| |
|
|
| |
|
|
| |
Management of Pediatric Tracheo Bronchial Foreign Body Aspiration |
|
| |
|
|
| |
Sudesh Kumar,1 Rashid Al-Abri, 1 Ashok Sharma,1 Hussain Al-Kindi,2 P Mishra3 |
|
| |
doi:10.5001/omj.2010.99
|
|
| |
|
|
| |
ABSTRACT
Foreign body aspiration is a relatively commonly encountered emergency in the pediatric age group. Foreign body can get lodge at any site from supraglottis to the terminal bronchioles. The removal of nasal foreign body in the pediatric age group particularly those lodged posteriorly should always be attempted under general anesthesia as it can dislodge down into the lower airway leading to fatal complications. Foreign body aspiration can result in a spectrum of presentations, from minimal symptoms, often unobserved, to respiratory compromise, failure, and even death. Children aged 1-3 years are particularly at risk because of their increasing independence, lessening of close parental supervision as they become older, increasing activity and curiosity.
From the 1ENT Division and Cardiothoracic Division Department of Surgery; 2 Department of Pediatrics; 3Department Anesthesia, Sultan Qaboos University Hospital, Al Khoud, Muscat, Sultanate of Oman.
Received: 17 Jul 2010
Accepted: 21 Aug 2010
Address correspondence and reprint request to: Dr. Rashid Al-Abri, ENT Division and Cardiothoracic Division Department of Surgery, Sultan Qaboos University Hospital, Al Khoud, Muscat Sultanate of Oman.
Email: ralabri@hotmail.com
|
|
| |
|
|
| |
How to cite this URL:
Kumar S, Al-Abri R, Sharma A, Al-Kindi H, Mishra P. Management of Pediatric Tracheo Bronchial Foreign Body Aspiration. Oct 2010: 25(4). Available from: http://www.omjournal.org/fultext_PDF.aspx?DetailsID=47&type=fultext
|
|
| |
|
|
| |
INTRODUCTION
Foreign body (FB) aspiration remains a significant cause of morbidity and mortality especially in young children.1 Suspicion of FB aspiration in children is raised with sudden paroxysms of coughing when not directly supervised, sudden choking after eating particularly when an older sibling feeds a younger sibling, or choking and coughing when a known, small object or food particles are within reach of the child. It is estimated that 1000 children die annually in the USA because of FB aspiration.2
The right main bronchus has a predilection for foreign body impaction because it is wider than the left and the right main bronchus has more direct extension of the trachea than the left main bronchus.3 Gustav Killian in 1887 was the first person to remove a foreign body from the lower airways with a rigid bronchoscopy.4 The management of inhaled tracheal foreign body causing air way compromise requires urgent bronchoscopic removal under the general anesthesia.
This is a report of a case of a two years old female who had a foreign body in the right nasal cavity for one month duration. While examining and attempting to remove it, the child cried excessively and FB dislodged downward into lower airway, and she had respiratory arrest. Immediately, she was intubated and shifted to the operation theatre and FB was successfully removed by rigid bronchoscopy.
CASE REPORT
A two years old female was referred to our department with suspected right nasal foreign body and she had history of intermittent nasal discharge for a month’s duration. On examination, there was mucopurulent discharge in the nasal cavity and a piece of rubber was seen in the posterior part of the nasal cavity. During the examination and attempting removal, the child cried and had a sudden choking of the FB. The child become cyanosed and she had respiratory arrest. She was immediately intubated and shifted to the operation theatre. There was a lot of resistance the ventilation but both lungs were partially ventilated with positive pressure ventilation. The chest X-ray of the patient did not reveal the foreign body. Then the fibroptic bronchoscopy was introduced through the end tracheal tube and FB was localized just above the carina (Figs. 1 & 2). The rigid bronchoscope of size 4 was introduced and the FB was grasped with forceps and removed. The check bronchoscopy was done and no other FB was seen. Repeat chest X- ray was normal and the child was discharged after 48 hours and was doing well at follow up.
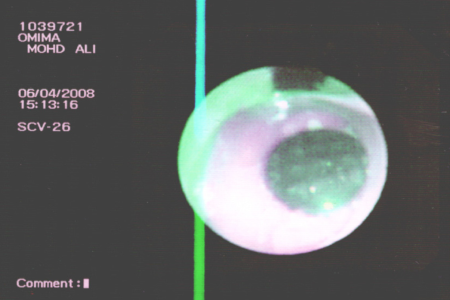
Figure 1: Bronchoscopic view of foreign body just above carina in the trachea, blocking it almost completely.
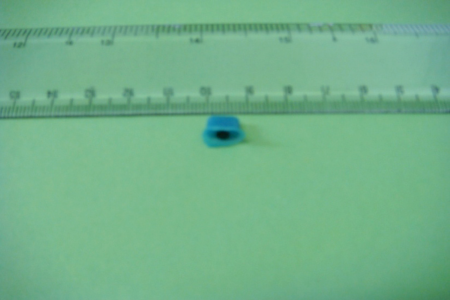
Figure 2: Foreign body photograph after Removal
DISCUSSION
The aspiration of FB by no means is an uncommon occurrence especially in the pediatric age group.5 Majority of FB aspiration occurs in children 1 to 3 years of age.6 In infants aged less than 1 year, the foreign body aspiration is the leading cause of accidental deaths. The success of removal of nasal FBs in the emergency department (ED) by emergency department physician has been reported to be 59 to 98% and various methods such as positive pressure, saline wash and mechanical extraction techniques have been used.7 However, the rest of the patients require removal by otolaryngologist in ED or in OR under general anesthesia depending on the shape, size and location of FB.
The inhaled foreign body can get lodge at any site from the laryngeal inlet to the terminal bronchioles. The location of foreign body in either of the bronchus depends upon the patients’ age and physical position at the time of inhalation. The angle made by the main bronchi with the trachea is similar until the age of 15 years resulting in equal incidence of foreign body in either bronchus. This angle between the two bronchus changes as a result of growth and development after 15 years and so the right bronchus becomes more in line with trachea and this makes a relatively straight path from the larynx to the bronchus.
There are wide ranges of clinical problems in children who are susceptible to aspirate.8 FB that pass through the larynx usually end up in one of the bronchi and seldom cause life threatening hypoxia. Rarely, as in the reported case, the object may be too large to enter the bronchus and a life threatening tracheal obstruction may accur.9 The management of inhaled foreign body depends upon the site of impact of the foreign body. Laryngeal and subglottic foreign bodies need urgent intervention in the form of tracheastomy or urgent bronchoscopy, whereas foreign bodies in the bronchus cause less airway problem.10 The inhaled foreign body can be removed by rigid or flexible bronchoscope. However, the rigid bronchoscope offers good visualization and is the preferred method for foreign body removal even in neonates and children.11,12
Both techniques of flexible bronchoscope for diagnostic purposes and the rigid bronchoscope for FB removal provide optimal care for children with FB.13 Better instrumentation and anesthesia have reduced the complication rate associated with FB removal.14
CONCLUSION
Accidental inhalation of foreign body in children into the tracheobronchial tree is not an uncommon entity. The nasal cavity FB, especially in children less than five years should be removed under general anesthesia as it can dislodge down and can lead to fatal complications. Removal of tracheo-bronchial FB requires rigid bronchoscopy and an experienced anesthetist to avoid unnecessary morbidity and mortality.
ACKNOWLEDGEMENTS
The authors reported no conflict of interest and no funding was received on this work.
|
|
| |
|
|
| |
REFERENCES |
|
| |
-
Sisenda TM, Khwa otsyula BO, Wambani JO. Management of tracheo-bronchial foreign bodies in children. East Afri Med J 2002; 799(11):580-583.
-
Black RE, Johson DG, Maatlak ME. Bronchoscopic removal of aspirated foreign bodies in children. J Pediatric Surg 1994; 34:1229-1231.
-
James B, Snow JR . Bronchology Int.Diease of the nose, throat, ear, head and neck. volume 2 , 14th Ed. 1991. p.1278-1296.
-
Killian G. Direct endoscopy of the upper air passage and esophagus , its diagnostic and therapeutic value in search for and removal of foreign bodies . J. Laryngol Rhinol Otol 1902; 17:461.
-
Gupta AK, Parida PK, Bansal S, Kumar S . Tracheal foreign body: an unusual history and presentation. Internet Journal of Pediatric and Neonatology 2006; 6:1.
-
Glynn F, Amin M, Kinsella J. nasal foreign body in children: should they have a plain radiograph in the accident and emergency? Pediatr emerg care 2008; 24:217-220.
-
Mutogama EK,Davis PJ. Anesthesia for ear, nose and throat surgery. In: Smith, Anesthesia for infants and children, 6th Ed.1996 p.669-674.
-
Tucker GF. Foreign bodies in the air passages and esophagus. In: raffenspenger JG, ed. Swan, Pediatric Surgery. 2nd New york. Appleton & Lange 1990. p.763-767.
-
Johnson DG .Malformation and obstructions of the airway. In: Ashcraft KW, Holder TM, eds. Pediatric Surgery. 2ND ED. Philadelphia: W.B.Saunders Company 1993. p.170.
-
Dunn GR, Wardrop P, Lo S, Cowan DL. Managment of suspected foreign body aspiration in children. Clin Otolatyngol Aliied Sci 2002; 27:384-386.
-
Godfrey S. Is there a place for rigid bronchoscopy in the management of pediatric lung diseases. Peadiataric Pulmon 1987; 3:179-184.
-
Wong KS, Lai SH, Lien R, Hsia SH. Retrieval of bronchial foreign body with central lumen using a flexible bronchoscope. Int J Pediatirc Otolrhinolaryngol 2002; 62:253-256.
-
Wood RE. Pitfalls in the use of flexible bronchoscope in pediatric patients. Chest 1990; 97:199-203.
-
Inglis AE, Wagner DV. Lower complication rate associated with bronchial foreign bodies over last 20 years. Ann Otol Rhino Laryngol 1992; 101:61-66.
|
|
| |
|
|
| |
|
|