A solitary nodule in the paratracheal region usually points towards a thyroid lesion. In an elderly patient, accompanying symptoms may include dysphagia, hoarseness, or a globus sensation in the throat. It may appear as an incidental finding on inspection or after an ultrasonography scan of the neck. However, an asymptomatic anterior neck swelling, which is pulsatile, may not always be a thyroid nodule. The presence of pulsation should raise some suspicion of vascular anomalies. Fine needle aspiration (FNA) or any invasive surgical investigation such as excisional biopsy could result in catastrophic complications.
Case Report
A 65-year-old female with underlying bronchiectasis was referred to our otorhinolaryngology clinic for further management of a right solitary thyroid nodule. The patient complained of a painless anterior neck mass for the past 10 years that had been slowly increasing in size. She denied any associated symptoms. There was no history of dysphagia, odynophagia, or hoarseness. According to her, there were no obstructive symptoms present. She had no signs or symptoms of hypo- or hyperthyroidism. She had no history of neck trauma. No one else in the family had any similar complaints.

Figure 1: Anterior neck mass, measuring 3 × 3 cm, which moved slightly with deglutition.
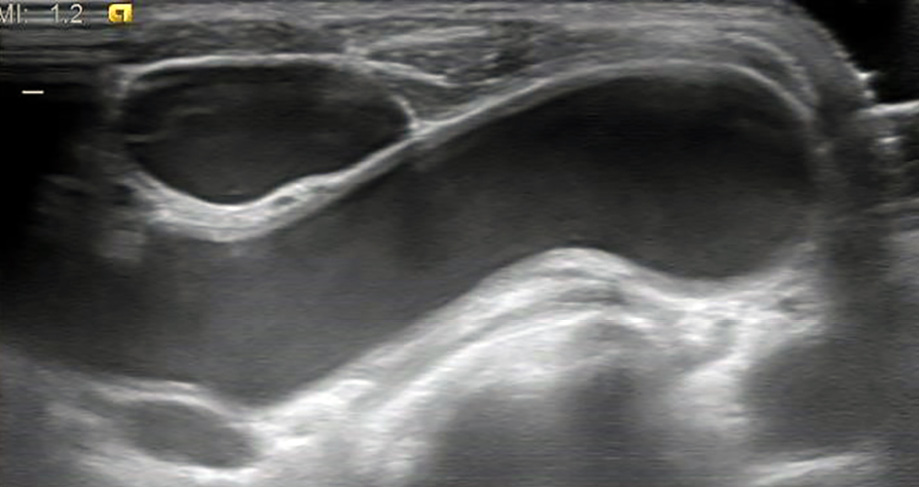
Figure 2: Neck ultrasound revealed right common carotid artery arising from the left common carotid artery.
Clinically, she appeared comfortable with no audible noisy breathing. Oral cavity examination revealed no abnormality. Neck examination revealed a non-tender, pulsatile, well-circumscribed anterior neck mass measuring 3 × 3 cm, which moved slightly with deglutition but not with tongue protrusion [Figure 1]. There were no other masses in the head, neck, or other parts of her body. No bruits were audible and all peripheral pulses were felt. Systemic examination was normal, and she had normal thyroid function test results. Laryngoscopy was performed, and no abnormality was seen.
Preliminary diagnosis of a solitary thyroid nodule was made based on her age, sex, duration of the mass and mobility of the mass with deglutition. However, we reserved any invasive investigation due to the presence of pulsation. Hence, a neck ultrasonography was performed and revealed that the bilateral thyroid lobes and isthmus had a normal size and location. However, the palpable mass was noted to be the right common carotid artery originating from the left common carotid artery at the base of the neck crossing the midline just below the thyroid isthmus [Figure 2]. Considering the patient’s age, her underlying medical illness, and that she was asymptomatic, we decided on conservative management.
Discussion
Anterior neck mass is a common presentation to the otorhinolaryngology clinic. Diagnosis of an anterior neck mass is mostly limited to solitary thyroid nodule followed by thyroglossal duct cyst. To achieve an accurate diagnosis it is important to use a combination of anatomical, pathological, and radiological approaches guided by a thorough history and physical examination.
The patient's age immediately ruled out the common anterior neck masses found in the pediatric age group such as thyroglossal duct cysts or lymphangioma (cystic hygroma). Since the swelling was in the anterior neck region, we excluded lateral neck swellings like branchial cysts, solitary lymphatic cysts, and carotid body tumors. The absence of any signs and symptoms of infection excluded cervical lymphadenitis and tubercular or non-tubercular lymphadenopathy. A solitary thyroid nodule remained a possibility in this case as the neck mass moved with deglutition.
The presence of a pulsatile anterior neck mass leads to suspicion of vascular anomalies like arteriovenous (AV) fistula, aneurysms, pseudoaneurysms, and carotid body tumors.1 A thorough history should be taken from patients presenting with a pulsatile neck mass, for example, AV fistula are commonly caused by trauma or medical procedures2,3 and pseudoaneurysms mostly appear following an arterial catheterization.4 Meticulous examination is crucial as direct surgical excision, FNA, or an open biopsy may be hazardous and cause torrential bleeding.5 However, in this patient, ultrasonography of the neck was performed and revealed a variant of the right common carotid artery from the left common carotid artery at the base of the neck crossing midline, causing a palpable mass. There was also no sign of an aneurysm or dissecting component.
Normally the right common carotid artery branches from the brachiocephalic trunk also known as an innominate artery, which originates from the aortic arch. Three branches originate from the aortic arch: the brachiocephalic trunk, the left common carotid artery, and the left subclavian artery.6 The innominate artery subsequently branches into the right common carotid artery and the right subclavian artery. The incidence of this ‘normal’ pattern is reported to be between 48% and 84% with variations reported between white and black individuals.7 Branches originating from the aortic arch may show different configurations. This ‘normal’ configuration occurs in approximately 70% of patients.8 We report an undescribed variant.
Management of pulsatile anterior neck mass secondary to vascular anomalies, particularly carotid artery variant, depends on various factors including the patients’ age and underlying medical condition, presenting complaint, possible outcomes, and complications of both the mass and surgery. For instance, in cases of atherosclerotic changes within the vessel, aneurysm, metastatic vascular tumor, pseudoaneurysm, AV fistula, and dissecting artery of the variant, surgical or endovascular intervention remains the main mode of management. Surgeons should be vigilant for cardiovascular accidents like transient ischemic attack following vascular surgery in these patients.
As for the imaging modalities, computed tomography, magnetic resonance imaging, and angiography can be ordered for further evaluation. Albeit, conventional angiography is the most accurate technique. In cases of asymptomatic and proven aberrant or variation of vessel, a conservative approach is advised considering the possible devastating surgical outcomes. As no consensus exists regarding management of this entity, treatment ought to be tailored to each patient and the benefit of surgery must be debated against the risk of possible consecutive neurological disorders and serious bleeding complications. Additionally, variations and angulations of carotid arteries are bound to produce changes in the laminar flow, causing swirls that may eventually lead to the advent of stricture or stenosis.9 Hence, this requires such patients to be on a regular follow-up to monitor any new or worsening symptoms.
Conclusion
Although an anterior neck mass is a common presentation, a thorough history and physical examination is considered to be of dire importance to determine the next step of management. The simple detection of mass pulsation may eventually lead to an accurate diagnosis and be life saving. Knowledge on variants of the origin and course of a vessel arising from the aortic arch is of paramount importance as ignorance of such a variation may lead to inadvertent surgical complications during procedures.
Disclosure
The authors declared no conflicts of interest.
Acknowledgements
We thank the patient for allowing us to share her details. We also would like to thank the radiology medical officer Dr. Hanif for providing the ultrasound image.
references
- 1. Mohamad I, Khalid M, Abdul Karim A. A pulsating mass in the pre-auricular region. Malays Fam Physician 2014;9(1):35-36.
- 2. Miekisiak G, Mis M, Sandler A, Druszcz A. Iatrogenic arteriovenous fistula of the superficial temporal artery. Oral Maxillofac Surg 2008 Dec;12(4):219-221.
- 3. Yerebakan C, Westphal B, Kröger JC, Steinhoff G. Traumatic arteriovenous fistula of the internal mammary vessels. Thorac Cardiovasc Surg 2009 Oct;57(7):422-424.
- 4. Ylönen K, Biancari F, Leo E, Rainio P, Salmela E, Lahtinen J, et al. Predictors of development of anastomotic femoral pseudoaneurysms after aortobifemoral reconstruction for abdominal aortic aneurysm. Am J Surg 2004 Jan;187(1):83-87.
- 5. Mohamad I, Nik Hassan NF. Upper lateral neck swelling: rare but important differential diagnosis. Ann Acad Med Singapore 2013 Aug;42(8):422-423.
- 6. Bergman RA, Afifi AK, Miyauchi R. Ilustrated encyclopedia of human anatomic variation. 1999:1-35.
- 7. De Garis CF, Black IH, Riemenschneider EA. Patterns of aortic arch in American white and Negro stocks, with comparative notes on certain other mammals. J Anat 1933 Jul;67(Pt 4):599-619.
- 8. Lippert H, Pabst R. Aortic arch. In: Arterial Variations in Man: Classification and Frequency. Munich, Germany: JF Bergmann-Verlag; 1985:3-10.
- 9. Ramakrishna A, Kosuri Kalyan C. Multiple bilateral anomalies of carotid arteries-a case report. NUJHS 2012;2:21-23.