Sodium is the primary cation in the extracellular fluid and is vital for maintaining intravascular volume. Two biological mechanisms can alter sodium balance and hydromineral homeostasis.1 The first is influenced by sodium chloride intake, which can lead to cell dehydration, inhibited sodium appetite, increased natriuresis, enhanced water intake, and reduced fluid excretion. The second mechanism involves hypovolemia, triggering compensatory reactions such as increased thirst and sodium appetite, especially for isotonic drinks, and antidiuretic and antinatriuretic responses. Hypervolemia reduces water and sodium intake while increasing diuresis and natriuresis.2 Dysfunctions in these systems can lead to a medical condition known as dysnatremia, including either hyponatremia (low sodium) or hypernatremia (high sodium).3,4
Hypernatremia is primarily caused by a water deficit relative to solute. The key reason is a disproportionate loss of total body water compared to solute loss. It is often associated with hypovolemia, in which water loss exceeds sodium loss.3,4 Hypernatremia is defined as a serum sodium concentration > 145 mmol/L.5 Alternative thresholds for determining the severity of hypernatremia have been suggested, including serum sodium concentrations > 150 mmol/L or > 156 mmol/L.6
Hypernatremia is rare in previously healthy individuals but common among hospitalized patients. Its prevalence varies widely depending on clinical settings, ranging from 1%–5% in general populations and between 9%–37% in intensive care units (ICUs).7–12 Risk factors include excessive fluid loss, excessive sodium intake, conditions that disrupt thermoregulation, diabetes insipidus, and renal tubular damage.13–15 There is an increased risk of hypernatremia in elderly patients with renal tubular damage associated with multiple myeloma,15 the second most frequent hematological malignancy.16 In acute myeloid leukemia, caused by the clonal expansion of myeloblasts in the peripheral blood, bone marrow, or other tissues,17 hypernatremia can be due to arginine vasopressin deficiency.18 Clinical manifestations range are moderate and nonspecific, such as headaches, nausea, and lethargy, to severe neurological signs such as seizures and coma.9
Electrolyte imbalances, including dysnatremia, are frequently observed in emergency departments and often result in hospitalization. Several studies conducted in emergency departments have examined risk factors for hypernatremia, including season, age, and climate. Hot climates such as the Gulf increases the risk of dehydration-related hypernatremia, particularly the elderly, due to excessive perspiration and insufficient fluid intake.5,14,19
It is important to note that the detection of hypernatremia is critical as it can result in prolonged hospital stays, increased morbidity and mortality rates, as well as higher healthcare costs.14 Moreover, dysnatremia has been identified as a predictor of mortality and morbidity in critically ill patients,9,13,20 particularly in patients with acute kidney injury.10,21 A large retrospective study showed that patients with severe hypernatremia (sodium concentration > 160 mmol/L) had almost a 50% in-hospital mortality rate.22 Other research has indicated an even higher in-hospital mortality rate of up to 75%.11 Hypernatremia can be life-threatening, and rapid correction of severe hypernatremia can lead to neurological consequences; however, this approach is debatable, and optimal rates of correction must be decided based on the individualized patient approach.9
Most existing studies have focused on the ICU setting,23 and there is a scarcity of data assessing hypernatremia among hospitalized patients. Additionally, there is a lack of knowledge regarding the factors that necessitate hospitalization due to hypernatremia. The aim of this study was to examine the prevalence and health impacts of hypernatremia in patients hospitalized for medical illnesses in a tertiary hospital setting and to evaluate health outcomes associated with hypernatremia.
Methods
This retrospective cohort study was conducted at Sultan Qaboos University Hospital from 29 December 2020 to 12 September 2021. Adult patients (aged ≥ 18 years) admitted to the General Internal Medicine Unit over the study period were included. Serum sodium levels were measured at the time of admission and at the point of discharge. Patients < 18 years, those with a serum sodium concentration < 136 upon admission, those directly admitted to the high dependency unit or ICU, and adult patients admitted under subspecialties outside of the General Internal Medicine Unit were excluded from the study.
Demographic data, such as age and sex, alongside medical history details, including conditions like hypertension, diabetes mellitus (DM), chronic kidney disease (CKD), heart failure, ischemic heart disease, and chronic liver disease, were collected from the patient’s electronic health records. Biochemical data, including electrolyte concentrations of calcium, potassium, phosphate, magnesium, and albumin, were collected. The patient's initial volume status was recorded at presentation, along with the management details for hypernatremia. The primary diagnosis was classified using the International Statistical Classification of Diseases and Related Health Problems, 10th Revision.
The normal range for serum sodium is 136–145 mmol/L. Hypernatremia is defined by a sodium concentration > 145 mmol/L and is classified into mild (146–150 mmol/L), moderate (151–160 mmol/L), and severe (≥ 161 mmol/L) categories.5,6 To evaluate hospitalization outcomes, the prevalence of hypernatremia was determined by analyzing the sodium concentration recorded upon admission.
The study received approval from the Medical and Research Ethics Committee at the College of Medicine and Health Sciences, Sultan Qaboos University (SQU), Muscat, Oman (MREC #2866; SQU-EC/ 087/2022; dated 28 August 2022). This study was conducted in accordance with the ethical standards and principles outlined in the Declaration of Helsinki.
Given the retrospective nature of this study, the requirement for consent was waived by the Medical and Research Ethics Committee.
The sample size was calculated based on the primary outcome: prevalence of hypernatremia. The literature indicates that the prevalence of hypernatremia is expected to range from 1–9%.9 Therefore, we determined that a sample size of 126 patients was necessary to identify the prevalence of hypernatremia in our setting by attaining a 95% confidence level and 80% statistical power. To study the association between hypernatremia and clinical outcomes, the cohort was increased using a non-probability convenience technique, which relied on the availability of patients during the study period. The research inclusion criteria were used to screen all patients admitted to the designated wards, which included 424 patients.
Analysis was conducted using sodium concentration measured upon admission. Relevant variables were compared between different concentrations of sodium and the normal sodium groups. Categorical variables were presented using frequencies and percentages. The median and IQRs were used to define variables following a continuous abnormal distribution, and the Kruskal-Wallis test was employed for univariate analysis. The chi-square test examined associations between categorical variables across the sodium groups, while Fisher’s exact test was used when expected cells frequencies were less than five. The Wilcoxon rank-sum test was performed to determine the impact on sodium concentration after hypernatremia treatment (comparing admission to discharge). Only variables with a significance level p < 0.05 were considered in the binary logistic regression analysis to identify potential independent characteristics associated with hypernatremia compared to normal sodium concentration and inpatient mortality. The study employed Kaplan-Meier survival estimates and log-rank tests to assess the time to various clinical outcomes in patients with different concentrations of hypernatremia. The significance level for a two-tailed test was set at p < 0.05. Statistical analysis was conducted using STATA (StataCorp. Stata Statistical Software: Release 17. College Station (TX): StataCorp LLC; 2021.).
Results
A total of 898 patients underwent screening during admission. Out of the total, 346 patients were excluded from the study because their sodium concentration at admission was < 136 mmol/L, and 128 patients were excluded because they had only one sodium reading throughout their admission. Only 424 patients who met the inclusion criteria were included in the analysis. On the day of admission, 34 patients (8.02%; 95% CI: 5.78–11.02%) had hypernatremia. Out of the patients included in the study, 4.7% (20) had mild, 2.3% (10) had moderate, and 0.9% (4) had severe hypernatremia.
Table 1 presents the clinical and biochemical characteristics of the groups, classified according to the severity of hypernatremia (mild, moderate, and severe) and normal sodium concentrations. There were 189 (44.6%) women, and the median age was 59.0 (IQR = 40.5–73.0) years. Aging was associated with severe hypernatremia compared to the other groups with different sodium concentrations (p < 0.010). Approximately half of the patients had a history of hypertension (47.2%), whereas none of the identified comorbidities were associated with differences in sodium concentrations among the groups. Additionally, patients with severe hypernatremia had lower concentrations of potassium and albumin compared to the other groups (p < 0.010). We further investigated the evolution of patients’ volume status upon admission. Out of the 34 patients diagnosed with hypernatremia, 21 (61.8%) were found to be hypovolemic. However, 30 patients received normal saline during their hospital stay, leading to a significant improvement in sodium concentration at discharge compared to admission (141.0 (IQR = 138.0–144.0) mmol/L vs. 149.5 (IQR = 147.0–154.0) mmol/L; p < 0.010).
Table 1: Clinical and biochemical characteristics and medications profile of admitted patients stratified according to hypernatremia severity and normal sodium on the day of admission (n = 424).
|
Female
|
189 (44.6)
|
175 (44.9)
|
5 (25.0)
|
7 (70.0)
|
2 (50.0)
|
0.110
|
|
Age, IQR, years
|
59.0 (40.5–73.0)
|
58.0 (40.0–71.0)
|
65.5 (49.5–76.0)
|
74.5 (68.0–83.0)
|
78.0 (72.5–82.0)
|
<0.010
|
|
Comorbidities
|
|
Hypertension
|
200 (47.2)
|
186 (47.7)
|
7 (35.0)
|
5 (50.0)
|
2 (50.0)
|
0.739
|
|
Ischemic heart disease
|
69 (16.3)
|
64 (16.4)
|
2 (10.0)
|
2 (20.0)
|
1 (25.0)
|
0.691
|
|
Heart failure
|
50 (11.8)
|
49 (12.6)
|
1 (5.0)
|
0 (0.0)
|
0 (0.0)
|
0.672
|
|
Diabetes mellitus
|
148 (34.9)
|
136 (34.9)
|
8 (40.0)
|
3 (30.0)
|
1 (25.0)
|
0.947
|
|
Chronic liver disease
|
21 (5.0)
|
18 (4.6)
|
2 (10.0)
|
1 (10.0)
|
0 (0.0)
|
0.356
|
|
Chronic kidney disease
|
65 (15.3)
|
62 (15.9)
|
0 (0.0)
|
3 (30.0)
|
0 (0.0)
|
0.079
|
|
Biochemical profile
|
|
Calcium, IQR, mmol/L
|
2.24 (2.16 – 2.31)
|
2.24 (2.16–2.31)
|
2.22 (2.07–2.30)
|
2.29 (2.24–2.39)
|
2.34 (2.27–2.38)
|
0.153
|
|
Potassium, IQR, mmol/L
|
3.80 (3.40 – 4.10)
|
3.80 (3.50–4.10)
|
3.40 (3.20–4.10)
|
3.10 (2.70–3.50)
|
2.90 (2.80–3.45)
|
< 0.010
|
|
Magnesium, IQR, mmol/L
|
0.80 (0.75–0.85)
|
0.80 (0.75–0.84)
|
0.80 (0.69–0.94)
|
0.79 (0.66–0.80)
|
0.82 (0.76–1.03)
|
0.557
|
|
Phosphate, IQR, mmol/L
|
0.99 (0.81–1.17)
|
0.99 (0.83–1.17)
|
0.98 (0.72–1.07)
|
0.99 (0.76–1.21)
|
0.77 (0.62–1.16)
|
0.597
|
|
Albumin, IQR, mmol/L
|
33.16 (27.00–40.00)
|
34 (28.00 – 40.00)
|
29.50 (24.00–34.10)
|
27.50 (20.00–33.00)
|
22 .00 (18.00–26.50)
|
< 0.010
|
|
Volume status assessment
|
|
Hypovolemic
|
93 (21.9)
|
72 (18.5)
|
12 (60.0)
|
5 (50.0)
|
4 (100)
|
< 0.010
|
|
Euvolemic
|
51 (12.0)
|
50 (12.8)
|
0 (0.0)
|
1 (10.0)
|
0 (0.0)
|
0.320
|
|
Overloaded
|
37 (8.7)
|
36 (9.2)
|
1 (5.0)
|
0 (0.0)
|
0 (0.0)
|
0.917
|
|
Not assessed
|
243 (57.3)
|
232 (59.5)
|
7 (35.0)
|
4 (40.0)
|
0 (0.0)
|
< 0.010
|
|
Treatment
|
|
|
|
|
|
|
Table 2 represents the clinical outcomes associated with different concentrations of hypernatremia. Patients with mild to moderate hypernatremia experienced substantially higher incidences of inpatient mortality compared to patients with normal sodium concentrations (13.1% and 35.0% vs. 30%; p = 0.024). All other measured clinical outcomes were not associated with differences in sodium concentrations. We included relevant parameters in the backward stepwise regression analysis to identify independent predictors for hypernatremia.
Table 2: Clinical outcomes of admitted patients stratified according to severity of hyponatremia (mild, moderate, and severe) and normal sodium (n = 424).
|
LOS, IQR, years
|
20.17 (7.53–45.91)
|
22.51 (7.30–55.39)
|
20.53 (11.97–37.71)
|
12.76 (6.60–18.19)
|
6.66 (4.23–9.09)
|
0.369
|
|
Admission to HDU/ICU
|
158 (37.3)
|
147 (37.7)
|
8 (40.0)
|
3 (30.0)
|
0 (0.0)
|
0.555
|
|
CPR
|
49 (12.6)
|
43 (11.0)
|
4 (20.0)
|
2 (20.0)
|
0 (0.0)
|
0.318
|
|
Inpatient mortality
|
61 (14.4)
|
51 (13.1)
|
7 (35.0)
|
3 (30.0)
|
0 (0.0)
|
0.024
|
|
90-day readmission
|
88 (20.8)
|
79 (20.3)
|
4 (20.0)
|
3 (30.0)
|
0 (0.0)
|
0.357
|
LOS: length of stay; HDU: high dependency unit; ICU: intensive care unit; CPR: cardiopulmonary resuscitation.
Serum albumin concentration had a negative association with the likelihood of hypernatremia (adjusted odds ratio (aOR) = 0.92, 95% CI: 0.88–0.96; p < 0.010). Hypovolemia, however, was associated with a positive likelihood of hypernatremia (aOR = 7.68, 95% CI: 3.57–16.49; p < 0.010) [Table 3]. Additionally, Table 4 shows that albumin had a negative association with the likelihood of inpatient mortality (aOR = 0.82, 95% CI: 0.79–0.87;p < 0.010).
Table 3: Backward stepwise binary logistic regression model for independent factors associated with hypernatremia versus normal sodium (n = 424).
|
Hypernatremia group
|
Albumin; IQR, mmol/L
|
0.92 (0.88–0.96)
|
< 0.010
|
* Stepwise backward binary logistic regression model for an adjusted odds ratio for the following factors significantly (p < 0.05) associated with hypernatremia in the univariate analysis that includes age, potassium, albumin, hypovolemia volume status, and not assessed volume status.
Table 4: Binary logistic regression model to identify if hypernatremia is independent factor for inpatient mortality (n = 424).
|
Inpatient mortality
|
Hypernatremia group
|
1.01 (0.58–4.15)
|
0.377
|
|
Age; IQR, years
|
1.01 (0.99–1.02)
|
0.287
|
|
Potassium; IQR, mmol/L
|
1.07 (0.76–1.49)
|
0.680
|
|
Albumin; IQR, mmol/L
|
0.82 (0.79–0.87)
|
< 0.010
|
|
Volume status: Hypovolemic
|
0.82 (0.79–0.87)
|
0.587
|
*Binary logistic regression model for an adjusted odds ratio for the following factors significantly (p < 0.05) associated with hypernatremia in the univariate analysis that includes age, potassium, albumin, hypovolemia volume statu,s and not assessed volume status.
Figure 1 presents a comparative analysis of the duration until readmission within 90 days among different sodium concentration groups. Patients with severe hypernatremia were readmitted earlier within this time frame compared to other groups; however, this pattern did not meet the threshold for statistical significance (hazard ratio = 1.41, 95% CI: 0.97–2.04; p = 0.06). Similarly, Figure 2 demonstrates the analysis of time to death within one year. Patients with moderate hypernatremia displayed an earlier incidence of death within one year, though, it was statistically insignificant (hazard ratio = 1.49, 95% CI: 0.96–2.31; p = 0.071).
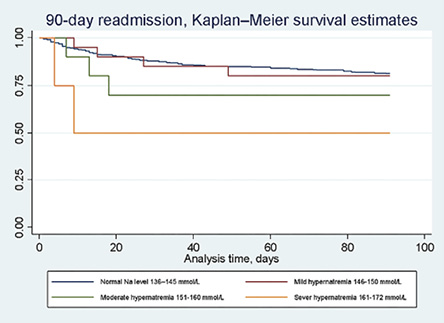 Figure 1: Analysis of time to 90-days readmission among the patients with different levels of sodium
Figure 1: Analysis of time to 90-days readmission among the patients with different levels of sodium
(n = 424).
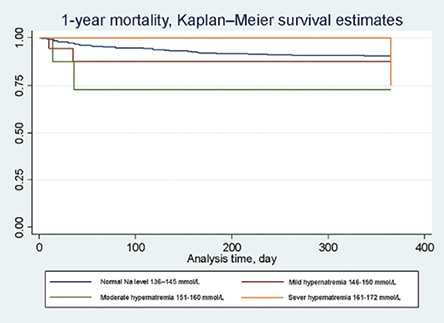 Figure 2: Analysis of time to one-year mortality among the patients with different levels of sodium
Figure 2: Analysis of time to one-year mortality among the patients with different levels of sodium
(n = 424).
Discussion
This study is one of the few to examine the prevalence and health implications of hypernatremia in patients admitted to medical wards. Hypernatremia prevalence was relatively high among the cohort, and it was associated with aging. Patients with hypernatremia presented to the hospital with hypovolemia and had lower concentrations of potassium and albumin. Although treatment resulted in improvements in sodium concentrations, patients with hypernatremia experienced a substantially higher incidence of inpatient mortality than those with normal sodium concentrations. Furthermore, a decrease in albumin concentrations demonstrated an independent association with adverse health outcomes.
Hypernatremia is a common electrolyte disorder, with a prevalence fluctuating between 1–37% among various patient groups, including those admitted to the ICU.7,8,10 In this study, the prevalence was 8.0%, which is within the range of hypernatremia prevalence in literature; however, it is on the lower side, ranging from 1–37% depending on the study population and clinical setting, this could be due to the exclusion of critically ill patients. Hypernatremia is notably common in ICUs, with studies reporting prevalence rates of 8.9–37.2%.12,24 In our study, mild hypernatremia was observed in 4.7% of patients, compared with the 1–13.1% reported in other studies. Moderate hypernatremia was observed in 2.3% of patients, compared to 8.5% in other studies. Severe hypernatremia was present in 0.9% of patients as opposed to 4–15.3% observed in various other studies, including studies from the UK.14,25 These discrepancies might be due to differences in patient types and settings in different studies. Some of those studies included patients from diverse specialties, who were in emergency rooms, outpatient settings, or even admitted to the ICU. In contrast, our study specifically focused on medical cases and included only patients admitted to medical wards.24,26 Additionally, the association between aging and hypernatremia observed in our cohort is consistent with findings from studies conducted in Japan and the USA, which have highlighted the diminished thirst mechanism and reduced renal function in elderly populations as significant contributors to hypernatremia.
Hypernatremia tends to occur more frequently in elderly, frail individuals compared to younger ones. Our study demonstrated a statistically significant association between age and hypernatremia; older patients exhibited a higher severity of hypernatremia.8,19 This can be explained by the diminished thirst sensation in the elderly and the gradual decline of renal function with age, which reduces the kidney’s efficacy in maintaining electrolyte and water homeostasis.27,28 Our study investigated sex as a potential factor associated with hypernatremia. Consistent with earlier studies, our findings revealed no significant association between sex and hypernatremia.19,29 However, a study from Japan reported a significant association between female sex and an increased risk of hypernatremia in older community-dwelling individuals, with smaller muscle mass potentially mediating this relationship.30
While the existing literature provides limited insights into the association of comorbidities with hypernatremia, our study reported that 41.2% of patients with hypernatremia had hypertension. Another study noted that around 54% of their patient population with hypernatremia were hypertensive. However, both studies found no significant association between hypernatremia and hypertension.31 No such data were available in the literature about the correlation between other chronic medical conditions and hypernatremia, as this was not studied thoroughly previously. CKD was identified in 8.8% of hypernatremia patients in this study. In contrast, another study reported CKD presence in only 1% of its hypernatremia patients.32 These discrepancies could be associated with varying stages of CKD, different treatments given, and possible dietary differences between the groups. Notably, baseline hyponatremia and time-dependent hyponatremia or hypernatremia are independently linked to an increased risk of all-cause mortality in patients with CKD.33 In addition, this study found that ischemic heart disease was present in 14.7%, heart failure was present in 2.9%, and DM was observed in 35.3% of patients with hypernatremia. In another study, only 11% of hypernatremia patients were found to have DM.34 This discrepancy in percentages may be attributed to differences in the prevalence of DM among the patients included in the studies. Interestingly, among hypernatremia patients, chronic liver disease was the least common comorbid condition, perhaps because hyponatremia is more typically associated with chronic liver disease. On the other hand, hypernatremia, though less common, is also linked to adverse outcomes in cirrhosis, often caused by hypotonic fluid losses due to osmotic diuresis or lactulose-induced diarrhea.35 Also, to emphasize that studies examining hypernatremia in the Gulf region remain limited, despite its clinical significance in hospitalized populations. The Gulf region, characterized by a predominantly hot climate, poses a higher risk of dehydration-related hypernatremia due to excessive water loss from perspiration and inadequate fluid intake, especially among vulnerable populations such as the elderly.
In this study, hypernatremia was significantly associated with hypokalemia and hypoalbuminemia. The relationship between hypernatremia and hypokalemia could be explained by plasma solute autoregulation, as both are cations and both influence cellular transmembrane potentials.36 Also, previous studies have noted a significant association between hypokalemia and hypernatremia, particularly in specific patient populations such as those with community-acquired pneumonia, cancer, and CKD. These conditions often coexist due to underlying disease processes or as side effects of treatments.37,38 Hypoalbuminemia is associated with hypernatremia, particularly in the context of critical illness, inflammation, and renal dysfunction. This mainly occurs due to the osmolar effect of sodium on plasma, which results in decreased albumin concentrations to maintain serum osmolarity.39 Sodium homeostasis is associated with water homeostasis, and changes in volume status might result in various forms of dysnatremia.
In this study, hypovolemia was found in 61.8% of patients with hypernatremia, a statistically significant finding. Hypernatremia in hypovolemic patients occurs due to water loss through different mechanisms, including urinary loss, gastrointestinal loss, or even sweating and insensible loss with febrile illnesses, resulting in elevated sodium readings.40 Overcorrection or an inability to appropriately correct hypernatremia may result in permanent neurological injuries and death.9,41 Therefore, meticulously calculated fluid replacement is imperative in these patients to avoid such preventable damage.8 In our study, normal saline infusion was used to correct hypernatremia for most of the patients with hypernatremia.
Across various clinical settings, hypernatremia is consistently associated with poor outcomes, including higher mortality rates, longer hospital stays, and increased healthcare costs. This association is evident in patients with severe traumatic brain injury, subarachnoid hemorrhage, and COVID-19, as well as in general hospitalized populations.42–44 The severity of hypernatremia further influences the extent of these adverse outcomes, with moderate to severe hypernatremia posing a greater risk.12,45,46 In this study, both mild and moderate hypernatremia were associated with increased mortality. However, this association was not observed in patients with severe hypernatremia due to the small number of patients in this group (n = 4).
This study has many strengths. Unlike previous studies, it focused on medical patients admitted to non-critical areas. It was powered to assess the prevalence of hypernatremia and to comprehensively examined various factors potentially associated with hypernatremia. Additionally, it evaluated health outcomes potentially linked to hypernatremia. However, the study’s limitations include its retrospective nature, which poses challenges. Data on nutritional status and average water intake were unavailable due to a lack of documentation, and capturing other information such as hematological parameters was not possible. Lastly, data on readmission and mortality were derived solely from Sultan Qaboos University Hospital only.
Conclusion
Hypernatremia is a significant electrolyte derangement among hospitalized patients, but less prevalent compared to critically ill medical patients. Old age and hypovolemia are common among patients with hypernatremia. Furthermore, hypokalemia and hypoalbuminemia are associated with hypernatremia, suggesting a common mechanism driving these body elemental disturbances. Hypernatremia may be associated with poor health outcomes, including increased inpatient mortality.
Disclosure
The authors declare no conflicts of interest. No funding was received for this study.
references
- 1. Bie P. Mechanisms of sodium balance: total body sodium, surrogate variables, and renal sodium excretion. Am J Physiol Regul Integr Comp Physiol 2018 Nov;315(5):R945-R962.
- 2. Bernal A, Zafra MA, Simón MJ, Mahía J. Sodium homeostasis, a balance necessary for life. Nutrients 2023 Jan;15(2):395.
- 3. Qian Qi. Hypernatremia. Clin J Am Soc Nephrol 2019;14(3):432-434.
- 4. Sonani B, Naganathan S, Al-Dhahir MA. Hypernatremia. StatPearls. Treasure Island (FL): StatPearls Publishing Copyright © 2024, StatPearls Publishing LLC; 2024.
- 5. Wootton E, Grossmann M, Warren AM. Dysnatremia in a changing climate: a global systematic review of the association between serum sodium and ambient temperature. Clin Endocrinol (Oxf) 2024 Jun;100(6):527-541.
- 6. Oehler D, Immohr MB, Böttger C, Bruno RR, Sigetti D, Haschemi J, et al. Donor hypernatremia is associated with increased mortality after heart transplantation: a retrospective study. Clin Transplant 2022 Dec;36(12):e14803.
- 7. Mapata L, Richards GA, Laher AE. Hypernatremia at a tertiary hospital intensive care unit in South Africa. Cureus 2022 Feb;14(2):e22648.
- 8. Bataille S, Baralla C, Torro D, Buffat C, Berland Y, Alazia M, et al. Undercorrection of hypernatremia is frequent and associated with mortality. BMC Nephrol 2014 Feb;15:37.
- 9. Feigin E, Feigin L, Ingbir M, Ben-Bassat OK, Shepshelovich D. Rate of correction and all-cause mortality in patients with severe hypernatremia. JAMA Netw Open 2023 Sep;6(9):e2335415.
- 10. Jansch C, Matyukhin I, Marahrens M, Lehmann R, Khader B, Ritter O, et al. Hypernatremia: epidemiology and predictive role in emerging and established acute kidney injury. J Clin Med Res 2023 Sep;15(8-9):399-405.
- 11. Yun G, Baek SH, Kim S. Evaluation and management of hypernatremia in adults: clinical perspectives. Korean J Intern Med 2023 May;38(3):290-302.
- 12. Arzhan S, Roumelioti ME, Litvinovich I, Bologa CG, Unruh ML. Outcomes of hospital-acquired hypernatremia. Clin J Am Soc Nephrol 2023 Nov;18(11):1396-1407.
- 13. Kuru BK, Baydın A, Ocak M, Aksoy İ. Diagnostic and prognostic efficacy of optic nerve sheath diameter in patients with dysnatremia. Med Ultrason 2024 Jun;26(2):147-152.
- 14. Otterness K, Singer AJ, Thode HC Jr, Peacock WF. Hyponatremia and hypernatremia in the emergency department: severity and outcomes. Clin Exp Emerg Med 2023 Jun;10(2):172-180.
- 15. Imashuku S, Kudo N, Kubo K. Severe hypernatremia and hyperchloremia in an elderly patient with IgG-kappa-type multiple myeloma. J Blood Med 2013 May;4:43-47.
- 16. Mohammed DA, Khallaf SM, El-Naggar MG, Abdel-Hameed MR, Bakry R. Interleukin-10: a potential prognostic marker in patients with newly diagnosed multiple myeloma. Resum Oncol 2021;17(1):38-41.
- 17. Sayed SA, Hassan EA, Abdel Hameed MR, Agban MN, Mohammed Saleh MF, Mohammed HH, et al. Ketorolac-fluconazole: a new combination reverting resistance in candida albicans from acute myeloid leukemia patients on induction chemotherapy: in vitro study. J Blood Med 2021 Jun;12:465-474.
- 18. Rasi V, Riekhof F, Mahmoud M, Ejiofor S, Lentine KL. A Case of hypernatremia in a newly diagnosed patient with acute myeloid leukemia: lessons for nephrologists. Cureus 2024 Apr;16(4):e59186.
- 19. Imai N, Sumi H, Shibagaki Y. Impact of age on the seasonal prevalence of hypernatremia in the emergency department: a single-center study. Int J Emerg Med 2019 Sep;12(1):29.
- 20. Ma Y, Zhang P, Hou M. Association of hypernatremia with mortality in patients with COVID-19: a systematic review and meta-analysis. Immun Inflamm Dis 2023 Dec;11(12):e1109.
- 21. Atlani M, Kumar A, Pakhare AP, Singhai A, Gadwala R. Potential association of hypernatremia with mortality in patients with acute kidney injury and COVID-19. Cureus 2022 Jul;14(7):e27530.
- 22. Ates I, Özkayar N, Toprak G, Yılmaz N, Dede F. Factors associated with mortality in patients presenting to the emergency department with severe hypernatremia. Intern Emerg Med 2016 Apr;11(3):451-459.
- 23. Lindner G, Funk GC, Schwarz C, Kneidinger N, Kaider A, Schneeweiss B, et al. Hypernatremia in the critically ill is an independent risk factor for mortality. Am J Kidney Dis 2007 Dec;50(6):952-957.
- 24. Arzhan S, Roumelioti ME, Litvinovich I, Bologa CG, Myers OB, Unruh ML. Hypernatremia in hospitalized patients: a large population-based study. Kidney360 2022 Apr;3(7):1144-1157.
- 25. Vedantam A, Robertson CS, Gopinath SP. Morbidity and mortality associated with hypernatremia in patients with severe traumatic brain injury. Neurosurg Focus 2017 Nov;43(5):E2.
- 26. Tsipotis E, Price LL, Jaber BL, Madias NE. Hospital-associated hypernatremia spectrum and clinical outcomes in an unselected cohort. Am J Med 2018 Jan;131(1):72-82.e1.
- 27. Andreucci VE, Russo D, Cianciaruso B, Andreucci M. Some sodium, potassium and water changes in the elderly and their treatment. Nephrol Dial Transplant 1996;11(Suppl 9):9-17.
- 28. Luckey AE, Parsa CJ. Fluid and electrolytes in the aged. Arch Surg 2003 Oct;138(10):1055-1060.
- 29. Barma MA, Soiza RL, Donnan PT, McGilchrist MM, Frost H, Witham MD. Serum sodium level variability as a prognosticator in older adults. Scand J Clin Lab Invest 2018;78(7-8):632-638.
- 30. Tanaka S, Fujishiro M, Imatake K, Suzuki Y, Ishihara H, Tani S. Impact of female sex on the susceptibility to hypernatremia among older community-dwelling individuals in Japan. Int J Gen Med 2022 Jan;15:777-785.
- 31. Wu D, Chen Y, Guan H, Sun Y. Association of abnormal serum electrolyte levels with hypertension in a population with high salt intake. Public Health Nutr 2019 Jun;22(9):1635-1645.
- 32. Hassanein M, Arrigain S, Schold JD, Nakhoul GN, Navaneethan SD, Mehdi A, et al; CRIC Investigators. Dysnatremias, mortality, and kidney failure in CKD: findings from the chronic renal insufficiency cohort (CRIC) study. Kidney Med 2022 Oct;4(12):100554.
- 33. Sun L, Hou Y, Xiao Q, Du Y. Association of serum sodium and risk of all-cause mortality in patients with chronic kidney disease: a meta-analysis and sysematic review. Sci Rep 2017 Nov;7(1):15949.
- 34. Snyder NA, Feigal DW, Arieff AI. Hypernatremia in elderly patients. A heterogeneous, morbid, and iatrogenic entity. Ann Intern Med 1987 Sep;107(3):309-319.
- 35. Bernardi M, Zaccherini G. Approach and management of dysnatremias in cirrhosis. Hepatol Int 2018 Nov;12(6):487-499.
- 36. Girndt M. [Electrolyte disorders]. Internist (Berl) 2011 Aug;52(8):963-974, quiz 975.
- 37. Ratanasrimetha P, Workeneh BT, Seethapathy H. Sodium and potassium dysregulation in the patient with cancer. Adv Chronic Kidney Dis 2022 Mar;29(2):171-179.e1.
- 38. Huang H, Jolly SE, Airy M, Arrigain S, Schold JD, Nally JV, et al. Associations of dysnatremias with mortality in chronic kidney disease. Nephrol Dial Transplant 2017 Jul;32(7):1204-1210.
- 39. Kahn T. Hypernatremia with edema. Arch Intern Med 1999 Jan;159(1):93-98.
- 40. Nguyen MK, Kurtz I. Correction of hypervolaemic hypernatraemia by inducing negative Na+ and K+ balance in excess of negative water balance: a new quantitative approach. Nephrol Dial Transplant 2008 Jul;23(7):2223-2227.
- 41. Adrogué HJ, Tucker BM, Madias NE. Diagnosis and management of hyponatremia: a review. JAMA 2022 Jul;328(3):280-291.
- 42. Hoffman H, Jalal MS, Chin LS. Effect of hypernatremia on outcomes after severe traumatic brain injury: a nationwide inpatient sample analysis. World Neurosurg 2018 Oct;118:e880-e886.
- 43. Kolmodin L, Sekhon MS, Henderson WR, Turgeon AF, Griesdale DE. Hypernatremia in patients with severe traumatic brain injury: a systematic review. Ann Intensive Care 2013 Nov;3(1):35.
- 44. Ruiz-Sánchez JG, Núñez-Gil IJ, Cuesta M, Rubio MA, Maroun-Eid C, Arroyo-Espliguero R, et al; HOPE COVID-19 investigators. Prognostic impact of hyponatremia and hypernatremia in COVID-19 pneumonia. A HOPE-COVID-19 (health outcome predictive evaluation for COVID-19) registry analysis. Front Endocrinol (Lausanne) 2020 Nov;11:599255.
- 45. Ni HB, Hu XX, Huang XF, Liu KQ, Yu CB, Wang XM, et al. Risk factors and outcomes in patients with hypernatremia and sepsis. Am J Med Sci 2016 Jun;351(6):601-605.
- 46. Thongprayoon C, Cheungpasitporn W, Yap JQ, Qian Q. Increased mortality risk associated with serum sodium variations and borderline hypo- and hypernatremia in hospitalized adults. Nephrol Dial Transplant 2020 Oct;35(10):1746-1752.