A 65-year-old female presented with chronic back pain after undergoing two months’ treatment elsewhere with little improvement. She had a history of a trivial injury some eight months earlier when she received treatment and became ambulatory. For the previous three months, she was having difficulty being supine. Her pain and discomfort were obvious. X-ray radiographs in supine and sitting postures suggested a collapse opening up at D12 level suggestive of a void [Figure 1]. Computed tomography (CT) confirmed a ‘vacuum sign’ seen on coronal and axial cuts [Figure 2]. Magnetic resonance imaging (MRI) clearly showed an edema at that particular level [Figure 2]. Laboratory test results ruled out any infection or malignancy. The patient underwent a single-level kyphoplasty (KP) under anesthesia. On the following day, her pain score (visual analog score) had tremendously improved from 8 to 1. The chest x-ray and CT scan showed satisfactory cement filling and height restoration [Figure 3]. She received anti-osteoporotic treatment and was doing well at the one year follow-up.
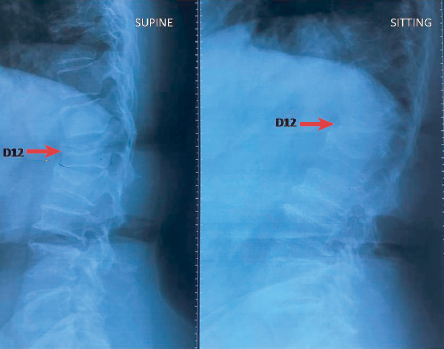
Figure 1: Loading x-ray showing inter-vertebral collapse (arrow).

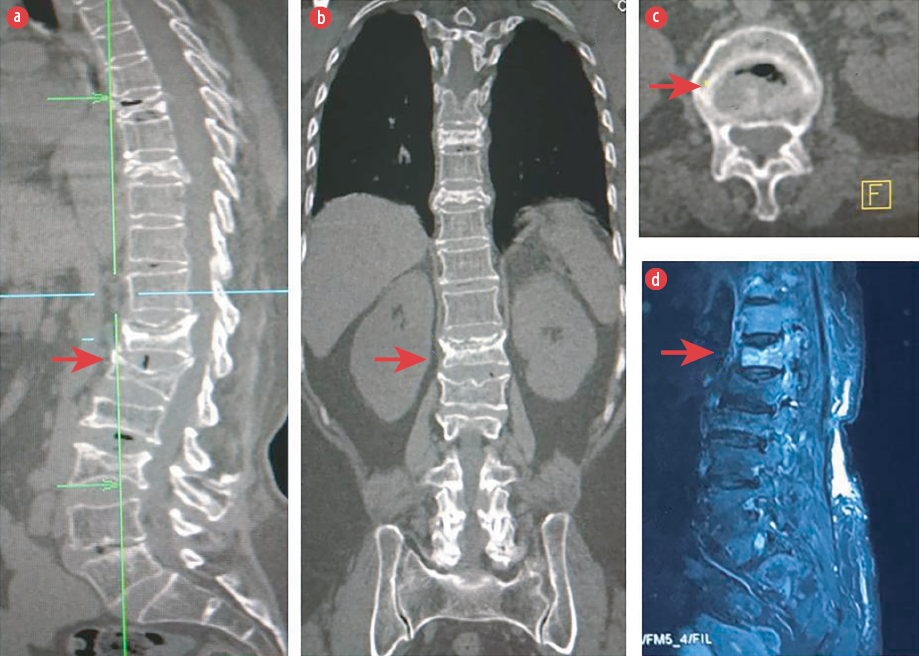 Figure 2: CT scans: (a and b) show intervertebral cleft in sagittal and coronal and (c) vacuum in axial cuts. (d) Fat suppressed MRI showing the affected vertebrae with patchy edema.
Figure 2: CT scans: (a and b) show intervertebral cleft in sagittal and coronal and (c) vacuum in axial cuts. (d) Fat suppressed MRI showing the affected vertebrae with patchy edema.

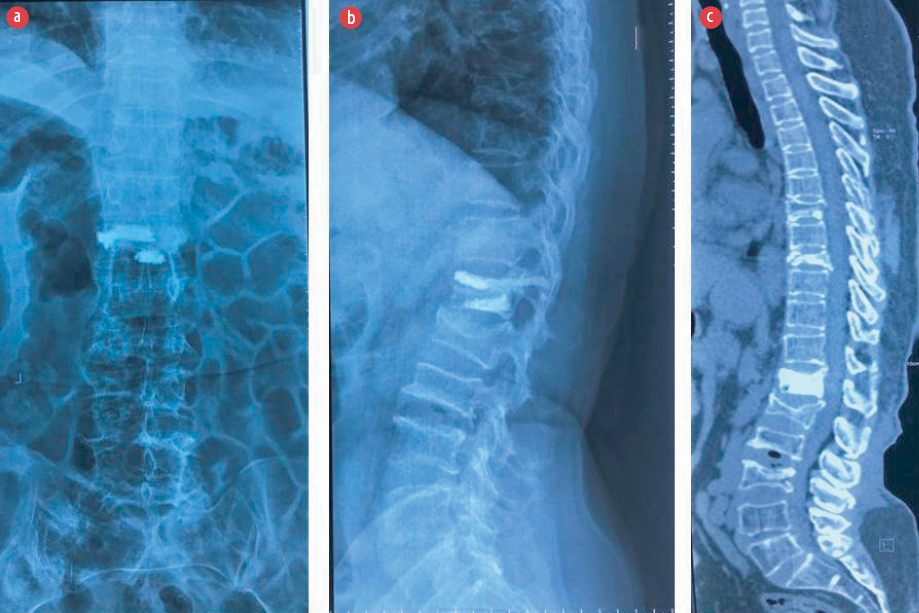 Figure 3: (a and b) Postoperative x-rays, anteroposterior and lateral, showing filling and restoration of height following kyphoplasty. (c) Postoperative CT scan demonstrates cement augmentation with greater clarity.
Figure 3: (a and b) Postoperative x-rays, anteroposterior and lateral, showing filling and restoration of height following kyphoplasty. (c) Postoperative CT scan demonstrates cement augmentation with greater clarity.
Question
What is the diagnosis?
a) Kummell's disease.
b) Scheuermann disease.
c) Apophyseal ring fracture.
d) Bertolotti's syndrome.
Answer
a) Kummell’s disease.
Discussion
Kummell’s disease (KD) is a late-onset vertebral osteonecrosis following a compression fracture. It was first described in 1895 by the German surgeon Herman Kummell.1 This condition may result from failure of the healing mechanism of a fracture resulting in the formation of an avascular zone below the vertebral endplate.2 It may manifest months after a trivial injury in an elderly patient having osteoporosis, in a younger person with chronic steroid use or radiation exposure, or in a known alcoholic.2,3 Patients are often mobile without neurological symptoms but mainly present with chronic and debilitating back pain of > 3 months duration. Plain lateral loading radiographs/dynamic views best illustrate the pseudarthrosis that is optimum for diagnosis.3 The pathognomonic ‘air-filled cleft’ is best demonstrated in CT, though MRI can show a ‘double line sign’ (a region of low intensity surrounded by higher intensity signal.4,5 Management of KD is by eliminating the abnormal motion at the pseudarthrosis site, which relieves pain. Operative management is less successful. Percutaneous vertebral cement augmentation by either KP or vertebroplasty provides radical and immediate pain relief in neurologically intact patients.6 Those who have cord compression features may also need stabilization and posterior decompression in addition to cement filling methods due to low healing potential of the fracture.2 However, these benign lesions must be differentiated from malignant compressive fractures. Malignant vertebral marrow involvement will show higher fractional anisotropy and lower mean diffusivity compared to the benign disease.7 Although contrast-enhanced MRI is helpful in most cases, the FDG-PET/CT is more diagnostic but limited by availability. Recently, diffusion tensor imaging has become the game-changer in segregating the benign from the malignant.
Regarding the other three (incorrect) answer choices, Bertolotti’s syndrome is a condition associated with transition vertebrae either as sacralization of the fifth lumbar vertebra or vice versa.8 Scheuermann kyphosis or Scheuermann disease is a juvenile kyphosis involving the thoracic vertebrae and rarely the lumbar vertebrae in adults with hyperkyphosis, successive three vertebral wedging up to five degrees and discogenic changes.9 Apophyseal ring fractures are rare injuries that mimic common disc herniation (though sometimes they may accompany it).10
Our patient received symptomatic treatment in form of KP along with primary management of osteoporosis. The x-rays/CT scans also show some healed vertebral fractures (no hyperintensity on T2 weighted/ STIR MRI) at multiple levels. These healed fractures are usually ‘silent’(asymptomatic), but can cause local kyphosis and if multiple levels are involved can lead to sagittal imbalance.11
Disclosure
The authors declared no conflicts of interest. Patient consent was obtained for use of radiographic images without disclosing their identity.
references
- 1. Kummell H. Die rarefizierende Ostitis der Wirbelkörper. Deutsche Med. 1895;21:180–181.
- 2. Yu CW, Hsu CY, Shih TT, Chen BB, Fu CJ. Vertebral osteonecrosis: MR imaging findings and related changes on adjacent levels. AJNR Am J Neuroradiol 2007 Jan;28(1):42-47.
- 3. Osterhouse MD, Kettner NW. Delayed posttraumatic vertebral collapse with intravertebral vacuum cleft. J Manipulative Physiol Ther 2002 May;25(4):270-275.
- 4. Ma R, Chow R, Shen FH. Kummell’s disease: delayed post-traumatic osteonecrosis of the vertebral body. Eur Spine J 2010 Jul;19(7):1065-1070.
- 5. Libicher M, Appelt A, Berger I, Baier M, Meeder PJ, Grafe I, et al. The intravertebral vacuum phenomen as specific sign of osteonecrosis in vertebral compression fractures: results from a radiological and histological study. Eur Radiol 2007 Sep;17(9):2248-2252.
- 6. Xiao YP, Bei MJ, Yan CQ, Chang JZ. Analysis of the effect of percutaneous vertebroplasty in the treatment of thoracolumbar Kümmell’s disease with or without bone cement leakage. BMC Musculoskelet Disord 2021 Jan;22(1):10.
- 7. Razek AA, Sherif FM. Diagnostic accuracy of diffusion tensor imaging in differentiating malignant from benign compressed vertebrae. Neuroradiology 2019 Nov;61(11):1291-1296.
- 8. Kumar J, Ali S, Zadran N, Singh M, Ahmed Z. A Rare Case of Bertolotti’s Syndrome in a Young Patient: A Case Report and Literature Review. Cureus 2020 Oct;12(10):e10957.
- 9. Bezalel T, Carmeli E, Been E, Kalichman L. Scheuermann’s disease: current diagnosis and treatment approach. J Back Musculoskelet Rehabil 2014;27(4):383-390.
- 10. Alvarenga JA, Ueta FT, Del Curto D, Ueta RH, Martins DE, Wajchenberg M, et al. Apophyseal ring fracture associated with two levels extruded disc herniation: case report and review of the literature. Einstein (Sao Paulo) 2014 Apr;12(2):230-231.
- 11. Lim J, Choi SW, Youm JY, Kwon HJ, Kim SH, Koh HS. Posttraumatic Delayed Vertebral Collapse : Kummell’s Disease. J Korean Neurosurg Soc 2018 Jan;61(1):1-9.