A preterm, small-for-gestational-age male newborn (36 weeks; 1600 grams; < 3rd percentile) infant in our neonatal intensive care unit was diagnosed with early-onset hypoglycemia. Therefore, soon after birth, he was initiated on gavage feedings. The rising glucose infusion concentrations necessitated the placement of an umbilical venous line. At 48 hours of life, coffee-colored aspirates emerged, mimicking the initial stages of necrotizing enterocolitis. However, a soft abdomen on palpation, audible bowel sounds, and frequent meconium passages were reassuring.
An abdominal radiograph obtained to assess the placement of the umbilical venous catheter revealed a curvilinear lucency, raising clinical suspicion of a serious ailment [Figure 1]. The infant was kept nil per os; parenteral nutrition was started. A repeat X-ray and an ultrasound taken 24 hours after the initial examination suggested that the air collection was resolving. Soon, the aspirates cleared, and oral feeding was initiated. The infant was discharged in good health after two weeks. At a follow-up visit four months after birth, he was thriving and growing well. Informed consent was taken from the patient's mother.
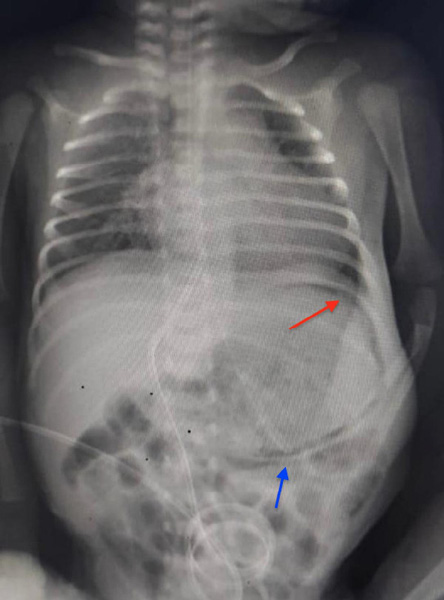 Figure 1: The initial anteroposterior abdominal radiograph of the newborn with an umbilical venous catheter in situ. Curvilinear gastric pneumatosis is seen (red arrow). The gavage tube is abutting the gastric wall (blue arrow).
Figure 1: The initial anteroposterior abdominal radiograph of the newborn with an umbilical venous catheter in situ. Curvilinear gastric pneumatosis is seen (red arrow). The gavage tube is abutting the gastric wall (blue arrow).
Question
1. What is the diagnosis?
a. Necrotizing enterocolitis.
b. Gastric pneumatosis.
c. Spontaneous intestinal perforation.
d. Intestinal malrotation.
e. Pneumoperitoneum.
Answer
b. Gastric pneumatosis
Discussion
Gastric pneumatosis is a distinct curvilinear lucency, paralleling and limited to the gastric curvature, which can be observed on a radiograph as shown in Figure 1. Gastric-outlet obstruction, critical illness, widespread necrotizing enterocolitis, sepsis, and asphyxia have been reported as etiologies.1–4 The postulated mechanisms include raised gastric pressure creating a mucosal rent, pneumomediastinum tracking into gastric musculature with positive pressure support application, or infection with gas-producing organisms.5,6 The extraluminal gas accumulation in pneumatosis intestinalis can be submucosal or subserosal. The intramural gas accumulation in the gastric musculature gives a characteristic curvilinear shape to the gastric wall. While pneumatosis intestinalis can involve any part of the large or small intestines, gastric pneumatosis is limited to the gastric area. A differential diagnosis of this condition is emphysematous gastritis, which may present with significant sickness.
Diagnosing gastric pneumatosis on an abdominal radiograph is straightforward. The management is directed towards the underlying etiology. In this case, the infant had a single risk factor of gavage tube placement, which is rare.5 A gastric mucosal tear from the pressure created while aspirating the gavage tube to check gastric contents might have been responsible for gastric pneumatosis in the patient. This injury is associated with coffee-brown colored aspirates. Our patient’s gavage tube-related gastric pneumatosis healed spontaneously and with supportive care.
Due to the subtle clinical signs of this condition, a radiograph is recommended for diagnosis. A stable newborn with isolated gastric pneumatosis generally responds well to conservative management.
Disclosure
The authors declare no conflicts of interest.
references
- Cohen HL, Chism PB, Radtke I. Excessive bright echoes sign for hypertrophic pyloric stenosis suggest the diagnosis: gastric pneumatosis and portal venous gas in infants suggest HPS. J Ultrasound Med 2017 May;36(5):1059-1063.
- 2. Angadi C, Chaurasia S, Priyadarshi M, Singh P, Basu S. Gastric pneumatosis in a neonate born late preterm on the first day of life. J Pediatr 2023 Mar;254:102-103.
- 3. Bayoumi MA, Elmalik EE. Gastric pneumatosis in a preterm infant following initial empiric antibiotic therapy. BMJ Case Rep 2021 Oct;14(10):e246446.
- 4. Abusalah ZG, George J. Preterm baby with gastric pneumatosis: a new association with a desirable outcome. BMJ Case Rep 2019 May;12(5):e230188.
- 5. Ting YJ, Chan KL, Wong SC, Chim S, Wong KY. Gastric pneumatosis in a premature neonate. AJP Rep 2011 Sep;1(1):11-14.
- 6. Ranjan V, Chowdhry BK, Kumar CM. Emphysematous gastritis in a newborn: Is it very rare or do we just miss it? J Neonatal Perinatal Med 2022;15(4):859-861.