study. Br J Clin Pharmacol 2011 Sep;72(3):505-513.
- 14. Orriols L, Delorme B, Gadegbeku B, Tricotel A, Contrand B, Laumon B, et al; CESIR research group. Prescription medicines and the risk of road traffic crashes: a French registry-based study. PLoS Med 2010 Nov;7(11):e1000366.
- 15. Rudisill TM, Zhu M, Davidov D, Leann Long D, Sambamoorthi U, Abate M, et al. Medication use and the risk of motor vehicle collision in West Virginia drivers 65 years of age and older: a case-crossover study. BMC Res Notes 2016 Mar;9:166.
- 16. Engeland A, Skurtveit S, Mørland J. Risk of road traffic accidents associated with the prescription of drugs: a registry-based cohort study. Ann Epidemiol 2007 Aug;17(8):597-602.
- 17. Dischinger P, Li J, Smith GS, Ho S, Auman K, Shojai D. Prescription medication usage and crash culpability in a population of injured drivers. Ann Adv Automot Med 2011;55:207-216.
- 18. Dischinger PC, Ho SM, Kufera JA. Medical conditions and car crashes. Annu Proc Assoc Adv Automot Med 2000;44:335-346.
- 19. Chitme HR, Kashmiri AA, Amri FM, Haidar AK, Ajmi AM, Saiari YA. Assessment of type and severity of road traffic accident injuries among Omani young adults. Saudi Journal of Medical and Pharmaceutical Sciences 2017;3(10):60-68.
- 20. Chitme HR, Al Harbi M, Al Saadi TS. Pattern of road traffic accident injuries in young adults. World Journal of Pharmaceutical Research 2015;4(4):313-323.
- 21. Chitme HR, Al Badri MMS, Al Saadi AH. Utilization of drugs in patients with road traffic accident injuries. Int J Nutr Pharmacol Neurol Dis 2017;7(1):8-11.
- 22. Koisaari T, Michelsson K, Holopainen JM, Maksimainen R, Päivänsalo J, Rantala K, et al. Traffic and criminal behavior of adults with attention deficit-hyperactivity with a prospective follow-up from birth to the age of 40 years. Traffic Inj Prev 2015;16(8):824-830.
- 23. Al-Reesi H, Ganguly SS, Al-Adawi S, Laflamme L, Hasselberg M, Al-Maniri A. Economic growth, motorization, and road traffic injuries in the Sultanate of Oman, 1985-2009. Traffic Inj Prev 2013;14(3):322-328.
- 24. Naumann RB, Dellinger AM, Zaloshnja E, Lawrence BA, Miller TR. Incidence and total lifetime costs of motor vehicle-related fatal and nonfatal injury by road user type, United States, 2005. Traffic Inj Prev 2010 Aug;11(4):353-360.
- 25. Marshall SC, Man-Son-Hing M. Multiple chronic medical conditions and associated driving risk: a systematic review. Traffic Inj Prev 2011 Apr;12(2):142-148.
- 26. Rainio J, Sulander P, Hantula L, Nuutinen J, Karkola K. Diseases and motor vehicle fatalities in Finland in 2001 and 2002. Traffic Inj Prev 2007 Sep;8(3):321-328.
- 27. Ahmed AA. Hypoglycemia and safe driving. Ann Saudi Med 2010;30(6):464-467.
- 28. Senra Moniz C, Alves Serra F, Costa Ferreira R, Vasconcelos C, Machado Saraiva A. [Diabetes and driving: evidence and recommendations]. Acta Med Port 2013 Jul-Aug;26(4):428-432.
- 29. Gjerde H, Christophersen AS, Normann PT, Mørland J. Toxicological investigations of drivers killed in road traffic accidents in Norway during 2006-2008. Forensic Sci Int 2011 Oct;212(1-3):102-109.
- 30. Smolensky MH, Di Milia L, Ohayon MM, Philip P. Sleep disorders, medical conditions, and road accident risk. Accid Anal Prev 2011 Mar;43(2):533-548.
- 31. Laubichler W, Haberl J. [Causes and incidence of traffic accidents caused by precipitous disorders of consciousness and illnesses of drivers. A one year study in Upper Austria and Salzburg]. Blutalkohol 1989 Jan;26(1):7-14.
- 32. Brož J, Kriváňová LS, Fedáková Z, Petrosyan L, Kvapil M, Polák J. [Motor vehicle driving and diabetes mellitus - medical aspects]. Vnitr Lek 2016 Mar;62(3):223-225.
- 33. Skurtveit S, Strøm H, Skrivarhaug T, Mørland J, Bramness JG, Engeland A. Road traffic accident risk in patients with diabetes mellitus receiving blood glucose-lowering drugs. Prospective follow-up study. Diabet Med 2009 Apr;26(4):404-408.
- 34. Veldhuijzen DS, van Wijck AJ, Verster JC, Kalkman CJ, Kenemans JL, Olivier B, et al. The impact of chronic pain patients’ psychotropic drug knowledge and warning labels on the decision whether to drive a car or not. Traffic Inj Prev 2006 Dec;7(4):360-364.
- 35. Satake M. Pharmacists’ advice about driving for diabetic patients. Yakugaku Zasshi 2017;137(3):329-335.
- 36. Ma L, Yan X. Examining the nonparametric effect of drivers’ age in rear-end accidents through an additive logistic regression model. Accid Anal Prev 2014 Jun;67:129-136.