|
Abstract
Solitary rectal ulcer syndrome is common in adults; however, it is thought to be rare in children. The etiology and exact pathogenesis of this condition are poorly understood. The main presenting feature of solitary rectal ulcer syndrome is rectal bleeding, but the clinical diagnosis and treatment remain challenging, particularly in pediatric patients. We present two pediatric patients with solitary rectal ulcer syndrome, who were treated surgically, and remain asymptomatic after the procedures. Clinicians should be aware of this problem in order to avoid delayed diagnosis and management.
Keywords: Solitary rectal ulcer syndrome; Rectal ulcer; Argon therapy; Trans-anal Resection; Rectal Ulcer in Children.
Introduction
Although common in adults, solitary rectal ulcer syndrome is thought to be rare in children. Its etiology is unknown, and its exact pathogenesis is poorly understood. It usually presents as bleeding from the rectum. Its clinical diagnosis and treatment remain challenging, particularly in pediatric patients. This is a report of two pediatric patients with solitary rectal ulcer syndrome. Although solitary rectal ulcer syndrome is still relatively rare, the incidence of this condition in children is increasing. Clinicians should be aware of this problem to avoid delayed diagnosis and management.
Case Report
Case No. 1
A 14-year-old boy with William’s syndrome, attention deficit hyperactivity disorder, mental retardation (IQ 60–70) and obesity presented with a 3-year history of constipation and intermittent fresh rectal bleeding with clots. The bleeding was accompanied by mucus discharge and was associated with tenesmus. This led to a mild decrease in hemoglobin level, which was treated with oral iron therapy. According to his parents; his regular meals were deficient in fibers and consisted of high proportion of soft drinks. There was no history of anal sexual activity, self-digitation, or foreign body insertion, and there was also no family history of inflammatory bowel disease.
Clinical examination showed no evidence of inflammatory bowel disease, Meckel's diverticulum, or colitis. Colonoscopy however, showed the presence of an anteriorly located solitary rectal ulcer approximately 2 cm from the anal verge. The patient was initially managed medically with laxatives and a high-fiber diet by clear instructions to the family to increase the proportion of vegetables, for example. This was followed by biofeedback, but the symptoms did not resolve.
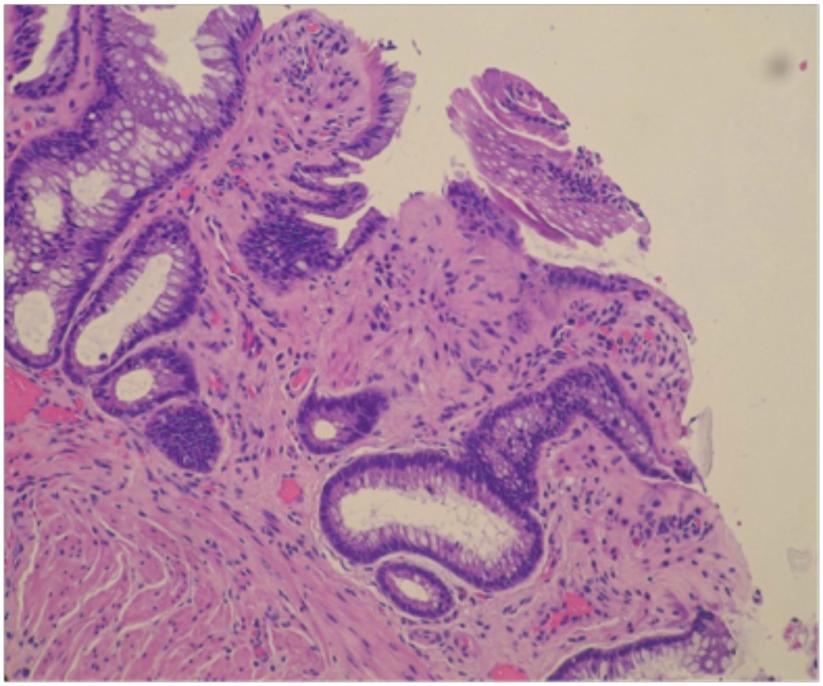
The patient subsequently underwent a single session of endoscopic excision using argon laser therapy, but the symptoms persisted, (Fig. 1). Endoscopic excision was followed by transrectal excision, suturing the ulcer base with absorbable sutures. Histopathologic examination revealed chronic active inflammatory ulcers with muscularis mucosa hyperplasia and diamond-shaped crypts, (Fig. 2). Three years after resection, the patient remains asymptomatic.
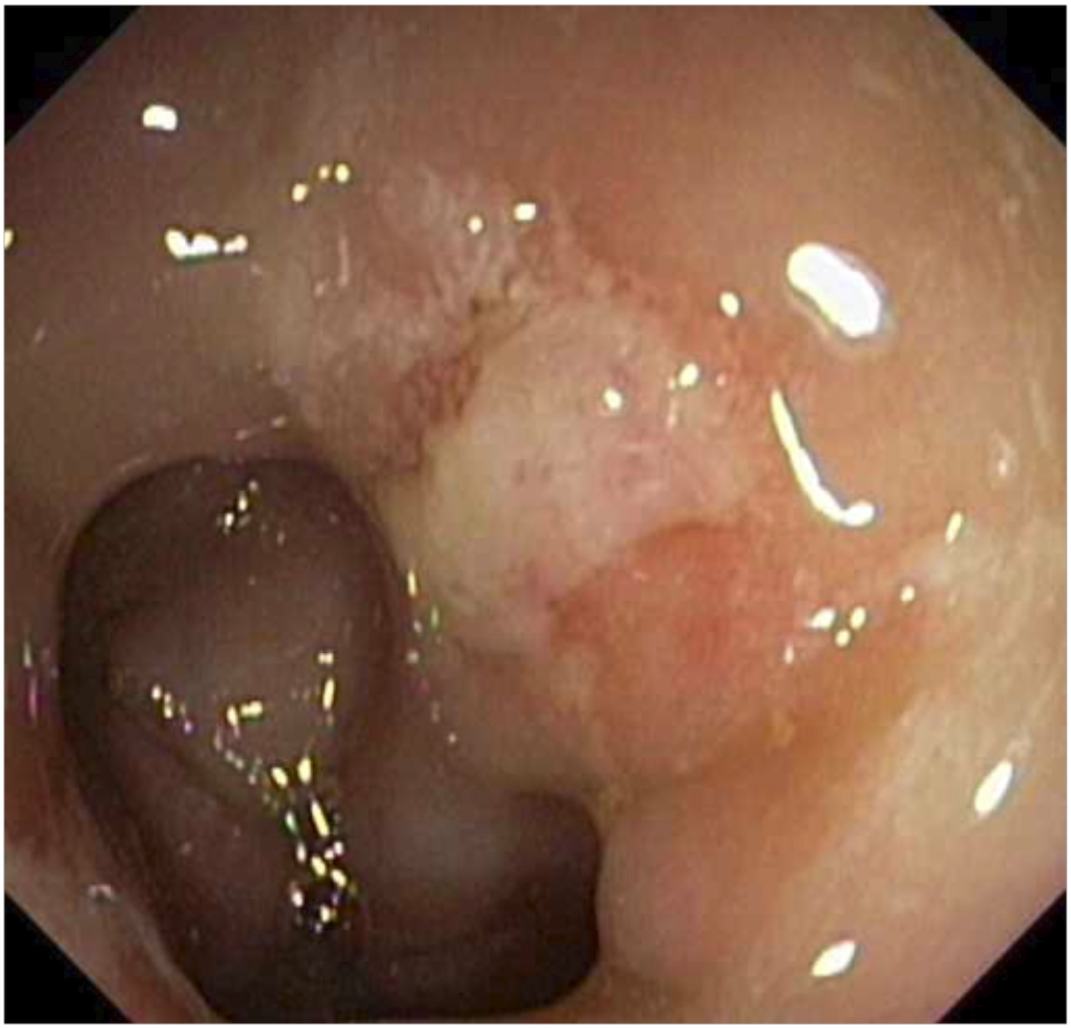
Figure 1: Photograph of the lesion showing a blanched flat rectal ulcer with hyperemic edges.
A
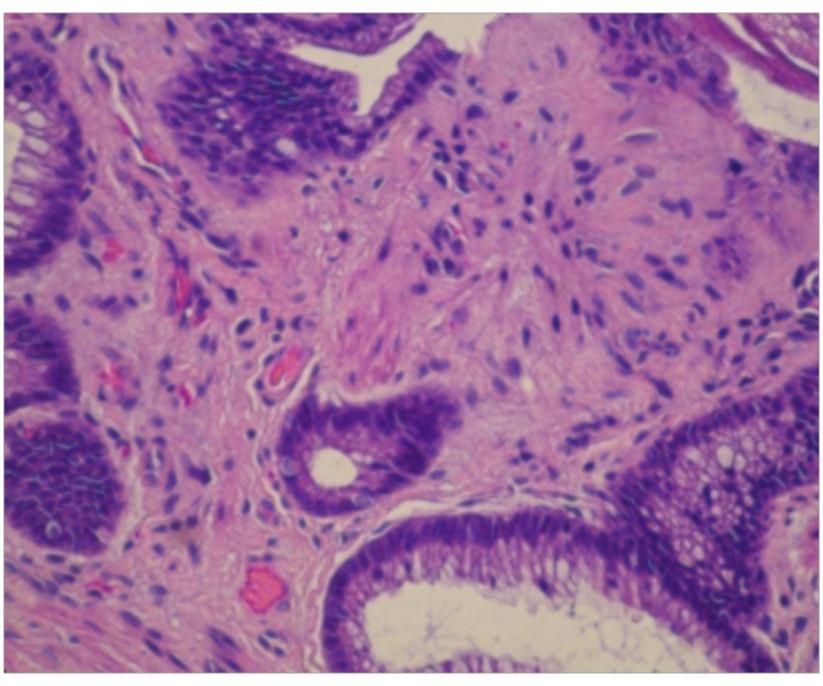
Figure 2: Histopathologic examination of the rectal lesion. (A) A solitary rectal ulcer, consisting of a polypoid large bowel mucosa with fibrotic lamina propria and migrating smooth muscle fibers. Hematoxylin and eosin staining (× 200); (B) Solitary rectal ulcer syndrome. The large bowel mucosa shows fibrosis and smooth muscle fibers in the lamina propria. Hematoxylin and eosin staining (× 400).
Case No. 2
A 12-year-old boy presented in the emergency department, for the first time, with painless bleeding from the rectum. He reported no previous history of such an attack, but he had a history of recurrent attacks of constipation, for which he had received treatment with laxatives. There was no evidence of psychological problems. On the other hand, the dietary history of the patient was unremarkable.
His general physical examination was unremarkable apart from mild pallor. Digital rectal examination revealed a polypoid lesion high in the rectum, about 8 to 10 cm from the anal verge. His hemoglobin concentration was 9 gm/dl.
The patient was provisionally diagnosed with a bleeding rectal polyp and was scheduled to undergo proctosigmoidoscopy and rectal polypectomy. At surgery, we observed a posterior ulcerated polypoid lesion, about 12 cm from the anal verge. In addition, the surrounding mucosa was ulcerated and indurated. The lesion was excised and the base was sutured. Palpation showed that the induration in the wall of the rectum extended almost to the serosal level. Histopathology showed an ulcerated polypoid lesion with histopathogical features of a solitary rectal ulcer. The patient did well post-operatively and remains free of symptoms two years after surgery.
Discussion
Solitary rectal ulcer, although fairly common in adults, is regarded as very rare condition in children.1 Although its exact etiology is unknown, it may be due to trauma, mucosal prolapse, ischemia, and/or a larger systemic process. Solitary rectal ulcer syndrome has been associated with perineal descent, nonrelaxing puborectalis syndrome, and rectal prolapse.2 Although some patients with solitary rectal ulcer syndrome are asymptomatic, most present with lower abdominal pain, tenesmus, bleeding from the rectum, mucus discharge and/or alterations of bowel habits, with many patients having difficulty defecating.
Proctosigmoidoscopy is always diagnostic. Rectal ulcers may be single or multiple. Three types of lesions have been described; ulcerative, polypoid and flat types. The most common type is ulcerative. A typical ulcer is shallow, with a white sloughy base and a thin rim of erythematous and edematous mucosa. The ulcers are usually located 4 to 12 cm from the anal verge and anterior to the anorectal junction. Although they are found most commonly on the anterior wall, they may also appear on the lateral and posterior walls.1,2 In these patients; colonoscopy and barium enema are used to exclude other types of colonic pathology. Histopathological characteristics of solitary rectal ulcer syndrome include fibrous obliteration of the lamina propria, disorientation with thickening of the muscularis mucosa, and regenerative changes with distortion of the crypt architecture. The lamina propria is replaced by smooth muscle and collagen, leading to hypertrophy and disorganization of the muscularis mucosa, referred to as fibromuscular obliteration.3
Both our patients had a history of constipation, with straining during defecation, but neither had a history of trauma or self-digitation. Repeated straining may lead to mucosal prolapse. The pathology observed in these patients may be due to pinching of the prolapsed mucosa by the unrelaxed puborectalis. Although inflammatory cloacogenic polyps have been described as a separate entity, they have the same appearance, site and histopathological features as the polypoid type of solitary rectal ulcer. We therefore regard these conditions to be identical.4
Treatment initially consists of conservative management, including an increase in dietary fiber, bowel retraining, and bulk laxatives. If conservative management fails, surgery, in the form of transrectal resection, is indicated. We recommend 2-3 years duration of conservative management before surgical interventions. Although rectopexy has been used in adult patients, it has not yet been used in children. Adults may also undergo Nd:YAG laser excision of solitary rectal ulcers, but more than one session is usually required. Although we treated our first patient with the Nd:YAG laser for one session, the patient’s family did not consent to additional sessions.5-7 Following transrectal resection, patients should continue eating a high-fiber diet and avoid constipation to avoid recurrence.
Conclusion
Our findings indicate that solitary rectal ulcer syndrome is not such a rare condition in children. Physicians should be aware of its incidence in children to avoid missing or delaying its diagnosis. Treatment is initially conservative, but, if that fails, transrectal resection followed by a high-fiber diet is usually curative.
Acknowledgements
The authors reported no conflict of interest and no funding was received for this work.
References
1. Chiang JM, Changchien CR, Chen JR. Solitary rectal ulcer syndrome: an endoscopic and histological presentation and literature review. Int J Colorectal Dis 2006 May;21(4):348-356.
2. Gabra HO, Roberts JP, Variend S, Shawis RN. Solitary rectal ulcer syndrome in children. A report of three cases. Eur J Pediatr Surg 2005 Jun;15(3):213-216.
3. Rutter KR, Riddell RH. The solitary ulcer syndrome of the rectum. Clin Gastroenterol 1975 Sep;4(3):505-530.
4. Bass J, Soucy P, Walton M, Nizalik E. Inflammatory cloacogenic polyps in children. J Pediatr Surg 1995 Apr;30(4):585-588.
5. Laser photocoagulation: Excision of solitary Rectal Ulcer. B Krisna Rav, K M Harikrishnan, Sharon Krishna. J Clin Laser Med Surg 1994;12(6):331-332.
6. Madigan MR, Morson BC. Solitary ulcer of the rectum. Gut 1969 Nov;10(11):871-881.
7. Long term clinical outcome of surgery for solitary rectal ulcer syndrome. Sitzler PJ, Kamm MA, Nicholls RJ. Mckee RG Br J Surg 1998;85:1246-1250 .
|