|
Introduction
A 38-year-old male presented with cough and dyspnea for approximately one month. He had a past medical history of hypertension, end-stage renal disease secondary to unspecified glomerulonephritis, and living-donor renal transplant 15 years ago. He had no history of exposure to tobacco or occupational toxins. His blood tests revealed increased serum creatinine (3.0 mg/dL), normal phosphate (4.0 mg/dL) and calcium levels (9.7 mg/dL), increased parathyroid hormone (95 pg/mL), and low calcidiol (10.2 ng/mL) and calcitriol (8.1 ng/mL) levels. The patient underwent bronchioalveolar lavage, which was negative for mycobacterial or fungal infection. Chest radiograph revealed fluffy densities involving the upper and mid lobes bilaterally with sparing of the subpleural region (Fig. 1). An axial computed tomographic scan of the chest showed extensive, upper lobe predominant ground glass opacities in an acinar distribution with areas of calcification. (Fig. 2, a and b)

Figure 1: Chest radiograph showing fluffy densities involving the upper lobes bilaterally with sparing of the cortex (black arrow).
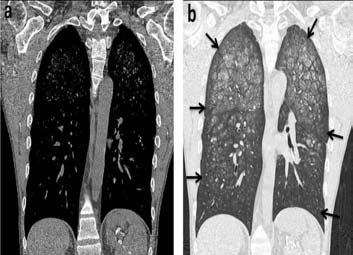
Figure 2: Coronal computed tomographic scan of chest in a) Mediastinal window b) lung window showing extensive, upper and middle lobe predominant ground glass opacities in an acinar distribution with areas of calcification with subpleural sparing (black arrows).
Questions
1. What is the diagnosis?
2. How do you treat it?
To access the full article, please complete the quiz online at www.omjournal.org
|