Influenza is a highly infectious disease caused by three types of influenza virus: A, B, and C. Influenza A infects humans and other animals causing moderate to severe illness in all age groups. Influenza B affects only humans causing milder disease. Influenza C is rarely reported as a cause of human illness.1
The World Health Organization (WHO) Region for the Eastern Mediterranean, given its location under several migratory bird flyways, is an important region for influenza research and surveillance. Countries in the region include Afghanistan, Bahrain, Djibouti, Egypt, Iran, Iraq, Jordan, Kuwait, Lebanon, Libya, Morocco, Oman, Pakistan, Palestine, Qatar, Saudi Arabia, Somalia, Sudan, Syrian Arab Republic, Tunisia, the United Arab Emirates, and Yemen. These countries lie under four of the eight global migratory bird flyways: Central Asia–India, West Asia–Africa, Mediterranean–Black Sea, and East Atlantic.2
Annually, influenza viruses circulate worldwide, causing substantial illness and death leading to considerable economic losses.3 Influenza A (H1N1 and H3N2) and influenza B viruses are the current subtypes of seasonal influenza viruses circulating in humans.4 The Eastern Mediterranean Region (EMR) is affected seasonally with influenza, with the majority of countries having a pattern of infection similar to other northern hemisphere countries peaking in the winter. However, due to their geographic location and spread, some countries (such as Qatar and Oman) have a tropical-like pattern with two peaks per year.
At the end of April 2009, an outbreak of influenza of a new type of A/H1N1 started in Mexico and the United States of America.5 The virus then spread throughout the world, causing a pandemic. Most reported cases at the time in the WHO EMR were in Saudi Arabia (14 500 cases) followed by Kuwait, Egypt, and Oman (6 000–8 000 cases). The number of fatalities in the EMR later rose to 1 018.6 More than 500 H1N1 sequences have been generated and published from several EMR countries since.
In response to the pandemic, several countries initiated vaccination campaigns in selected priority groups.7 Saudi Arabia put in place a preparedness plan that ensured the optimum provision of health services for pilgrims and minimal disease transmission on their return home.8 H1N1 is now in the post-pandemic period and has become a seasonal influenza virus that continues to circulate with localized outbreaks of varying magnitude.9
Avian influenza A virus subtypes H5, H7, and H9 have also been reported to cause human infections, given their ability to cross the species barrier and further replicate in humans.10 The EMR includes countries where avian influenza viruses, including the highly pathogenic H5N1 and H9N2, are endemic in the domestic poultry populations.
Highly pathogenic H5N1 received considerable attention as an emerging virus with human pandemic potential.11,12 In contrast to its serious impact on domestic poultry, however, few human cases have been confirmed. To date, 844 human H5N1 cases have been documented, of which 449 (53.19%) were fatal.13 The burden of H5N1 on human health in EMR countries is significant. So far, 353 confirmed cases and 118 fatalities have been reported in Djibouti, Egypt, Iraq, and Pakistan.13 Almost all cases of H5N1 infection in humans have been associated with close contact with infected live or dead birds, or H5N1-contaminated environments.14 H9N2 viruses are endemic in the poultry in several countries. Seroepidemiologic studies from Egypt, Lebanon, and Iran have documented evidence of H9N2 antibodies in humans.15–17 Egypt was the first country in the EMR to confirm human infection with H9N2.
A previous literature review up to 2012 showed that in some countries of the EMR, influenza research is growing and diverse. Research covered epidemiologic, veterinary, and basic science aspects. However, the volume and diversity of influenza research was low, especially in light of the burden of influenza in the region.2
Given the importance of influenza infection, we conducted a comprehensive literature review to understand the current status of influenza research in the WHO EMR. We aimed to detect whether any changes in influenza research occurred after 2012. We also expanded the search to include the grey literature, reported outbreaks, and generated sequences.
We used PubMed, Scopus, and Google Scholar to search the peer-reviewed literature using the search terms “Influenza” and “Country Name” [Figure 1]. An additional search term, “Influenza” and “Middle East,” was also used to avoid excluding any multinational publications. An alternative country name was also used for certain countries to avoid excluding publications when, for instance, the French name of the country was commonly used. These alternative names were Liban for Lebanon, Maroc for Morocco, Gaza and West Bank for Palestine, Syria for the Syrian Arab Republic, Tunisie for Tunisia, and Emirates and UAE for the United Arab Emirates. The search was restricted to records published after 2012.
We attempted to include the grey literature in our search given the fact that the published scientific research from the region was sparse. The first source for gray literature was Google Scholar. This search engine is important in some countries of the EMR and is widely used. For example, in Egypt university scientific committees monitor and evaluate researchers linked to official research centers or universities via registration into Google Scholar. Moreover, the manual addition option in Google Scholar permits researchers to add their local publications, hence expanding visibility. The second source for gray literature was searching for graduate student dissertations. This was done by searching the official websites of universities in the EMR using the search term “Influenza” for all dissertations from 2012 onwards [Figure 1].
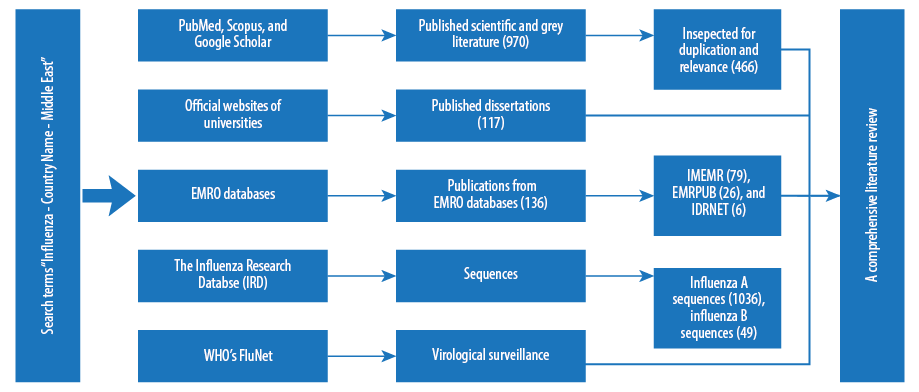
Figure 1: Search strategy flowchart.
Furthermore, we searched the websites of ministries of health and agriculture as well as WHO online regional databases for published articles and reports using a single search term “Influenza”.
The WHO databases included the Index Medicus for the Eastern Mediterranean Region (IMEMR), WHO publications (EMRPUB), and the Institutional Digital Repository (IDRNET) [Figure 1].
Finally, the Influenza Research Database (IRD) (www.fludb.org), a National Institutes of Health database dedicated to influenza and linked to GenBank, was used. A nucleotide sequence search was conducted for all species of influenza, all hosts, all segments, and all countries in the EMR since 2012. WHO’s FluNet was searched, and virological surveillance charts for all available data from participating countries were downloaded [Figure 1].
Published scientific and grey literature
The initial literature search yielded a total of 970 records; these were compiled into three different libraries using EndNote X7 software. We obtained 362 records from PubMed, 294 from Scopus, and 314 from Google Scholar. Records were inspected for relevance individually by reading the abstract, and then the three libraries were merged into one final library and inspected again for duplication. A total of 543 records were retained, which were checked again for relevance, and only those that were influenza research papers from the WHO EMR were retained. A total of 466 records were analyzed by reading the abstracts of the retained records by one of the authors and verified by another author. Records from Google Scholar showed that 108 of 209 records were gray literature publications.
Published scientific and grey literature findings by country, type, and date
Five countries appeared to have active influenza research groups, producing more than 85.0% of the published influenza research [Table 1]. Iran had the highest number of publications with 147 records, followed by Egypt with 128 records, Saudi Arabia with 63 records, Pakistan with 43 records, and Morocco with 17 records. No records were found for Djibouti, Somalia, or Palestine.
Table 1: Publications from the Eastern Mediterranean Region (EMR).
|
Afghanistan |
2 |
- |
- |
- |
- |
|
Bahrain |
1 |
- |
2 |
- |
- |
|
Djibouti |
0 |
- |
- |
- |
- |
|
Egypt |
128 |
105 |
12 |
699 |
- |
|
Iran |
147 |
- |
28 |
198 |
39 |
|
Iraq |
6 |
1 |
1 |
3 |
- |
|
Jordan |
4 |
- |
1 |
- |
- |
|
Kuwait |
6 |
- |
3 |
- |
- |
|
Lebanon |
5 |
- |
- |
11 |
- |
|
Libya |
3 |
- |
- |
4 |
- |
|
Morocco |
17 |
- |
- |
19 |
10 |
|
Oman |
6 |
- |
1 |
91 |
- |
|
Pakistan |
43 |
1 |
4 |
- |
- |
|
Palestine |
0 |
- |
- |
- |
- |
|
Qatar |
7 |
- |
- |
- |
- |
|
Saudi Arabia |
63 |
4 |
27 |
- |
- |
|
Sudan |
5 |
6 |
- |
- |
- |
|
Somalia |
0 |
- |
- |
- |
- |
|
Syria |
1 |
- |
- |
- |
- |
|
Tunisia |
8 |
- |
- |
7 |
- |
|
UAE |
5 |
- |
- |
4 |
- |
|
Yemen |
1 |
- |
- |
- |
- |
|
Middle East* |
8 |
- |
32 |
- |
- |
*Publications from more than one country or intercountry meeting reports.
Most of the published research comprised epidemiological research and basic virology papers. Epidemiology papers constituted 30.3% with 141 records [Figure 2]. On close inspection, most of these were descriptive clinical epidemiology papers describing cases of influenza in hospitalized populations, complications of influenza or influenza as a cause (among other agents) of respiratory tract infections. Very few had an analytical epidemiology design or were reporting controlled trials or clinical trials.
Basic virology papers constituted a major portion of reviewed research (29.6%) with 138 records [Figure 2]. The majority of these papers experimented with H5N1, H9N2, or pandemic H1N1 viruses. Most research was directed towards molecular and phylogenetic analyses of these viruses. Some explored the pathogenicity of avian influenza viruses in poultry, and a few experimented with antiviral resistance, development of vaccines and diagnostic techniques, as well as studying vaccine efficacy, research which has more immediate impact on public veterinary health.
There were 71 (15.2%) records for epizootiology research [Figure 2]. Most papers found described the prevalence and cocirculation of H5 or H9 viruses among poultry and wild birds. A handful looked at other species (equine, canine, porcine, and feline).
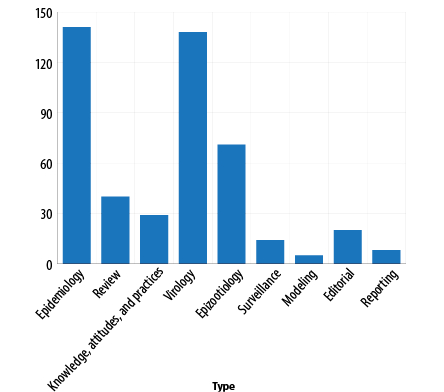
Figure 2: Database records from the Eastern Mediterranean Region according to type.
Reviews, editorials, opinion, case reports and papers on knowledge, attitude and practice constituted about 24.8% of published research. Although such papers may have an immediate impact on policy- and decision-making, they remain descriptive and would be of limited research value. Papers showing results of surveillance among birds or humans were very limited.
The highest volumes of influenza research were in 2014 with 143 records (30.6%) and in 2012 with 137 records (29.3%). There were 109 records for 2013 and 77 for 2015.
Published dissertations from EMR countries
A total of 117 dissertations were found from five countries. Another spreadsheet was created for dissertations containing the following data: title, author, type (MSc or Ph.D), university, faculty, department or specialty, and date.
Capturing published dissertations was more feasible for some countries than others. Factors such as university regulations in countries where all student dissertations are deposited online, for example, Egypt, helped bring these dissertations into the public domain. Egypt was the leading country in this respect with a large number (105 out of 117 found) of published dissertations [Table 1]. Dissertations from Iraq, Saudi Arabia, Pakistan, and Sudan were also found. None were found from other countries.
Publications from EMRO databases
The initial database search yielded a total of 136 records: 104 from IMEMR, 26 from EMRPUB, and six from IDRNET. After inspection for relevance, 111 records were retained; 79 from IMEMR, 26 from EMRPUB, and six from IDRNET.
EMRO databases publications findings by country and date
Iran and Saudi Arabia lead the other countries with 28 (25.2%) and 27 (24.3%) records, respectively, followed by Egypt with 12 (10.8%) records [Table 1]. The highest publication number was recorded for 2012 with 39 (49.3%) records. A total of 26 records were captured from EMRPUB representing notification of new influenza cases, recommendations on seasonal influenza vaccines and consultation on the estimation of the burden of influenza in the region. The IDRNET search yielded a total of six records, all intercountry meeting reports.
Sequences
Searching the IRD database for published influenza sequences since 2012 yielded 1 036 influenza A sequences, 49 influenza B sequences, and 0 influenza C sequences. Table 1 shows the distribution of influenza A sequences by country. The largest proportion was from Egypt with 699 published sequences. These sequences were mostly from avian H5N1 and H9N2 viruses. Iran contributed 198 sequences, most of which were from human influenza A viruses, with only 17 from avian H9N2 viruses. A number of countries published less than 20 sequences, and none were found from the other EMR countries. It is worth noting that 75% of the sequences were complete gene sequences, thus having added value by enabling not only diagnostics but also research.
Of the 1 036 sequences published, 320 were for human viruses and the rest were from animal hosts. Among avian viruses, H5N1 had 357 sequences, and H9N2 had 355 sequences. Other subtypes were not reported, indicating a lack of surveillance in wild birds. Although the majority of the published sequences were for the HA gene (368) or the NA gene (127), almost half were from internal genes, showing that researchers are generating sequences for research rather than just for diagnostics. Only two countries published the influenza B sequences: Iran (39 sequences) and Morocco (10 sequences).
Virological surveillance
Reviewing virological data available on WHO’s FluNet between week 30 of 2014 and week 29 of 2015 (http://www.who.int/influenza/gisrs_laboratory/flunet/en/) reveals that seasonal influenza A and B viruses contribute to the burden of disease and also showed the significance of human H5N1 infection in the EMR. We then searched FluNet for countries of the EMR reporting data and found that the following countries were contributing: Afghanistan, Bahrain, Egypt, Iran, Iraq, Jordan, Morocco, Oman, Pakistan, Qatar, Syria, and Tunisia. The data are typically contributed by the national influenza centers or the central laboratories of reporting countries [Figure 3].
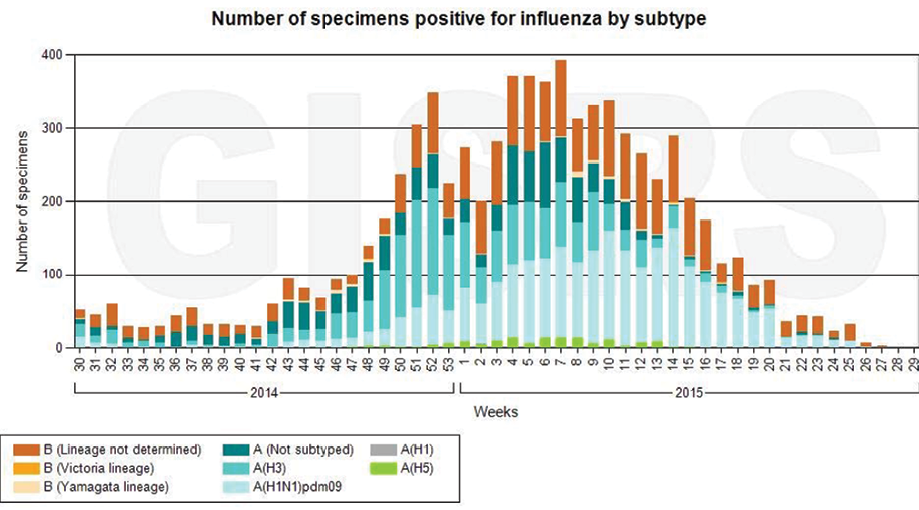
Figure 3: Human influenza activity in the Eastern Mediterranean Region: number of positive specimens according to virus subtype, 2014–2015. http://www.who.int/influenza/gisrs_laboratory/flunet/en/.
Discussion
Influenza research gained more momentum recently with almost 400 research papers published from the EMR; however, many gaps remain. Although five countries appeared to have active influenza research, most of the publications came from only two countries: Iran and Egypt.
Most published papers lacked an advanced study design as was evident by the descriptive nature of epidemiological studies. This was also demonstrated by the fact that many basic science papers focused on the simple task of analyzing the molecular and phylogenetic characteristics of circulating viruses, but did not answer specific viral evolution and ecology questions. Very few papers focused on the burden of influenza.
The previously published literature review reported systematic surveillance in humans and animals was lacking.2 This type of study remains insufficient and not equal to the burden of disease in the region. Although the concern caused by the continuous H5N1 circulation in the region, very limited studies were conducted at the human-animal interface, hence little is known about the extent of avian-to-human transmission of H5N1 in the region.
There is dearth of virological samples from the region that are being tested, typed, and subtyped. This indicates that too little virological surveillance. However, more sequences are being generated each year not only for diagnostic purposes (partial HA and NA): they are also essential for research (complete gene sequences and full genomes). The submitted data originated from very few countries, mostly Egypt and Iran.
Many graduate students are conducting their dissertation research on influenza. This indicates that there is a cohort of interested young scientists in the region. Apart from Egypt, very few dissertations focusing on influenza were recorded from other countries. This might be the case due to the dissertation work not finding its way into the public domain. Therefore, publishing dissertations on an online portal is very useful in bringing graduate studies’ research to light. This can be encouraged in other countries.
Conclusions
Influenza research in the EMR requires a boost to tally with the real burden of the disease in the region. This can be fulfilled by conducting systemic surveillance and research at the human-animal interface especially in countries where H5N1 and H9N2 are endemic. Establishing a regional center of excellence for influenza research and surveillance tasked with setting research priorities, increasing collaboration, and providing support to countries and research groups is recommended.
Disclosure
The authors declared no conflicts of interest. This research was supported by funding from the WHO Regional Office for the Eastern Mediterranean.
references
- 1. CDC. Epidemiology and prevention of vaccine-preventable disease: influenza. 13th ed. Textbook TPBC; 2015.
- 2. Kayali G, Webby RJ, Samhouri D, Mafi AR, Bassili A. Influenza research in the Eastern Mediterranean Region: the current state and the way forward. Influenza Other Respir Viruses 2013 Nov;7(6):914-921.
- 3. Molinari NA, Ortega-Sanchez IR, Messonnier ML, Thompson WW, Wortley PM, Weintraub E, et al. The annual impact of seasonal influenza in the US: measuring disease burden and costs. Vaccine 2007 Jun;25(27):5086-5096.
- 4. Zhand S, Tabaraei A, Moradi A, Fotoohi F, Javid N, Bazoori M, et al. Detection of seasonal influenza H1N1 and H3N2 viruses using RT-PCR assay during 2009 flu pandemic in Golestan Province. Medical Laboratory Journal 2014;8(2):27-32.
- 5. Centers for Disease Control and Prevention (CDC). Swine influenza A (H1N1) infection in two children–Southern California, March-April 2009. MMWR Morb Mortal Wkly Rep 2009 Apr;58(15):400-402.
- 6. Gambotto A, Barratt-Boyes SM, de Jong MD, Neumann G, Kawaoka Y. Human infection with highly pathogenic H5N1 influenza virus. Lancet 2008 Apr;371(9622):1464-1475.
- 7. Global survey on National Vaccine Deployment and Vaccination Plans for pandemic A (H1N1) 2009 vaccine – 2010 Report of Findings World Health Organization. May 2013 [cited Dec 2015]. http://www.who.int/influenza_vaccines_plan/resources/2010_H1N1_NVDP_WHO_Survey.pdf
- 8. Memish ZA, McNabb SJ, Mahoney F, Alrabiah F, Marano N, Ahmed QA, et al; Jeddah Hajj Consultancy Group. Establishment of public health security in Saudi Arabia for the 2009 Hajj in response to pandemic influenza A H1N1. Lancet 2009 Nov;374(9703):1786-1791.
- 9. WHO. H1N1 in post-pandemic period 2010 [cited August 2010]. Available from: http://www.who.int/mediacentre/news/statements/2010/h1n1_vpc_20100810/en/.
- 10. Khanna M, Kumar P, Choudhary K, Kumar B, Vijayan VK. Emerging influenza virus: a global threat. J Biosci 2008 Nov;33(4):475-482.
- 11. Guan Y, Poon LL, Cheung CY, Ellis TM, Lim W, Lipatov AS, et al. H5N1 influenza: a protean pandemic threat. Proc Natl Acad Sci U S A 2004 May;101(21):8156-8161.
- 12. Webby RJ, Webster RG. Are we ready for pandemic influenza? Science 2003 Nov;302(5650):1519-1522.
- 13. Cumulative number of confirmed human cases of avian influenza A (H5N1) reported to WHO. WHO Influenza. 2015 [cited Dec 2015]. Available from: http://www.who.int/influenza/human_animal_interface/H5N1_cumulative_table_archives/en/.
- 14. WHO. Avian influenza A(H5N1) in Egypt 2015 [cited March 2015]. Available from: http://www.emro.who.int/surveillance-forecasting-response/surveillance-news/h5n1-egypt-march-2014.html.
- 15. Azizpour A, Azizpour Y, Habibzadeh S, Faraji P, Tamook A, Vosoghi E, eds. A serological study of antibodies to H9N2 Avain Influenza Virus in Human Population of Ardabil area, Iran. The 13th Iranian & The Second International Congress of Microbiology; 2012.
- 16. Gomaa MR, Kayed AS, Elabd MA, Zeid DA, Zaki SA, El Rifay AS, et al. Avian influenza A(H5N1) and A(H9N2) seroprevalence and risk factors for infection among Egyptians: a prospective, controlled seroepidemiological study. J Infect Dis 2015 May;211(9):1399-1407.
- 17. Barbour EK, Sagherian VK, Sagherian NK, Dankar SK, Jaber LS, Usayran NN, et al. Avian influenza outbreak in poultry in the Lebanon and transmission to neighbouring farmers and swine. Vet Ital 2006 Apr-Jun;42(2):77-85.