Streptococcus constellatus is a gram-positive cocci classically associated with subdural empyema, liver abscess, frontal sinus abscess, and head and neck infections.1–4 While it has been sporadically reported as the causative organism in pleural empyema, it has not previously been documented in the context of e-cigarette or vaping product use-associated lung injury (EVALI).5 The prevalence of EVALI varies by region; one large US cohort reported a prevalence of 1.4 cases per 100 000 individuals aged 12–64 years old.6 Here, we report the case of a 13-year-old male who succumbed to EVALI complicated by Streptococcus constellatus empyema.
Case report
A 13-year-old male with a history of daily e-cigarette use and no prior medical illness presented to our hospital with a one-month history of intermittent cough and fever, along with worsening dyspnea over the past day. He denied any episodes of hemoptysis. Upon physical examination, his blood pressure was 152/82 mmHg, respiratory rate was 35 breaths/min, heart rate reached 150 beats/min, and oxygen saturation was 89% on room air. Lung auscultation revealed reduced air entry over the right lung, while the corresponding chest radiograph noted a right-sided pleural effusion [Figure 1]. Blood investigations revealed leukocytosis of 19.53 × 103/uL (reference range: 4–11× 103/uL) and a C-reactive protein level of 213.4 mg/L (reference range: < 5.0 mg/L). Renal function, liver function, and glucose investigations were all within the normal range. An arterial blood gas analysis, performed while the patient was on a rebreather face mask with a flow rate of 15 L/min, indicated decompensated metabolic acidosis with hyperlactatemia (pH 7.25, pO2 249 mmHg, pCO2 30 mmHg, HCO3- 13.2 mmol/L, and lactate 8.2 mmol/L). Due to worsening respiratory distress, the patient was subsequently intubated and transferred to the high-dependency unit.
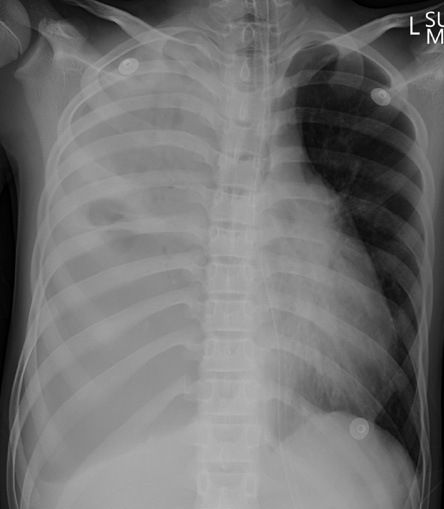 Figure 1: Chest X-Ray on 2 August 2022. The frontal chest radiograph shows complete opacification of the right hemithorax, with evident mass effect resulting in tracheal and mediastinal deviation to the left. The left lung field appears clear.
Figure 1: Chest X-Ray on 2 August 2022. The frontal chest radiograph shows complete opacification of the right hemithorax, with evident mass effect resulting in tracheal and mediastinal deviation to the left. The left lung field appears clear.
Bedside ultrasound revealed a right-sided multiseptated collection. Thoracocentesis yielded purulent fluid, prompting the placement of a chest drain [Figure 2]. Pleural fluid analysis revealed a protein level of 16 g/L and a lactate dehydrogenase level of 5355 u/L. Due to the need for high-ventilator settings and persistent bubbling from the chest
drain, a bronchopulmonary fistula was suspected, leading to the insertion of a second chest tube to optimize ventilation. Informed consent was obtained from the patient’s father.
 Figure 2: Chest X-Ray on 3 August 2022. The frontal radiograph, obtained post-intubation, reveals lucency along the lower zone of the right hemithorax consistent with pneumothorax, resulting in compression of the adjacent lungsgarette or vaping product use-associated lung injury.
Figure 2: Chest X-Ray on 3 August 2022. The frontal radiograph, obtained post-intubation, reveals lucency along the lower zone of the right hemithorax consistent with pneumothorax, resulting in compression of the adjacent lungsgarette or vaping product use-associated lung injury.
Discussion
Empyema caused by Streptococcus constellatus is commonly reported in the elderly, particularly those with comorbidities such as diabetes mellitus. A small retrospective series demonstrated a relatively low mortality rate of 11.1%; however, more than half of the patients developed respiratory failure, and a third developed severe pneumonia, including acute respiratory distress syndrome and septic shock. Early diagnosis and timely treatment are essential in reducing mortality due to pleural infection.7 The Centers for Disease Control and Prevention (CDC) have proposed the following diagnostic criteria for a confirmed case of EVALI: (1) use of an e-cigarette or a related product (e.g., vaping or dabbing) within 90 days of symptom onset; (2) presence of lung opacities on chest imaging (radiograph or CT scan); (3) exclusion of pulmonary infection; and (4) absence of a more likely alternative diagnosis (e.g., cardiac, neoplastic, and rheumatologic).8
In this case, the patient did not undergo a complete pulmonary infectious work-up, such as a respiratory viral panel or influenza testing. However, he met the remaining criteria for EVALI, and according to CDC definitions, he would be classified as a probable case of EVALI. Alternatively, if clinicians encounter a positive result on an infectious work-up but do not believe that the presentation is solely due to underlying infection, the patient may also be considered a probable case of EVALI.9 Ultimately, EVALI remains as a diagnosis of exclusion, as no direct confirmatory testing exists.10
In cases of bilateral effusion due to pneumonia, the mortality rate can increase by 6.5 times compared to patients hospitalized with pneumonia alone. By definition, a parapneumonic effusion refers to any pleural effusion occurring secondary to pneumonia (bacterial or viral) or lung abscess, with an abscess termed as an empyema when pus is present in the pleural space.11 Several cases documenting complications of vaping have been reported in the literature. For example, a 38-year-old female with a history of vaping and e-cigarette use developed a left-sided empyema, which was managed with intravenous antibiotics and fibrinolytics.12 Another report described a 26-year-old male with a vaping history who developed a loculated empyema requiring surgical decortication.12 It has been postulated that vape-related empyema results from a transformation of phosphatidylcholines, a component of surfactant, from a gel to a liquid crystalline phase when exposed to tocopherols such as vitamin E acetate found in vape liquid.13 This transformation leads to
alveolar dysfunction.13
The severe presentation and eventual death of the patient were likely attributed to delayed medical attention. One contributing factor may have been the patient’s undocumented immigration status, possibly hesitating to seek medical care promptly.
Conclusion
This case underscores the potential risks of vaping while emphasizing the importance of early management in pleural infections. Pleural empyema is a potential complication of EVALI. Clinicians are advised to be vigilant in obtaining a history of vape use, especially when dealing with non-immunocompromised individuals of younger age who present with severe pleural infections.
Disclosure
The authors declare no conflicts of interest.
references
- Şahin S, Yazar U, Cansu A, Kul S, Kaya S, Özdoğan EB. Is sinusitis innocent?–unilateral subdural empyema in an immunocompetent child. Indian J Pediatr 2015 Nov;82(11):1061-1064.
- 2. Atemnkeng F, Al-Ttkrit A, David S, Alataby H, Nagaraj A, Diaz K, et al. An unusual case of intraabdominal abscess after a colonoscopy with polypectomy. J Med Cases 2021 Aug;12(8):301-305.
- 3. Carrera W, Lewis WB, Silkiss RZ. Frontal sinus abscess with cutaneous fistula secondary to Streptococcus constellatus. Orbit 2021 Apr;40(2):171.
- 4. Hirai T, Kimura S, Mori N. Head and neck infections caused by Streptococcus milleri group: an analysis of 17 cases. Auris Nasus Larynx 2005 Mar;32(1):55-58.
- 5. Lin J, Zhang Y, Bao C, Lu H, Zhong Y, Huang C, et al. The clinical features and management of empyema caused by Streptococcus constellatus. Infect Drug Resist 2022 Oct;15:6267-6277.
- 6. Friedman AS. Association of vaping-related lung injuries with rates of e-cigarette and cannabis use across US states. Addiction 2021 Mar;116(3):651-657.
- 7. Davies HE, Davies RJ, Davies CW; BTS Pleural Disease Guideline Group. Management of pleural infection in adults: British thoracic society pleural disease guideline 2010. Thorax 2010 Aug;65(Suppl 2):ii41-ii53.
- 8. Aldy K, Cao DJ, Weaver MM, Rao D, Feng SY. E-cigarette or vaping product use-associated lung injury (EVALI) features and recognition in the emergency department. J Am Coll Emerg Physicians Open 2020 Jun;1(5):1090-1096.
- 9. Blount BC, Karwowski MP, Shields PG, Morel-Espinosa M, Valentin-Blasini L, Gardner M, et al; Lung Injury Response Laboratory Working Group. Vitamin E acetate in bronchoalveolar-lavage fluid associated with EVALI. N Engl J Med 2020 Feb;382(8):697-705.
- 10. Traboulsi H, Cherian M, Abou Rjeili M, Preteroti M, Bourbeau J, Smith BM, et al. Inhalation toxicology of vaping products and implications for pulmonary health. Int J Mol Sci 2020 May;21(10):3495.
- 11. Light RW, Girard WM, Jenkinson SG, George RB. Parapneumonic effusions. Am J Med 1980 Oct;69(4):507-512.
- 12. Patil SM, Beck PP, Patel TP, Dale Swaney R, Dandachi D, Krvavac A. Electronic vaping-induced methicillin-sensitive Staphylococcus aureus pneumonia and empyema. Case Rep Infect Dis 2021 Mar;2021:6651430.
- 13. Malik B, Kalantary A, Ghatol A, Kunadi A. Vaping-induced sepsis and rapidly evolving pleural effusion in a young, otherwise healthy male. Cureus 2022 May;14(5):e25327.