|
Abstract
Objectives: The aim of this paper is to describe the epidemiology of occupational injuries in the Harweel oil field, Oman.
Methods: The study is based on data gathered from a computerized database maintained by Petroleum Development of Oman (PDO). All non-fatal work-related occupational injuries registered between April 2007 and December 2009 were gathered and analyzed.
Results: A total of 170 work-related injuries were reported during the study period. Foreign body to the eye was the most common type of injury (27.6%) encountered among all injuries, followed by man falls/slips (11.8%). Injury to the upper extremities accounted for the largest percentage (38.8%) among other body parts. While, a significant portion of the injuries (52%) affected workers aged less than 30 years. The average injury rate per 1000 exposed workers per year was 19.8.
Conclusion: The study outlines the types of injuries most commonly encountered in the oil field in Oman. Additional data is required in order to devise proper epidemiological analysis. Establishing a comprehensive surveillance system for injuries is essential to ascertain factors influencing such injuries.
Keywords: Work-related injuries; Occupational injuries; Petroleum Development of Oman; Harweel; Oil field.
Introduction
Injuries pose a major public health problem and contribute to serious social and economic consequences that could be prevented by appropriate interventions.1-4 Occupational injuries constitute a major portion of the global injury burden, comprising almost 30% of all medically treated injuries to adults aged 18 to 64 years.5 The International Labor Organization (ILO) estimated that every year, about 2.2 million people die from work related injuries and work related diseases.6 Furthermore, there are around 270 million non-fatal workplace injuries occurring, where the victims miss at least three days off work. It is also estimated that 4% of the Gross Domestic Product (GDP) is lost due to workplace accidents and illnesses in the US.7 The majority of the global workforces are located in the developing countries where the rate of injuries is even 10 to 20% higher compared to developed countries.8
The oil and gas industry is one of the leading industries where a great portion of workforces are employed. The risks of injuries are higher in such industry compared to other sectors. According to the US national safety council, non-fatal work related injuries are 49% higher for the oil and gas field services industry than for all US industries combined, and these injuries are more severe.9 On the other hand, safety is considered as a high precedence objective for most companies working in this field. Nevertheless, serious injuries are still a challenge for the development of the industry. The UK offshore oil and gas industry for example, has been warned against the poor safety records as 2010 statistics showed an increase in major injuries.10
In general, the association between development and injuries has been established.11 The Sultanate of Oman has experienced a substantial infrastructural development over the last four decades. This has in turn increased the size of the workforce in the country. The national statistics for 2009 showed that the total workforce in the Sultanate was 32% in both public and private sectors and the preliminary data showed that the occupational injuries accounted for approximately 4% of the GDP. The total number of occupational injuries per 1,000 workers was 1.8 and 1.4 for 2006 and 2007, respectively.12
The Omani economy is heavily dependent on oil products, which constitutes around 75% of the country’s export earnings and 40% of its GDP.13 Petroleum Development of Oman (PDO) is the major exploration and production company in Oman accounting for more than 90% of the country's crude-oil production and almost all of its natural gas supply.14 PDO has discovered new oil reserves in Southern Oman, including a cluster of fields constituting Ghafeer, Sarmad, and Harweel. In 2005, a contract was awarded for the development of enhanced oil recovery (EOR) with gas re-injection schemes at the Harweel field, located in the far south of the sultanate; where this study is based.15
This paper attempts to describe the frequency, nature, and severity ratings, as well as the type of occupational and time trend of injuries at the Harweel oil field in Oman.
Methods
This study is based on data gathered from a computerized database maintained by PDO. Data were gathered from PDO information system, Harweel Safety department data and regional data archives from PDO Marmul Clinic. All medical reports issued by medical authorities at the Harweel oil field between 1st April 2007 and 31st December 2009 were reviewed. Data of all forms of injuries were extracted from the reports. We liaised with the safety team at the Harweel Safety Department to distinguish and thus classify the injuries into two categories; work related and non-work related.
The injured persons would initially be seen at the medical clinic, where the injury is reported. The investigating team will further analyze the injury to determine whether it is indeed work related. Work related injuries are defined as injuries taking place during the specified working hours, while the employee is engaged in work-related activities.16 Among all injuries; only the work related injuries were included and analyzed in this study.
PDO has defined guidelines to classify the severity of injuries. Minor injuries which do not affect health performance are classified as Medical Treatment Cases (MTC). While minor injuries that restrict work performance are classified as Restricted Work Cases (RWC). Furthermore, injuries necessitating the victim to take time off work are classified as Lost Time Injuries (LTI).16 However, in some cases an employee may suffer from multiple injuries at the same time; only one such case of severe injury was included in the current study. The nature of injury was coded as; burn, man fall/slip, RTA, ankle sprain/twist, nail on foot, assault, eye foreign body, bite, hammer, object fall, object hit, cut wound, crush/squeeze/trap, splinter on hand and unclassifiable.
Using SPSS version 17.0, data were analyzed by frequency in years, type of injury, severity of injury, age and body parts. Also, the frequency of monthly injuries per man hour for every trimester, yearly was calculated.
Results
A total of 426 injuries were reported during the study period from April 1st 2007 to December 31st 2009, of which 170 (40%) were recorded as work-related injuries. Table 1 presents the frequency and percentages of each type of injury. Foreign body to the eye was the most common type of injury encountered of all the reported injuries (27.6%), followed by falls/slips (11.8%). Unclassifiable injuries accounted for 7.6% of the total injuries reported, which included; injuries during drilling, scaffolding, shuttering, grinding, object movement, tire testing, etc.
The study also found that approximately 38.8% (n=66) of the injuries affected the upper extremities, while 29.4% (n=50) affected the eyes. Injuries to the lower limbs constituted 18.2% (n=31), head and neck injuries constituted 11.2% (n=19), and only 2.4% (n=4) accounted for trunk and back injuries.
The results also revealed that the majority of the injured employees (n=133, 78.2%) were Indians, and only 12 (7.1%) of the injured were Omanis. The rest of the injured employees were non-Indian expatriates. A significant segment of the reported injuries (80%, n=136) were classified as MTC. Only 11 cases (6.5%, n=11) were reported as LTI. Among the Omani employees, 25% of the reported injuries were categorized as LTIs, representing the highest percentage of LTIs compared to the other nationalities; Indian and non-Indian (5.3% and 4%, respectively).
Table 1: Types of injuries.
| Type of injury |
Frequency (%) |
| Eye FB (weld/Grind/Fabricate/Pipe Fitter) |
32 (18.8) |
| Man Fall/Slip |
20 (11.8) |
| Eye FB (Others) |
15 (8.8) |
| Burn |
14 (8.2) |
| Ankle sprain/Twist |
11 (6.5) |
| Crush/Squeeze/Trap |
11 (6.5) |
| RTA |
10 (5.9) |
| Cut wound |
10 (5.9) |
| Object hit |
8 (4.7) |
| Assault |
7 (4.1) |
| Hammer |
6 (3.5) |
| Object fall |
5 (2.9) |
| Bite |
3 (1.8) |
| Splinter on hand |
3 (1.8) |
| Nail on Foot |
2 (1.2) |
| Unclassifiable |
13 (7.6) |
| Total |
170 (100) |
FB= Foreign Body, RTA= Road Traffic Accident.
The average age of the injured workers was 30 years (SD: 7.3). The highest frequency of injury was reported among employees aged under 30 years (n= 89, 52.4%), while the lowest frequency of injury was reported among employees aged between 35-39 years (n=17, 10%). Moreover, employees aged above 39 years exhibited a relatively low frequency rate of injuries (n= 8, 12.9%).
The results also show that employees aged between 25-29 years constituted a significant segment of injuries classified as LTI (27.3%); and also accounted for a significant number of injuries recorded as MTC (35.3%); furthermore, 39.1% of the injuries categorized as RWC were also attributed to this age group. In comparison, employees aged between 35-39 years and employees over the age of 39 years generally exhibited higher LTI injuries (18.2% and 27.3%, respectively) but lower MTC injuries, (10.3% and 10.3%, respectively), while the injuries recorded as RWCs accounted for 4.3% and 21.7%, respectively for these age groups.
The total working hours in the Harweel project totalled 36.48 million hours. The average injury rate per 1000 exposed workers was 19.8 injuries per year. The frequencies of monthly injuries reported per man hour are presented in Fig. 2, which depicts two peaks in injury rates; at the beginning of the project and during the second trimester of 2008. The other trimesters represented almost equal injury rates per man hour.
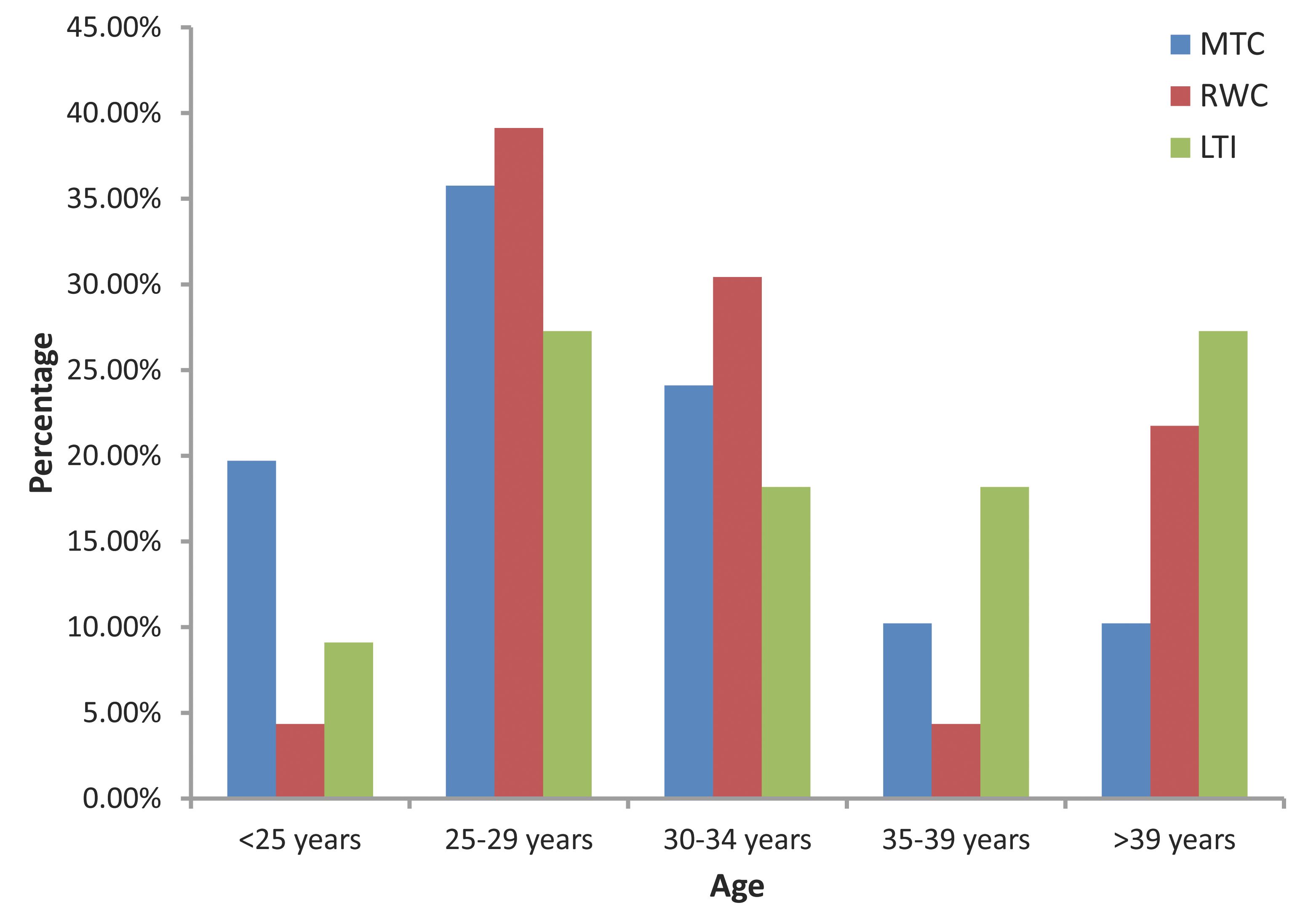
Figure 1: Age groups with injury ratings. MTC= Medical Treatment Cases, RWC= Restricted Work Cases, LTI= Lost Time Injuries.
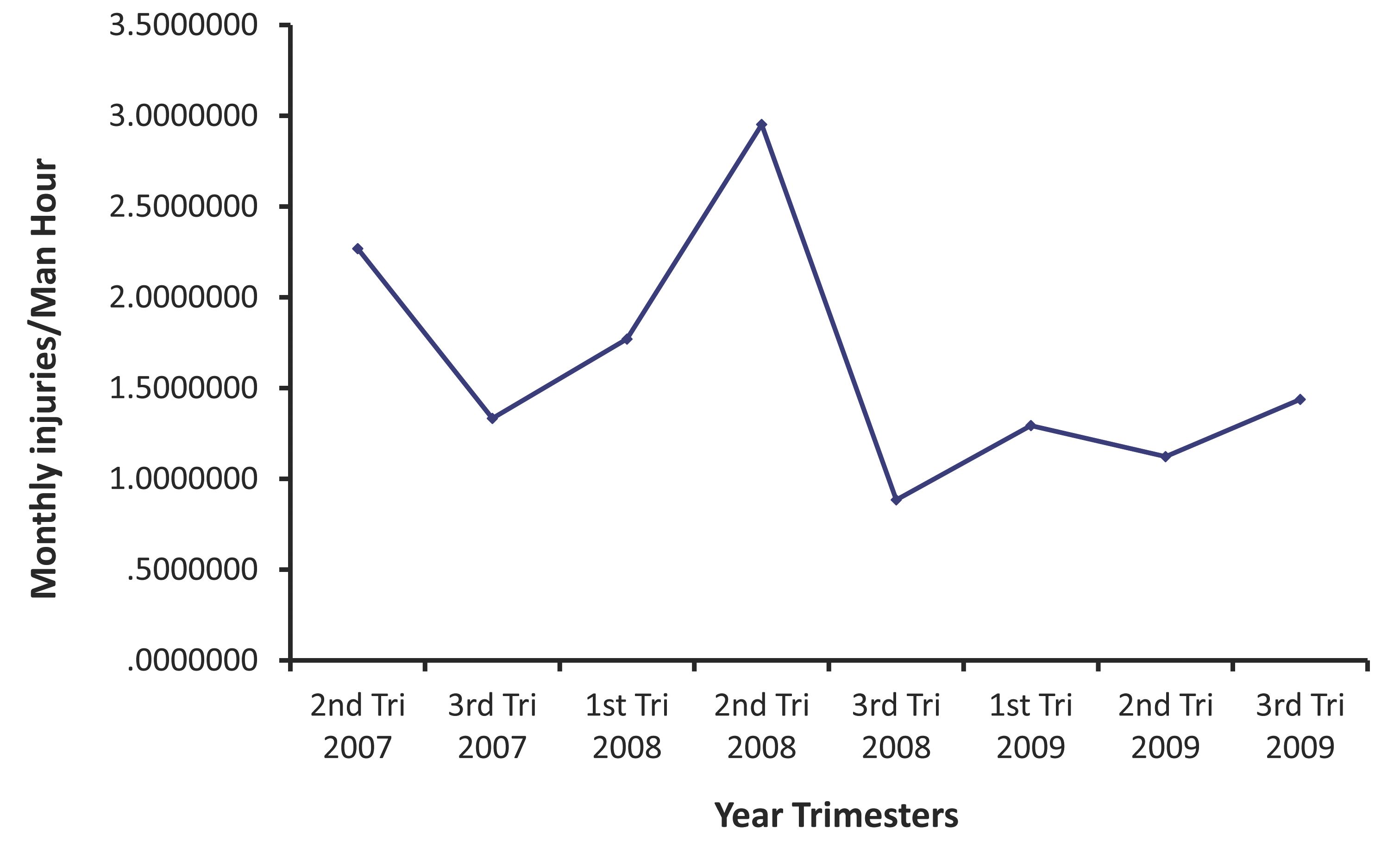
Figure 2: Monthly injuries per man hour.
Discussion
Epidemiological analysis of occupational injuries by characteristics, nature and potential causes is useful for the successful use of resources and identifying targets for prevention, but also helps to evaluate the effectiveness of intervention strategies, and consequently highlights the proper targets for prevention.17 Ongoing occupational surveillance also facilitates the review of trends over time and between geographical areas.17
Currently, there is no national system available to provide a complete picture of the occupational injury burden in the Sultanate of Oman.12 This study is the first to specifically investigate work-related injuries in the Harweel area of PDO. PDO has a computerized database for occupational injuries in different areas of the company, which not only provides data concerning the injuries, but the system also distinguishes between work-related and non-work related injuries.16
Data from a survey of a study on working adults from the United States reported an injury rate of 75 per 1000 exposed workers per year.18 Several factors can be attributed to be the main risk factors for work-related injuries; e.g. exposure to physical, mechanical and chemical hazards, as well as the conduct of unsafe practices by workers.19-21
Like other Gulf Cooperation Council countries (GCC), the majority of workforces in Oman are expatriates; mostly Indians.22 The majority of the workforce at the Harweel oil field are Indians, which may explain the highest reported frequency of injuries in this particular group. Due to the continuous movement of workers in and out from the site, it has been very difficult to estimate the actual incidence among different groups of workers within the work force.
The upper extremities were involved in the highest percentage of work-related injuries; 38.8% of all reported injuries. A similar finding has been reported by the National Occupational accidents and injuries surveillance system, which described that hands and fingers were the commonest body parts affected.12 Injuries to the eyes accounted for 29.4% of all body injuries reported. Thus, eye injuries could be prevented by wearing adequate eye protection and introducing appropriate machine guards to protect workers against obvious risks.23,24
In the Harweel project, the average injury rate per 1000 exposed workers per year was found to be 19.8. This rate is seemingly low compared to the United States national survey, which reported 75 injuries per 1000 exposed workers per year.18 In contrast, our rate is higher compared to the rate reported in the national survey of the Sultanate of Oman; 1.8 and 1.4 in 2006 and 2007 respectively.12 The problem of under-reporting of injuries is still an obstacle in Oman.12 Thus, a higher sample size and a well structured surveillance system are warranted in order to calculate a more precise figure.
The second trimester of 2007 accounted for high injury rates because it was the start of the project. While in the second trimester of 2008, the company and its contractors recruited a large number of new employees, who needed training and observation for some time, thus a high frequency rate of injuries may have occurred during this period.
Younger employees constituted a significant number of the total injuries. According to the National Occupational Accidents and Injuries Surveillance System, the majority of accidents affected workers aged between 25-34 years.12 Similar observations have also been reported by other investigators internationally.25-28
The high incidence of work-related injuries impacting young and new people could be attributed to; lack of information, lack of training, lack of supervision, lack of experience on the job and lack of knowledge and skill, amongst other reasons. Moreover, many workers begin work at an early age and often without safety training.4
The ILO estimated an increased number of young people (age range: 15-24) and older people (age range: 60 and above) entering the workforce over the next 15 years. The problem with that is that workers in these two age groups have a higher tendency of accident rates.7 Nonetheless, the safety of young workers could be ensured through better safety training, hazards analysis, and tool and workstation design, as well as engineering controls and the use of personal protective equipment.27
The burden of work-related injuries reinforces the need to examine the conditions of the work place in order to reduce the impact of work-related injuries. Prevention through safety regulations is advocated; it is also less expensive for both the workers and the society.7 There is no evidence to suggest that any country or company would have gained from an unsound level of safety and health in the long run.11 Moreover, opting for a low safety, low-health and low-income survival strategy might not lead to high competitiveness or sustainability.11
According to the ILO report, approximately 80% of occupational deaths and accidents could be prevented, if only all the countries belonging to the ILO applied the well established Accident Prevention Strategies and Behaviors.11
Conclusion
Overall, work-related injuries represent a significant burden of diseases reported in Omani oil fields. Introducing a comprehensive surveillance system would facilitate monitoring of trends of injuries overtime, and offer the potential to evaluate the prevention strategies. Prospective studies should be designed to evaluate the efficiency of the intervention strategies in the industry.
Acknowledgements
We acknowledge the helpful data and comments provided by Mr. Antoine Gilbert Marie Thiel Van. Harweel Project - HSE Manager. PDO-OSHH. http://www.pdo.co.om/hseforcontractors/. E-mail: tony.agm.vanthiel@pdo.co.om
References
1. Chau N, Mur JM, Touron C, Benamghar L, Dehaene D. Correlates of occupational injuries for various jobs in railway workers: a case-control study. J Occup Health 2004Jul;46(4):272-280.
2. Ahn Y-S, Bena JF, Bailer AJ. Comparison of unintentional fatal occupational injuries in the Republic of Korea and the United States. Inj Prev 2004 Aug;10(4):199-205.
3. Bhattachersee A. Relationships of job and some individual characteristics to occupational injuries in employed people. A community-based study. Occup Health (Lond) 2003;45:382-391 .
4. Tadesse T, Kumie A. Prevalence and factors affecting work-related injury among workers engaged in Small and Medium-Scale Industries in Gondar. Ethiop.J.Health Dev. 2007;21(1):25-34.
5. Smith GS, Wellman HM, Sorock GS, Warner M, Courtney TK, Pransky GS, et al. Injuries at work in the US adult population: contributions to the total injury burden. Am J Public Health 2005 Jul;95(7):1213-1219.
6. Somavia J. Facts on safety at work. Website: www.ilo.org/communication. Accessed August 2010.
7. Joint Press Release ILO/WHO Number of Work related Accidents and Illnesses Continues to Increase, ILO and WHO Join in Call for Prevention Strategies. Available at: www.ilo.org. Accessed August, 2010.
8. WHO/ILO. Occupational health and safety in Africa. Meeting report. World Health Organization with input of WHO/ILO Joint Effort Taskforce 2001; pp.5-6.
9. National Safety Council. Work Injury and Illness Rates 1991.
10. Offshore industry warned over not good enough safety statistics. Available at: www.hse.gov.uk. Accessed Jan 2011.
11. Takala J. Introductory Report: Decent Work – Safe Work, XVIth World Congress on Safety and Health at Work. Vienna, 27 May 2002.
12. Salim Al-Wahaibi. Issa Al-Shuaili. National strategy for occupational health and safety in the Sultanate of Oman 2009–2012. Available at: http://www.deohoman.org/nationalstrategy.html. Accessed on August, 2010.
13. Oman to Diversify Economy Designs Omanization Program. Available at:www.oilgasarticles.com. Accessed 01.Feb.2011.
14. About PD. Available at: http://www.pdo.co.om/pdoweb/tabid/54/Default.aspx. Accessed Nov/2010.
15. Oil Reserves in Oman. Available at: www.oilgasarticles.com. Accessed Feb/2011.
16. Nivedita Ram. health, safety and environment procedure:Incident Notification, Analysis, Reporting and Follow-Up. Document id: PR 1418. PDO HSE Documents. Available at www.PDO.CO.OM. Accessed on August, 2010 (Restricted access).
17. Baker EL, Melius JM, Millar JD. Surveillance of occupational illness and injury in the United States: current perspectives and future directions. J Public Health Policy 1988;9(2):198-221.
18. Dembe AE, Erickson JB, Delbos R. Predictors of work-related injuries and illness: National survey findings Occup Environ Hyg. 2004;8:542-550.
19. Chau N. etal. Relationships between some individual characteristics and occupational accidents in the construction industry. Occup Health (Lond) 2002;44:131-139 .
20. Liv XR, Zhonghu Lao, Dong Wei, Sheng Zhiye, Bing Za Zhi. Relationship Occupational injuries with social and economic factors 2004;22:86-89.
21. Wilkins R. Do long working hours lead to more workplace Injuries? Evidence from Australian industry-level panel data. Melbourne institute of applied economic and social research. The University of Melbourne 2004; pp.3-5.
22. Malecki EJ, Ewers MC. Labor migration to world cities: with a research agenda for the Arab Gulf. Prog Hum Geogr 2007;31(4):467-484 .
23. Lipscomb HJ. Effectiveness of interventions to prevent work-related eye injuries. Am J Prev Med 2000 May;18(4)(Suppl):27-32.
24. NIOSH National Occupational Research Agenda (NORA). Report on traumatic occupational injury research needs and priorities, US Department of Health and Human Services, Public Health Service, CDC, 1998.DHHS (NIOSH) publication no 98–134.
25. Noe R, Rocha J, Clavel-Arcas C, Aleman C, Gonzales ME, Mock C. Occupational injuries identified by an emergency department based injury surveillance system in Nicaragua. Inj Prev 2004 Aug;10(4):227-232.
26. Schulte PA, Stephenson CM, Okun AH, Palassis J, Biddle E. Integrating occupational safety and health information into vocational and technical education and other workforce preparation programs. Am J Public Health 2005 Mar;95(3):404-411.
27. Jackson LL. Non-fatal occupational injuries and illnesses treated in hospital emergency department in the United States. Inj Prev 2001;7:21-26 .
28. Righi E, Gatti G, Marcheselli R, Fantuzzi G, Aggazzotti G. Epidemiology of work related injuries in young people: results survey carried out in Modena (Italy) 2003; 15:735-745.
|