An encysted hydrocele of the cord (also known as spermatic hydrocele) occurs when there is an entrapment of fluid in the processus vaginalis.1 This fluid does not communicate with the tunica vaginalis or the peritoneal cavity. Although rare, the condition is more commonly seen in infants and children; however, it has also been reported in adults.2 These lesions may occur anywhere along the tract of testicular descent from its intra-abdominal embryologic origin. Though the exact causes and pathogeneses are often unknown, cases have been reported to occur after groin trauma.
Encysted hydrocele have also been described in the context of congenital abnormalities. Encysted hydrocele of the cord is a differential diagnosis in presentations of incarcerated inguinal hernia, dermoid cyst or teratoma, inguinal lymphadenopathy, lymphatic cyst, and tumors of the spermatic cord.
We describe three cases of boys aged 16, seven, and four years. Each presented with a left scrotal swelling, which was diagnosed clinically as an encysted hydrocele, confirmed by surgical exploration, and resolved successfully.
Case Reports
Case one
A mass had appeared in the left scrotum of a 16-year-old boy, eight months prior to the presentation. There was no history of precipitating factors such as trauma or local infection. The mass grew to its current size in three weeks. During that period, it was intensely painful. The pain subsided but returned occasionally with a severity of 4–6 on the pain scale. The pain was described as constant and dull, but usually self-abating. Continuous pain was managed with paracetamol. There was no associated vomiting, constipation, or abdominal swelling. The patient, who had no history of such swellings, described this one as his ‘third testicle.’
Clinical examination was unremarkable except for the left scrotal swelling. Palpation revealed a smooth-surfaced, painless, tense-to-hard ovoid mass about 8 × 6 × 6 cm in size, located nearly 3 cm below the inguinal canal exit. The spermatic cord above and below the mass had the same thickness, which was also as thick as the contralateral cord. The mass could not be felt separately from the spermatic cord. The scrotal skin appeared unaffected and was freely mobile. The mass did not transilluminate. Each testicle was about 4 × 3 × 3 cm, non-tender, and smooth-surfaced, with no palpable surface irregularity [Figure 1].
 Figure 1: Left scrotal swelling in a 16-year-old boy.
Figure 1: Left scrotal swelling in a 16-year-old boy.
A clinical diagnosis of encysted hydrocele of the cord was made with possible differential diagnosis of a teratoma or a lymph node. Ultrasonography may have helped exclude a teratoma and confirm the diagnosis; however, the facility was unavailable at our primary care center, and we did not contemplate it further.
A decision was made to surgically explore the lesion. Under local anesthesia, a transverse scrotal incision was made and gently dissected to reveal an ovoid cystic mass attached to one side of the cord [Figure 2].
 Figure 2: Intraoperative view of the left testis and the encysted hydrocele above it.
Figure 2: Intraoperative view of the left testis and the encysted hydrocele above it.
The encysted hydrocele was then dissected off the cord. Incision through the cystic mass released a brownish fluid from a multiloculated structure with fibrous strands [Figure 3].
 Figure 3: (a) The excised hydrocele of the cord. (b) Vertical section of the hydrocele, showing its multilocular structure and fibrous strands.
Figure 3: (a) The excised hydrocele of the cord. (b) Vertical section of the hydrocele, showing its multilocular structure and fibrous strands.
Case two
A seven-year-old boy presented with a left scrotal mass that had been noticed at birth. The parents described the swelling as distinct from the left testicle and that it did not extend into the abdomen. This mass was painless and did not increase in size while crying or coughing. When the patient was six months old, he was seen at a health facility where a yellowish fluid was aspirated. The swelling initially disappeared, only to slowly recur weeks later. Since then, the parents reported that the mass had not increased in size.
On examination, a soft, fluctuant, non-tender, non-reducible mass was noted in the left scrotum about 1 cm below the left external inguinal ring. The spermatic cord was palpable above the mass. The mass was transilluminated, and there were no palpable inguinal lymph nodes bilaterally. The scrotal skin appeared normal. A diagnosis of an encysted hydrocele of the cord was made clinically.
After local anesthesia and a para-scrotal incision to explore the mass, a cystic mass measuring 2 × 4 cm was revealed [Figure 4]. This was gently dissected off the spermatic cord. The excised hydrocele was composed of yellowish fluid enclosed in a thin sac. The postoperative course was uneventful, and the patient was discharged home the same day. The wound healed normally, and there was no recurrence.
 Figure 4: Intraoperative view of the left testis and the encysted hydrocele in a seven-year-old boy.
Figure 4: Intraoperative view of the left testis and the encysted hydrocele in a seven-year-old boy.
Case three
A four-year-old boy presented with a scrotal swelling that was noticed by his parents at birth, but had not subsequently increased in size. His prenatal history was unremarkable.
On examination, a non-tender, soft, fluctuant mass about 7 × 2 cm was palpable in the child’s left scrotum. The mass was non-reducible and translucent to light. The left testis could be palpated independently of the mass. The testes were about 1 × 1 cm in size, with no abnormalities. A diagnosis of encysted hydrocele of the cord was considered. All other physical examination findings were unremarkable.
Surgical exploration was performed. A fluid-filled hydrocele of about 8 × 2 × 2 cm was gently dissected off the spermatic cord [Figure 5].
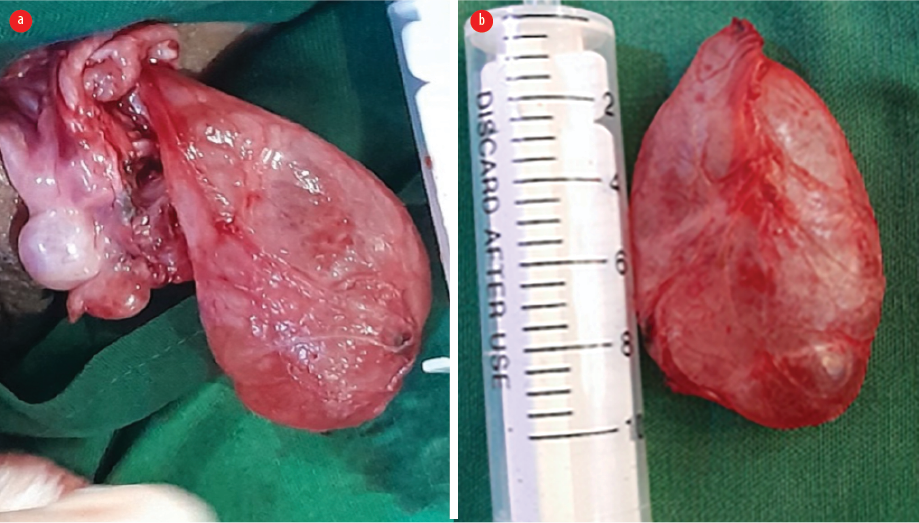 Figure 5: (a) Intraoperative view of the encysted hydrocele alongside the left testicle in a four-year-old. (b) The excised hydrocele.
Figure 5: (a) Intraoperative view of the encysted hydrocele alongside the left testicle in a four-year-old. (b) The excised hydrocele.
Permission and informed consent were obtained from the parents of all three patients.
Discussion
We have described the cases of three boys who presented to a primary clinic in Ghana. Each case was clinically diagnosed with encysted hydroceles, surgically explored, and successfully treated. An encysted hydrocele should be differentiated from the more prevalent vaginal hydrocele or the extremely rare abdominoscrotal hydrocele.3 An encysted hydrocele may be congenital or acquired following trauma or infection.2,4 In most cases, a direct cause is not found. Cases are even rarer in females, where encystment occurs in the canal of Nuck.5 In English medical literature, we found a few reported cases in adult males with encysted hydrocele, but only one adolescent, a 19-year-old Nigerian.2,6
Encysted hydrocele can pose a diagnostic challenge to clinicians in primary health centers without imaging facilities, who have to base the diagnosis solely on patient history and clinical examination. Cases are often asymptomatic (as in our cases 2 and 3) and serendipitously discovered.7 A symptomatic hydrocele in the inguinal canal presenting with acute groin swelling and sudden onset of pain might be confused with an incarcerated inguinal hernia.6,8
When a swelling is found lower down the tract of testicular descent with a palpable mass similar to a testicle, as in our three cases, it should prompt a high index of suspicion for an encysted hydrocele. The encysted fluid has been reported to undergo torsion, resulting in severe pain in some instances.9 Though a ‘third testicle’ description helps to delineate it from a hernia, it may not differentiate it from polyorchidism, dermoid cysts or teratomas, or testicular cancer.10
Imaging modalities that aid in the diagnosis of encysted hydroceles include ultrasound, computed tomography, and magnetic resonance imaging.7 Ultrasound will typically describe a cystic anechoic mass,6 which may confirm the diagnosis before surgery. Imaging could not be considered because of the unavailability of even basic sonography equipment at our primary care facility. The surgical exploration method we adopted is supported by positive reports from elsewhere.8–10 Complete resection of the hydrocele is usually recommended. Aspiration is not recommended as it often leads to regrowth, as observed in the history of case 2. In longstanding cases or in instances of superimposed infections or hemorrhage within the cyst, the healing process can result in fibrosis of the cyst wall. This may explain the multiloculated thick-walled cyst found in case 1. A few case reports have described thin-walled sacs similar to those found in cases 2 and 3. Although mesothelioma was a possible diagnosis, follow-up of our patients did not reveal any such indications. We recommend a histopathology of the sample in settings where it is possible. We were unable to conduct a histopathology due to patient financial constraints and the long distance (300 km) to the nearest tertiary center with histopathology facilities.
Conclusion
Primary care physicians in peripheral facilities should consider clinical encysted hydroceles as a possible diagnosis of scrotal swellings in children who present with scrotal masses as they may not be as rare as often assumed. Management by surgical excision is recommended as being both diagnostic and curative.
Disclosure
The authors declare no conflicts of interest.
references
- 1. Chang Y-T, Lee J-Y, Wang J-Y, Chiou CS, Chang CC. Hydrocele of the spermatic cord in infants and children: its particular characteristics. Urology 2010 Jul;76(1):82-86.
- 2. Esen B, Sarıdemir S, Guleryuz Bolsu G, Doğanözü AC. Encysted spermatic cord hydrocele in adults: a case report and review of the literature. Acta Oncol Turc 2020;53(3):543-546.
- 3. Abantanga FA. Groin and scrotal swellings in children aged 5 years and below: a review of 535 cases. Pediatr Surg Int 2003 Aug;19(6):446-450.
- 4. Ravikanth R. Acquired encysted hydrocele of the cord secondary to trauma in a child: sonological appearances of a rare entity. J Med Ultrasound 2020 Oct;30(1):65-66.
- 5. Janssen K, Klinkner D, Kumar T. Encysted hydrocele of canal of nuck: a case report with review of literature. J Surg Tech Case Rep 2011 Jul;3(2):97-98.
- 6. Manimaran D, Karthikeyan TM, Khan DM. Encysted spermatic cord hydrocele in a 60-year-old, mimicking incarcerated inguinal hernia: a case report. J Clin Diagn Res 2014;8(2):153-154.
- 7. Busigó JP, Eftekhari F. Encysted spermatic cord hydroceles: a report of three cases in adults and a review of the literature. Acta Radiol 2007 Dec;48(10):1138-1142.
- 8. Wani I, Rather M, Naikoo G, Gul I, Bhat Z, Baba A. Encysted hydrocele of cord in an adult misdiagnosed as irreducible hernia: a case report. Oman Med J 2009 Jul;24(3):218-219.
- 9. Senayli A, Senayli Y, Sezer E, Sezer T. Torsion of an encysed fluid collection. Scientific World Journal 2007 Apr 9;7:822-824.
- 10. Sugianto KY, Vijay Pramod S, Siregar S, Hernowo BS. Encysted spermatic cord hydroceles in 3-year-old boy, case report. Urol Case Rep 2021 Mar;38:101652.