|
Abstract
Objectives: The morphology and anatomical relationship of periorbital features vary according to age, sex and ethnicity. Standard database regarding periorbital region is available for other ethnic groups. Since there is no data available in the literature, specifically for south Indian ethnic adults, the present study was carried out to determine the normal average values for South Indian ethnic population related to gender.
Methods: Anthropometric measurements of both eyes were done on standardized frontal view photograph of 200 South Indian ethnic adults aged 18 to 26 years. Parameters included were palpebral fissure width (PFW), palpebral fissure height (PFH), palpebral fissure inclination (PFI), outercanthal distance (OCD), interpupillary distance (IPD), intercanthal distance (ICD) and comparisons were made between the genders using the independent t test.
Results: Significant sexual dimorphism was noted in the given parameters. Palpebral fissure width (male: 31.08 mm; female: 29.90 mm), palpebral fissure inclination (male: 5.053°; female: 6.102°), outercanthal distance (male: 95.55 mm; female: 92.44 mm) and interpupillary distance (male: 66.72 mm; female: 62.59 mm). The palpebral fissure height (male: 11.30 mm; female: 11.58 mm) and intercanthal distance (male: 34.27 mm; female: 33.41 mm) showed no significant sexual differences.
Conclusion: Statistically significant differences were found between South Indian ethnic males and female in certain key parameters. The present study suggests that ethnicity and gender should be considered in orbital surgery. To individualize the treatment planning and diagnosis, it is important for the surgeons to have knowledge of these local norms.
Keywords: Aesthetics; Anthropometry; Database; Orbital; Palpebral fissure.
Introduction
The bilateral orbital region which is located in the upper face acts as a key determinant in the perception of facial attractiveness, youthfulness and health. The eye fissure dimensions and interorbital distance may be altered in facial deformities. To quantify the deformity, the patient’s measurements have to be compared with the normal values which are specific for patient’s race, age and sex. There are certain studies in the literature indicating that the morphology and anatomical relationship of palpebral fissure varies according to age, sex and ethnicity.1-5 From the surgical point of view, though the number of advanced corrective and surgical procedures have been developed in the field of reconstructive surgery, the lack of knowledge of the variations in the morphological and anatomical relationship of periorbital structures among different ethnic groups may hamper the surgeon’s efforts to retain the ethnical features.2 Thus, the knowledge of anatomic relations, morphology, coupled with aesthetical criteria of the patient population is a crucial part of treatment planning to achieve ideal postoperative outcomes, particularly in bilateral conditions.1,3 Since the normal data base of one ethnic group may not represent the others, there is a requirement for ethnically specific database. A standard database which gives a normal range of orbital dimension for South Indian ethnic population would be useful for a wide range of fields in designing products like optical spectacle frames and lenses to fit most people.4 In areas like ophthalmology, plastic and reconstructive surgery, the data can be useful in surgical procedures (ocular prosthetics, Blepharoplasty), diagnostic procedures,3,5 and in studies involving facial attractiveness.6 Anthropometric data for various ethnic and racial groups have been established in many studies.1-21 Lakshminarayana et al.7 have reported the interorbital distance measurements for South Indian children. However, there are no data in the literature available specifically for South Indian adults. The aim of the present study was to analyze the palpebral fissure dimensions and its position to generate normative values for South Indian ethnic adults and secondarily to evaluate the association of sexual dimorphism on these measured parameters.
Methods
A total of 205 South Indian ethnic medical students were randomly chosen at Manipal University, out of which 200 subjects (100 males and 100 females) were evaluated. Five subjects were excluded from the study as three subjects had a previous history of periocular trauma, surgery and two were of mixed ethnic origins. The study was approved by Manipal university ethics committee (UEC/58/2010). After obtaining informed written consent, the subjects were photographed in the frontal view with a cannon model EOS 1000 D SLR camera. A tripod was used for stability and to correct the height of the camera according to subject’s body height. The camera was aligned to the axial plane of the eye by an inbuilt camera grid. A scale bar was framed alongside the subject to allow the measurement at life size. Then the image was recorded with standard head position and eyes open in primary gaze.22,23 Two examiners independently measured the predetermined positions on the standardized photographs using a measuring software (Image J analyser); the mean of the two examiners’ values was used. A third reading was taken if the initial two measurements showed a large discrepancy, and the two closest readings were then considered.
The following measurements were taken on the standardized photographs:
I. Palpebral fissure measurements (Fig. 1):
Palpebral fissure width (PFW)
Palpebral fissure height (PFH)
Palpebral fissure inclination (PFI)
II. Canthal (Medial and lateral) and interpupillary distances
(Fig. 2):
Outercanthal distance (OCD)
Interpupillary distance (IPD)
Intercanthal distance (ICD)
The mean anthropometrical values of the measurements were compared between either sexes using the independent t test. The Technical error measurement (TEM), relative technical error measurement values (r TEM %) of intra-observer and interobserver, as well as coefficient reliability (R), were evaluated for all the measurements.24,25 A pilot study was done to calculate the sample size. This was calculated using a standard difference of 0.58, alpha of 0.05 and a power of 0.9.
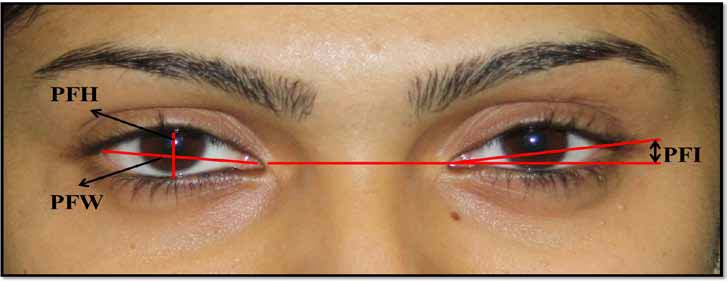
Figure 1: Palpebral fissure measurements. PFW = Distance between the medial and lateral canthus; PFH= Distance between inferior margin of eyelid to superior eyelid margin over the pupil; PFI = Palpebral fissure inclination in degree (angle between intersecting lines, from the horizontal reference line, drawn through the medial canthi to the lateral canthus).
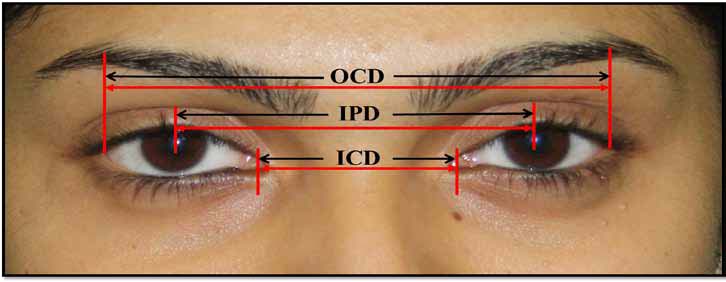
Figure 2: Canthal (medial and lateral) and interpupillary distance measurements. OCD = Distance between the lateral canthus; IPD= Distance between the pupil, ICD = Distance between the medial canthus.
Results
The mean values of right and left eye fissure were taken together. The mean values and standard deviation of palpebral fissure shape and interorbital distance measurements are shown in Table 1. The intra-observer and inter-observer TEM, r TEM %, Coefficient of reliability (R) values are presented in Table 2.
Table 1: Comparison of palpebral fissure and interorbital distance measurements according to gender.
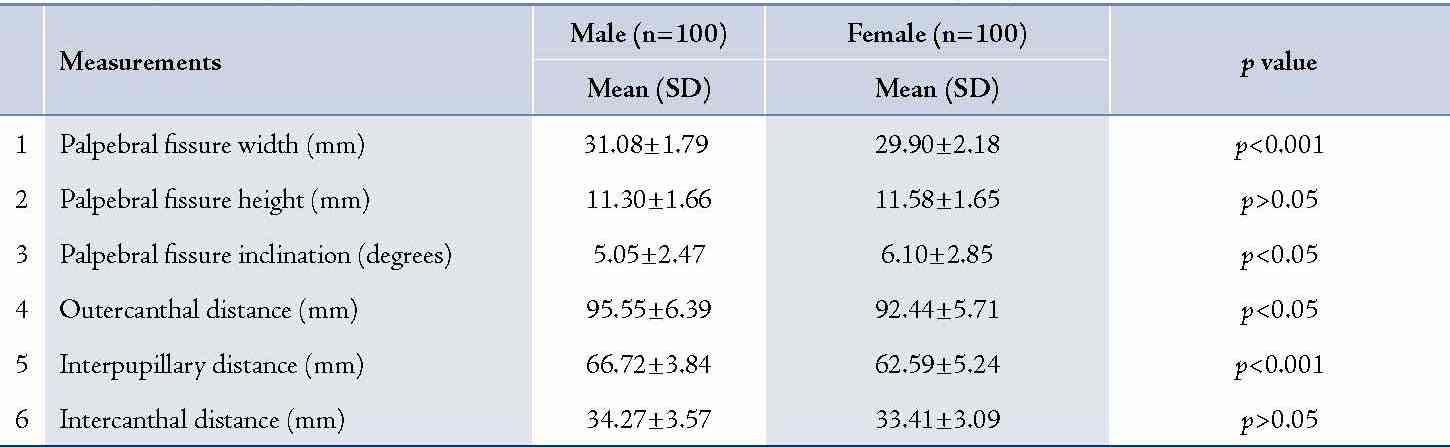
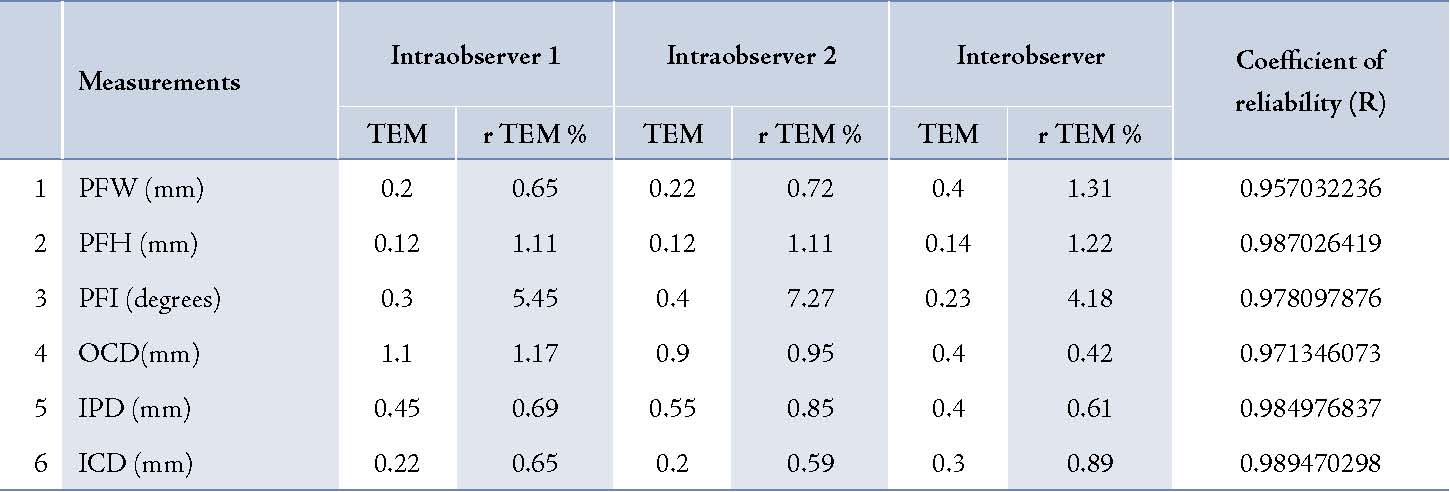
Table 2: Intraobserver and interobserver technical error of measurement (TEM), relative TEM % and coefficient of reliability (R).
The mean anthropometrical values of the palpebral fissure and interorbital distance were compared between the two sexes using the independent t test. The mean value of palpebral fissure width was 31.08 ± 1.79 mm in males and 29.9 ± 2.18 mm in females. The mean value of palpebral fissure height was 11.3 ± 1.66 mm in males and 11.58 ± 1.65 mm in females and the palpebral fissure slant was 5.05 ± 2.47° in males and 6.10 ± 2.85° in females. The average outercanthal distance for males and females were 95.55 ± 6.39 mm and 92.44 ± 5.71 mm, respectively. The average interpupillary distance for males and females were 66.72 ± 3.84 mm and 62.59 ± 5.24 mm, respectively; and the intercanthal for males and females were 34.27 ± 3.57 mm and 33.41 ± 3.09 mm, respectively. There was a significant difference in the palpebral fissure width, (p<0.001), palpebral fissure inclination (p<0.001), outer canthal distance (p<0.05), and interpupillary distance (p<0.001) between males and females. There was no significant difference in the palpebral fissure height (p>0.05) or inter-canthal distance (p>0.05) between the two sexes.
The intra observer TEM value ranged between 0.12 and 1.1, while r TEM % ranged between 0.65 and 7.27. Interobserver TEM values ranged between 0.14 and 0.4, and r TEM % ranged between 0.42 and 4.18. Coefficient of reliability (R) was high, ranging between 0.96 and 0.99.
Table 3: Compilation of palpebral fissure parameters of various population.
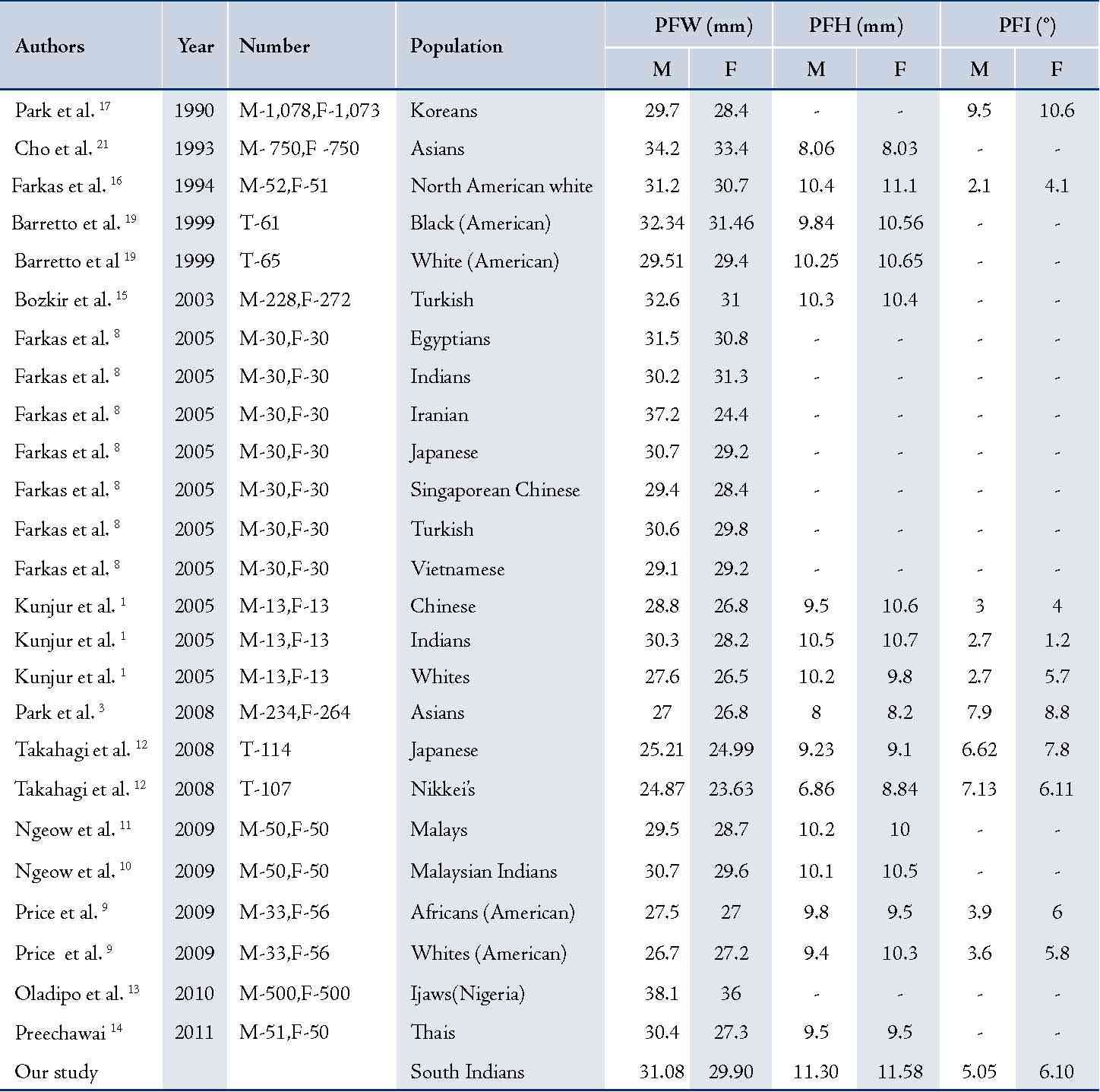
M: male; F: female; T: total; PFW: palpebral fissure width; PFH: palpebral fissure height; PFI: palpebral fissure inclination.
Table 4: Compilation of OCD, IPD and ICD measurements of various populations.
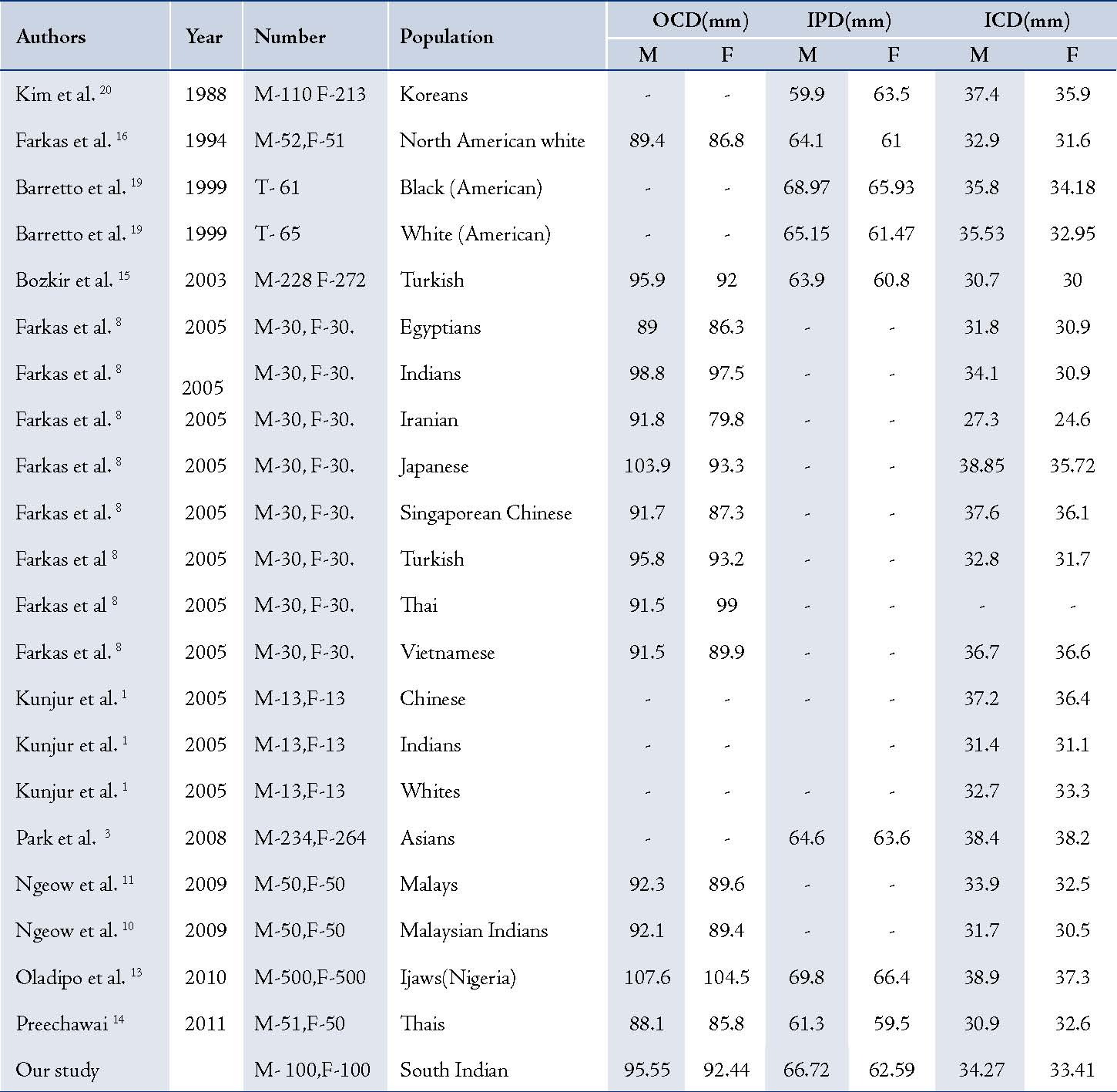
M: male; F: female; T: total; ICD: Inintercanthal distance; OCD: outercanthal distance; IPD: interpupillary distance.
Discussion
In the present study, the shape and position of the palpebral fissure of the South Indian ethnic population were evaluated (Table 1), and the data were compared with other racial and ethnic groups (Tables 3,4). Variations and similarities were detected in certain key parameters between the South Indian ethnic population and other populations.
Palpebral fissure width: In our study, the male had longer palpebral fissure than the female subjects and they showed statistically significant sexual differences (males: 31.08 mm; females: 29.9 mm). In contrast, Farkas et al.8 and Price et al.9 reported slightly higher values in females than the male subjects among Indians (males: 30.2 mm; females: 31.3 mm) aged 18-30 and Caucasians (males: 26.7 mm; females: 27.2 mm) aged 20-39, respectively (Table 2). Ngeow reported a female mean value of 29.6 mm for Malaysian Indians aged 18-25.10 While, Farkas et al. reported female mean value of 29.8 mm for Turkish population aged 18-30 years.8 The values from the studies by Ngeow,10 and Farkas et al.8 for female subjects were similar to those of South Indian ethnic female subjects. Takahagi et al.12 reported mean values for Nikkeis' (male: 24.87 mm; female: 23.63 mm) and Japanese (male: 25.21 mm; female: 24.99 mm) aged 20-29 years. Oldipo et al.13 reported a superior mean value (male: 38.1; female: 36 mm) for Ijaws of Nigeria aged 18-65 years. South Indian ethnic male and female subjects had a longer PFW than the Nikkei’s and Japanese. Shorter PFW compared to Ijaws of Nigeria.13 The longer palpebral fissure may be associated with a wider and larger face
Palpebral fissure height: The mean value of palpebral fissure height for South Indian ethnic male and female subjects was almost similar with no significant sexual difference (Table 2) similar to Thais,14 Japanese,12 and Turkish population.15 Preechawai et al. in a study on Thais observed interestingly similar mean values in both male and female subjects (9.5 mm) aged 20-40 years.14 This is in contrast to Takahagi et al. who found large variability between male and female subjects (male, 6.86 mm; female, 8.84 mm).12 Farkas et al. reported a female mean value of 11.1 mm for Caucasians.16 This article reports a similar female mean value of 11.58 mm. When compared to previous studies, PFH in the South Indian ethnic population had wider eyes compared to other racial groups.
Palpebral fissure inclination (degrees): In the present study, South Indian ethnic adults showed mongoloid type of palpebral fissure. Adler suggested that the eyes look aesthetically pleasing if both medial and lateral canthi are at the same level.26 According to western aesthetic norms, the lateral canthus should lie slightly higher than the medial canthus. In the present study, significant sexual difference was found, with more obliquity of palpebral fissure in females than in males (males: 5.03°; females: 6.102°). Kunjur et al. in a study on adult Indians, observed that PFI in males is more oblique than in females which is at variance with the present study.1 He reported mean values for Chinese (males: 3°; females: 4°), Indian (males: 2.7°; females: 1.2°) and White (males: 2.7°; females: 5.7°) racial groups. In the present study, mean values were higher when compared to the reports by Kunjur et al.1 Takahagi et al.12 reported a female mean value of 6.1°, while Nikkei’s and Price reported a female mean value of 6° in African Americans.9 The present study also reports of a similar mean value of 6.1° in females. Park et al.17 have reported PFI mean values (male: 9.5°; female: 10.6°) for Koreans, which was higher compared to other racial groups. The dimensions of palpebral fissure are normally affected by the configuration of periorbital features. The normative values of size and slant of palpebral fissure may be valuable for the clinician in the assessment of ptosis, malar hypoplasia, and epicanthus inversus. These data can also be used as a reference for setting aesthetic norms for the South Indian population.
Outercanthal, intercanthal and interpupillary distances: Outer-canthal distance, inner-canthal distance and interpupillary distance are commonly used in assessment of hypertelorism. Kulkarani et al. have suggested that a clear distinction should be made between the measurements in the assessment of hypertelorism.18 The ICD and OCD measurements are usually affected by the surrounding soft tissue. The ICD may be increased due to broad nasal bridge. Hence, he suggested that IPD is an accurate measure for hypertelorism. Abdulla et al.27 used ICD to predict the combined width of the maxillary six anterior teeth, as well as for selection.
4a. Outercanthal distance: In the present study, mean values for OCD distance for males was higher than those for females. Farkas et al. reported a higher value in females than in males for Thais.8 Bozkir et al. in a study on Turkish adults reported mean values (male: 95.9 mm; female: 92 mm), which were similar to our study (male: 95.55 mm; female: 92.44 mm).15 Oldipo et al. in a study on Ijaws of Nigeria reported mean OCD of 107.6 mm for males, and 104.5 mm for females, which are higher compared to our findings.13
4b. Interpupillary distance: The mean value of IPD obtained in the present study fits the Caucasian norms (60 to70 mm). We also observed that these values were significantly higher in males than in females (males: 66.72 mm; females: 62.59 mm). Barretto et al.19 also reported male mean value of 65.15 mm for Whites and Kim et al.20 reported female mean value of 63.5 mm for Koreans. The results of Barretto et al.19 and Kim et al.20 were closer to our findings. The IPD was wider in Ijaws of Nigeria (male: 69.8 mm; female: 66.4 mm), compared to South Indian ethnic adults. While Preechawai et al.14 reported female mean value of 59.5 mm for Thais and Kim et al.20 reported male mean value of 59.9 mm for Koreans. The IPD distance was wider in South Indian adults compared to Thais and Koreans.
4c. Intercanthal distance: According to Caucasians norms, the ICD ranges from 30 to 35 mm. In the present study, mean value of ICD in both genders (male: 34.27 mm; female: 33.41 mm) follows the Caucasians norms. In our study, no significant gender difference was observed in mean ICD. Farkas et al.8 reported a mean value of 34.1 mm in Indian males and Kunjur at al.1 reported 33.3 mm in White females. Our findings of ICD in both the sexes (male: 34.27 mm; female: 33.41 mm) were similar to the figures reported by Farkas et al.8 and Kunjur et al.1 When compared to our study, Farkas et al.8 reported lower mean values of 27.3 mm for males and 24.6 mm for female subjects aged 18-30 in a study on an Iranian population. Oldipo et al.13 reported higher values (male: 38.9 mm; female: 37.3 mm) compared to our study.
The similarities and variations in the results with certain ethnic groups can be explained on the anthropological point of view. Based on the physical anthropology, the Asian groups PFW of South Indian female ethnic group was identical to the mean value of Malaysian Indians and Japanese, while PFI was similar to Nikkei’s. Only ICD of South Indian male was similar to Indian males. The mean value of PFH in both sexes was superior compared to that of other ethnic groups. Interestingly, we noted that none of the parameters of south Indian ethnic groups were identical to Chinese, Koreans or Thais. Among the Middle Eastern groups, PFW of South Indian males was similar to that of Egyptian male ethnic group, while females PFW value were identical to the Turkish female ethnic group. The mean values OCD of both sexes of Turkish ethnic group were identical to south Indians. Although parameters like PFH, IPD and ICD showed lower values compared to south Indians, the PFW was greater in Iranians. In the African groups, PFW, OCD, IPD, ICD was greater than the south Indian population.
However, the PFH, PFI was not greater in Africans. PFW of Afro-Americans was lower compared to south Indians. Africans showed wide ICD because of the broad wide nasal bridge. The PFH, PFI and ICD of the Caucasian female group was identical to the mean value of South Indian female ethnic group. The PFW of both sexes in Caucasians and south Indians were identical. OCD distance was greater in South Indians.
Based on paleoanthropology, Malaysian Indians' facial characteristics are similar to their South Indian counterparts, because both groups are Dravidians. Most of the Malaysian Indians are descendants of South India who live in Malaysia. In the present study, we observed that the South Indians present with Turkish and Caucasian features probably because Indians belong to the subgroups of Caucasoid called Indo-Dravidian.
We also observed some similarities with Japanese who belong to the mongoloids group. Risley, based on anthropometric measurement observed the mongoloid features in Indian population and he classified them as Mongolo-Dravidians type.28 Malhotra, stated on the basis of morphological features, the mongoloid and Caucasoid contribute to the biological composition of Indian population. 29
The variation in results from the previous studies may also be due to measuring techniques. The anthropometric data in orbital region have been collected by direct (rulers and calipers) and indirect measuring techniques (camera and computer analysis). In the present study, the morphology of orbital region was studied using indirect anthropometry (photogrammetry technique and software). Coombes et al. have suggested that digital photography combined with computer analysis offers advantage over direct anthropometry, the method is simple, standardized, and documentable and can be applied in research.30
Conclusion
The results from this study construe that there is a statistically significant gender difference in certain parameters between males and females. When the data of the present study were compared with the previous reports, the measured parameters showed variations and similarities (racial and sexual) with other populations. Variations in the morphology of orbital features according to race, sex and ethnicity may affect the treatment planning and diagnosis during facial analysis. Hence, during reconstructive surgery, it is important for the surgeons to have knowledge of local norms during facial analysis in order to evaluate and modify the disproportionate features without disturbing the ethnical features. The results of this study will be of immense use in surgical procedures like ocular prosthetics, blepharoplasty and in forensic science to trace missing individuals by applying facial reconstruction techniques, dentistry, genetics and paleoanthropological studies.
Acknowledgements
The authors reported no conflict of interest and no funding was received for this work.
References
1. Kunjur J, Sabesan T, Ilankovan V. Anthropometric analysis of eyebrows and eyelids: an inter-racial study. Br J Oral Maxillofac Surg 2006 Apr;44(2):89-93.
2. Sim RS, Smith JD, Chan AS. Comparison of the aesthetic facial proportions of southern Chinese and white women. Arch Facial Plast Surg 2000 Apr-Jun;2(2):113-120.
3. Park DH, Choi WS, Yoon SH, Song CH. Anthropometry of asian eyelids by age. Plast Reconstr Surg 2008 Apr;121(4):1405-1413.
4. Osuobeni EP, al-Gharni SS. Ocular and facial anthropometry of young adult males of Arab origin. Optom Vis Sci 1994 Jan;71(1):33-37.
5. Ferrario VF, Sforza C, Colombo A, Schmitz JH, Serrao G. Morphometry of the orbital region: a soft-tissue study from adolescence to mid-adulthood. Plast Reconstr Surg 2001 Aug;108(2):285-292, discussion 293.
6. Edler R, Agarwal P, Wertheim D, Greenhill D. The use of anthropometric proportion indices in the measurement of facial attractiveness. Eur J Orthod 2006 Jun;28(3):274-281.
7. Lakshminarayana P, Janardhan K, David HS. Anthropometry for syndromology. Indian J Pediatr 1991 Mar-Apr;58(2):253-258.
8. Farkas LG, Katic MJ, Forrest CR, Alt KW, Bagic I, Baltadjiev G, et al. International anthropometric study of facial morphology in various ethnic groups/races. J Craniofac Surg 2005 Jul;16(4):615-646.
9. Price KM, Gupta PK, Woodward JA, Stinnett SS, Murchison AP. Eyebrow and eyelid dimensions: an anthropometric analysis of African Americans and Caucasians. Plast Reconstr Surg 2009 Aug;124(2):615-623.
10. Ngeow WC, Aljunid ST. Craniofacial anthropometric norms of Malaysian Indians. Indian J Dent Res 2009 Jul-Sep;20(3):313-319.
11. Ngeow WC, Aljunid ST. Craniofacial anthropometric norms of Malays. Singapore Med J 2009 May;50(5):525-528.
12. Takahagi RU, Schellini SA, Padovani CR, Ideta S,Katori N, Nakamura Y. Oriental oculopalpebral dimensions: Quantitative comparison between Orientals from Japan and Brazil. Clin Opthalmol2008Sep; 2(30):563-567.
13. Oladipo GS, Okoh PD, Hart JS. Anthropometric Study of Ocular Dimensions in Adult Ijaws of Nigeria. Res. J. Medicine & Med. Sci 2010;5(2):121-124.
14. Preechawai P. Anthropometry of eyelid and orbit in four southern Thailand ethnic groups. J Med Assoc Thai 2011 Feb;94(2):193-199.
15. Bozkir MG, Karakaş P, Oĝuz O. Measurements of soft tissue orbits in Turkish young adults. Surg Radiol Anat 2003 Apr;25(1):54-57.
16. Farkas LG. Anthropometry of the Head and Face. 2nd ed. New York: Raven Press, 1994.
17. Park DM, Song JW, Han KW, Kang JS. Anthropometry of Korean eyelids. J. Korean Soc. Plast. Reconstr. Surg 1990;179(5):822.
18. Kulkarni ML, Rajendran NK, Sangam DK. Inner canthal, outer canthal and inter pupillary distance in newborns. Indian Pediatr 1992 Jun;29(6):759-763.
19. Barretto RL, Mathog RH. Orbital measurement in black and white populations. Laryngoscope 1999 Jul;109(7 Pt 1):1051-1054.
20 .Kim CJ, Ham KS, Kim Y, Cho YJ. A facial anthropometric study on the Korean youths. J. Korean Soc. Plast.Reconstr. Surg 1988;15(5):427.
21 .Cho JH, Han KH, Kang JS. Normal anthropometric values and standardized templates of Korean face and head. J. Korean Soc. Plast. Reconstr. Surg 1993;20(5):995-1005.
22. DiBernardo BE, Adams RL, Krause J, Fiorillo MA, Gheradini G. Photographic standards in plastic surgery. Plast Reconstr Surg 1998 Aug;102(2):559-568.
23. Fernández-Riveiro P, Smyth-Chamosa E, Suárez-Quintanilla D, Suárez-Cunqueiro M. Angular photogrammetric analysis of the soft tissue facial profile. Eur J Orthod 2003 Aug;25(4):393-399.
24. Weinberg SM, Scott NM, Neiswanger K, Marazita ML. Intraobserver error associated with measurements of the hand. Am J Hum Biol 2005 May-Jun;17(3):368-371.
25. Ulijaszek SJ, Kerr DA. Anthropometric measurement error and the assessment of nutritional status. Br J Nutr 1999 Sep;82(3):165-177.
26. Adler FH. Physiology of the Eye. 2nd ed. St. Louis: Mosby; 1975:13.
27. Abdullah MA. Inner canthal distance and geometric progression as a predictor of maxillary central incisor width. J Prosthet Dent 2002 Jul;88(1):16-20.
28. Risley H. Sir 1969. The People of India. (1915). Delhi: Orient Book Reprint Corporation, Reprinted.
29. Malhotra KC. Morphological composition of the people of India. J Hum Evol 1978 Jan;7(1):45-53 .
30. Coombes AG, Sethi CS, Kirkpatrick WN, Waterhouse N, Kelly MH, Joshi N. A standardized digital photography system with computerized eyelid measurement analysis. Plast Reconstr Surg 2007 Sep;120(3):647-656.
|