Undifferentiated pleomorphic sarcoma (UPS) of the larynx is a rare malignancy with an unknown prevalence, as very few cases have been reported.1,2 Moreover, to our knowledge, no case involving the ventricles of the larynx has been reported. The paucity of cases and the variable behavior of UPS tumors make it challenging to arrive at optimal management plans.
Usually, surgical oncology patients are referred to the oncology team for further evaluation and decision-making. However, in this case, a meeting was held with a pathologist, an oncologist, and an otorhinolaryngologist to decide the treatment plan. Thus, this case report emphasizes the importance of a multidisciplinary team approach for managing UPS of the laryngeal ventricle to provide the best treatment option for the patient.
Case Report
A man in his seventies with diabetes mellitus and hypertension presented to our otorhinolaryngology clinic complaining of hoarseness of three months duration. He had no difficulty in eating, aspiration symptoms, otalgia, shortness of breath, or neck swelling. He was a non-smoker. His hoarseness was assessed as grade 2 based on the grade, roughness, breathiness, asthenia, and strain (GRBAS) scoring. Examination of the neck revealed no enlargement of cervical lymph nodes.
Investigation using a 70-degree angled scope revealed a lobulated mass arising from the middle third of the right vocal cord with adequate airway [Figure 1]. The patient underwent endoscopic laryngeal microsurgery under general anesthesia. Intraoperatively, we observed a mass occupying almost the entire length of right ventricle. The mass was adjacent to the anterior commissure but did not infiltrate it. The right vocal cord and right false cord were spared. The epiglottis, left vocal cord and false cord, arytenoids, and subglottic were normal. A decision for tumor excision and histopathological examination (HPE) was made. The right ventricular mass was excised; however, we were unable to remove the tumor completely, as its base had extended deep into the ventricles [Figure 2].
 Figure 1: A lobulated mass arising from the middle third of the right vocal cord is revealed intraoperatively.
Figure 1: A lobulated mass arising from the middle third of the right vocal cord is revealed intraoperatively.
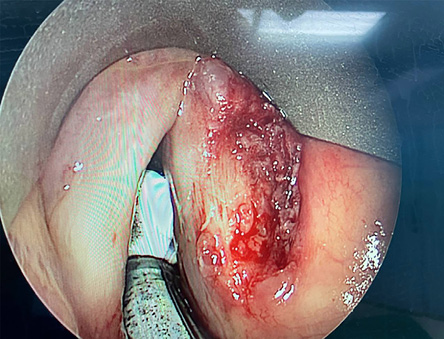 Figure 2: Intraoperatively, the base of the tumor is seen to extend deep into the right ventricle.
Figure 2: Intraoperatively, the base of the tumor is seen to extend deep into the right ventricle.
HPE of the right laryngeal ventricular mass showed that the tumor was covered with unremarkable squamous epithelium with diffuse infiltration of malignant cells within the stroma [Figure 3] and spindle cells with marked nuclear pleomorphism and abundant ill-defined cytoplasm. Multinucleation with abnormal mitotic figures were observed. The cells were strongly positive for vimentin [Figure 4] and focally positive for actin and CD34 expression. Thus, a diagnosis of UPS was reached. A deep biopsy of the ventricular mass revealed no malignant cells.
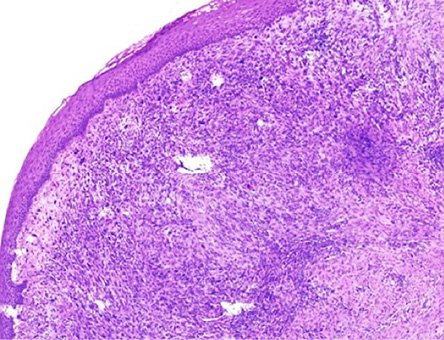 Figure 3: Histopathological image of the right laryngeal ventricular mass shows that the tumor is covered with unremarkable squamous epithelium with diffuse infiltration of malignant cells within
Figure 3: Histopathological image of the right laryngeal ventricular mass shows that the tumor is covered with unremarkable squamous epithelium with diffuse infiltration of malignant cells within
the stroma.
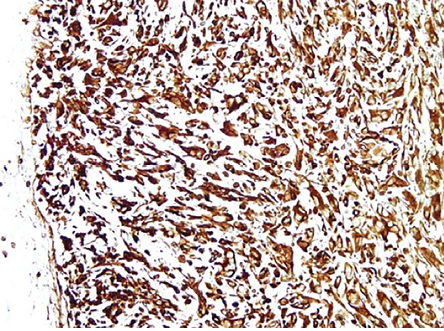 Figure 4: Immunohistochemistry demonstrates strong positivity for vimentin.
Figure 4: Immunohistochemistry demonstrates strong positivity for vimentin.
The patient subsequently underwent a computed tomography scan from the base of the skull to the abdomen, which revealed no cervical lymph nodes
or metastases.
Following discussions with the oncology team, we proceeded with postoperative radiotherapy. He underwent intensity-modulated radiation therapy with a radiation dose of 66 Gy in 33 fractions over six weeks. The radiation dose was chosen to account for the possibility of residual disease. Owing to the supraglottic location of the tumor, bilateral cervical nodes from levels II, III, and IV were also included in the radiation field. The ipsilateral cervical lymph nodes were irradiated with a microscopic dose of 60Gy, while the contralateral nodes received an even lower dose of 54Gy.
The patient tolerated radiotherapy treatment well, with only grade 1 mucositis and radiation dermatitis. On review one year after completion of radiotherapy, he had minimal hoarseness. Laryngoscopic examination revealed no mass and normal laryngeal inlet structures. The patient is currently undergoing regular surveillance follow-up. Informed consent was obtained from the patient.
Discussion
UPS, previously known as malignant fibrous histiocytoma, was first reported in 1964 and represents a soft tissue sarcoma.3,4 Sarcomas are uncommon malignancies of the head and neck, with laryngeal sarcomas accounting for less than one per cent of all cases.1,2,4 UPS has variable behavior ranging from slow-growing lesions to aggressive and destructive lesions with potential for systemic metastasis.5,6
UPS is a diagnosis of exclusion, making it a challenging process, as it must be differentiated from other malignant tumors such as sarcomatoid carcinoma, fibrosarcoma, myxofibrosarcoma, leiomyosarcoma, rhabdomyosarcoma, and osteosarcoma, which show comparable cellular pleomorphisms.5 This makes the role of the pathologist crucial. A diagnosis is made when HPE fails to reveal a line of differentiation after use of an adequate sample, in addition to taking into account the findings from ancillary diagnostic techniques such as immunohistochemistry.7 Smooth muscle actin is expressed in pleomorphic myogenic sarcomas, and markers such as vimentin, p53, and Ki67 are reportedly exhibited in UPS, although they are not disease-specific.8,9
In rarely reported diseases such as UPS, treatment plans must be generated through multidisciplinary discussions. In the current case, the otorhinolaryngologist and oncologist collaborated to develop the management plan. Surgery is the primary therapeutic approach for localized disease. The treatment of laryngeal UPS is based on UPS of other organs, which involves surgical excision with negative margins.9 The therapeutic approach for laryngeal sarcomas is dictated by their size, location, and biological characteristics. Since many laryngeal sarcomas show less infiltrative characteristics, and the risk of metastasis occurs later than in laryngeal carcinomas, surgical intervention has been a primary modality of treatment.2 Therefore, radical resection of UPS tumors is an effective modality for improving survival and decreasing recurrence. However, partial laryngectomy and laryngeal microsurgery have also been described with good outcomes.5
The role of radiotherapy in UPS has been controversial but has evolved over the last 30 years.2 Approximately 3–5% of UPS cases occur in patients who have received radiotherapy for other malignancies, making radiotherapy treatment controversial.3 Sarcomas are considered radioresistant. However, the Spanish Society of Medical Oncology guidelines show that perioperative radiotherapy decreases local recurrence but has no impact on survival. Postoperative adjuvant radiotherapy is considered for patients with high-grade tumors, positive surgical margins, larger tumors (> 5 cm), and recurrent lesions.2,10 A shared decision among the otorhinolaryngologist, pathologist, and oncologist must be made to give the best outcome for patients.
Conclusion
We have presented an extremely rare case of UPS of the laryngeal ventricle, which adds to the limited literature available. This case also highlights the importance of collaboration among the otorhinolaryngologist, pathologist, and oncologist in diagnosing and managing such rare conditions.
Disclosure
The authors declare no conflict of interest.
Acknowledgments
We would like to thank Dr. Elsie Jane Anastasius for helping in treating this patient.
references
- 1. Mishra H, Rastogi M, Mishra R, Gupta A, Srivastava RK, Srivastava A. Undifferentiated pleomorphic sarcoma of larynx: a rare entity with review of literature. Journal of Medical Science and Clinical Research 2015;3(9).
- 2. Liu C-Y, Wang M-C, Li W-Y, Chang S-Y, Chu P-Y. Sarcoma of the larynx: treatment results and literature review. J Chin Med Assoc 2006 Mar;69(3):120-124.
- 3. Chen S, Huang W, Luo P, Cai W, Yang L, Sun Z, et al. Undifferentiated pleomorphic sarcoma: long-term follow-up from a large institution. Cancer Manag Res 2019 Nov;11:10001-10009.
- 4. Wang Z, Tang Z, Zhao H, Zeng X, Han X, Zhang Q. Treatment of recurrent undifferentiated pleomorphic sarcoma of infratemporal fossa by surgery combined with carbon ion radiotherapy: one case report. Front Surg 2021 Aug;8:693774.
- 5. Cambruzzi E, Cruz RP, Gava VG, Pêgas KL. Undifferentiated high-grade pleomorphic sarcoma of the larynx treated with partial laringectomy. Braz J Otorhinolaryngol 2020 Dec;86(Suppl 1):14-16.
- 6. Aljariri AA, Alsaleh AR, Al-Enazi HA, Haider HA, Petkar M, Rahman W, et al. Glottic malignant fibrous histiocytoma: a case report and literature review. Case Rep Oncol 2021 Mar;14(1):641-646.
- 7. Chang RC, Dave SP, Robinson PG. Undifferentiated pleomorphic sarcoma of the parotid gland: a rare pediatric case. Head Neck 2008 Jul;30(7):970-973.
- 8. Benites BM, Miranda-Silva W, Fonseca FP, Oliveira CR, Fregnani ER. Undifferentiated pleomorphic sarcoma of the mandible. J Korean Assoc Oral Maxillofac Surg 2020 Aug;46(4):282-287.
- 9. Robles-Tenorio A, Solis-Ledesma G. Undifferentiated pleomorphic sarcoma. StatPearls, StatPearls Publishing 2023 [cited 2023 February 12]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK570612/.
- 10. de Juan Ferré A, Álvarez Álvarez R, Casado Herráez A, Cruz Jurado J, Estival González A, Martín-Broto J, et al. SEOM clinical guideline of management of soft-tissue sarcoma (2020). Clin Transl Oncol 2021 May;23(5):922-930.