|
Abstract
Tenosynovial chondromatosis is a very rare disease. The most common symptom is a slowly enlarging soft tissue mass, which may be painful or cause limitation of joint motion. Plain radiograph may appear normal during early phases of the disease, but subsequent imaging may be necessary to exclude other pathologies. Nonoperative treatment may be elected for some patients, but a synovectomy and the removal of loose bodies are indicated for persistent symptoms. This report describe a case with a multinodular cartilaginous proliferation and rice body in the first web space of the hand, similar to synovial chondromatosis, but arising in the tenosynovial membranes.
Keywords: Tenosynovial chondromatosis; Hand; Neoplasm.
Introduction
Tenosynovial chondromatosis is a very rare disease.1 Synovial chondromatosis/osteochondromatosis is an unusual condition that is characterized by cartilaginous and osseous metaplasia in the synovial membranes of large joints, such as the knee or hip joint. By contrast, tenosynovial chondromatosis, which is thought to be the extra-articular counterpart of synovial chondromatosis, has a strong tendency to occur in the fingers and feet.1-3 There are only rare reports in the medical literature of a multinodular extra-articular cartilaginous proliferation involving the tenosynovial membranes.4-8
This report describes a case with multinodular cartilaginous proliferation and rice body in the first web space of the hand, similar to synovial chondromatosis, but arising in the tenosynovial membranes.
Case Report
A 48-year-old woman was admitted because of a mass and pain in the first web space of the hand dorsum, (Fig. 1). There was no history of trauma or rheumatoid disease. She noted that the mass had slowly grown in the last year. She had consulted many physicians, including a rheumatologist and orthopedist and she was diagnosed with a simple ganglion cyst, or tenosynovitis, and treated conservatively. Examination revealed a firm, very tender, 4.0 cm, lobular, soft tissue mass without crepitus in the dorsal aspect of the first web space of the hand. Pain was exaggerated by finger motion. Radiographs showed that the soft tissue mass shadow and the underlying bony cortex were normal and clearly separated from the lesion, (Fig. 2). In the STIR sequence, MRI demonstrated that chondral bodies surround the first web space and second flexor tendon, (Fig. 3).

Figure 1: Mass in the dorsal first web space of the hand.

Figure 2: Radiographs exhibited soft-tissue mass shadow and the underlying bony cortex were normal.

Figure 3: The MRI demonstrates that round separate chondral bodies surround the first web space and second flexor tendon (STIR sequence).
A benign synovial tumor with calcification was considered. The most likely diagnosis was primary synovial osteochondromatosis. Laboratory studies including hemograms and biochemical values were normal, and the patient underwent a debulking procedure. When a surgical exploration of the lesion was performed, numerous shiny soft corpuscles consistent with rice bodies were found in the first web space, extending distally through the sheath to the proximal side of the second finger, (Fig. 4). Histopathologic evaluation showed benign cartilaginous tissue with overlying scant synovial tissue consistent with tenosynovial chondromatosis, (Fig. 5).

Figure 4: Intraoperative photograph showing multiple rice bodies contained within the synovial sheath distally extending.
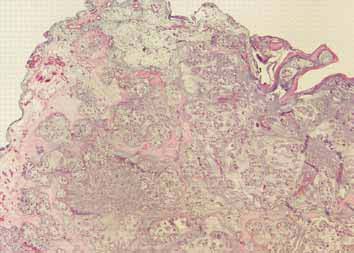
Figure 5: A nodule surrounded by the tenosynovial membrane (HE ×40).
The patient’s postoperative recovery was uneventful and she regained a full and painless range of motion in about two months. At the one-year follow-up, no underlying disorder was evident.
Discussion
Extra-articular tenosynovial chondromatosis is a benign metaplasia of synovial tissue into the cartilaginous tissue but is occasionally a locally aggressive disease.2-4 The primary form of synovial chondromatosis is different from the more common secondary osteochondromatosis that consists of free articular cartilage fragments resulting from either degenerative disease or trauma. Primary synovial osteochondromatosis may arise from either articular synovium or tendon sheath synovium. Males are affected twice as frequently as females and the most common symptom is a slowly enlarging soft tissue mass that may be painful or cause limitation of joint motion. The hands, feet, and wrists are most commonly affected. The involvement of major joints occurs primarily in adults and usually around the knee.2-4,7,8 Radiographically, extra-articular synovial chondromatosis appears as a soft tissue mass with multiple small calcified or ossified densities. Occasionally, there may be only several calcific bodies, which conglomerate to give a lobulated appearance. Routine radiographs are usually adequate for preoperative evaluation. Because of the need for en bloc excision of these locally aggressive lesions, additional studies may be useful to define the extent of the lesion.9 A review of the literature indicates that primary extra-articular synovial chondromatosis of the first web space, as seen in our patient, is exceedingly rare. The disease can also be classified based on the phase of maturation of the lesion. Milgram proposed three phases of the disease in 1977: early, transitional, and late. In early synovial chondromatosis, no loose bodies are present but active synovial disease exists. In the transitional phase, there are both loose bodies and active synovial disease. Finally, in late synovial chondromatosis, there is no longer active synovial disease but loose bodies persist.10 As in this case, patients that present in the transitional phase may have synovitis and pain without any radiographic changes, obscuring the diagnosis. Plain radiographs may appear normal during the early or transitional phase of the disease or show a loose body. Subsequent imaging may be necessary to exclude other pathology. An MRI for diagnosis and differential diagnosis is required.
Conclusion
Nonoperative treatments may be chosen for some patients, but synovectomy and removal of loose bodies is indicated for persistent symptoms. However, the optimal management is surgical exploration and complete excision. Although commonly reported, the risk of recurrence does not interfere with the surgical decision.
Acknowledgements
The authors reported no conflict of interest and no funding was received for this work.
References
1. Roulot E, Le Viet D. Primary synovial osteochondromatosis of the hand and wrist. Report of a series of 21 cases and literature review. Rev Rhum Engl Ed 1999 May;66(5):256-266.
2. Sviland L, Malcolm AJ. Synovial chondromatosis presenting as painless soft tissue mass–a report of 19 cases. Histopathology 1995 Sep;27(3):275-279.
3. Fetsch JF, Vinh TN, Remotti F, Walker EA, Murphey MD, Sweet DE. Tenosynovial (extraarticular) chondromatosis: an analysis of 37 cases of an underrecognized clinicopathologic entity with a strong predilection for the hands and feet and a high local recurrence rate. Am J Surg Pathol 2003 Sep;27(9):1260-1268.
4. Dahlin DC, Salvador AH. Cartilaginous tumors of the soft tissues of the hands and feet. Mayo Clin Proc 1974 Oct;49(10):721-726.
5. Gil-Albarova J, Morales-Andaluz J, Castiella T, Seral F. Tenosynovial chondromatosis of the third finger. Arch Orthop Trauma Surg 2000;120(3-4):239-240.
6. Rompen JC, Ham SJ, Molenaar WM, van Horn JR. Synovial chondromatosis of the wrist and hand–a case report. Acta Orthop Scand 1999 Dec;70(6):627-629.
7. Doumas C, Vazirani RM, Clifford PD, Owens P. Acute calcific periarthritis of the hand and wrist: a series and review of the literature. Emerg Radiol 2007 Sep;14(4):199-203.
8. Murphey MD, Vidal JA, Fanburg-Smith JC, Gajewski DA. Imaging of synovial chondromatosis with radiologic-pathologic correlation. Radiographics 2007 Sep-Oct;27(5):1465-1488.
9. Karlin CA, De Smet AA, Neff J, Lin F, Horton W, Wertzberger JJ. The variable manifestations of extraarticular synovial chondromatosis. AJR Am J Roentgenol 1981 Oct;137(4):731-735.
10. Milgram JW. Synovial osteochondromatosis: a histopathological study of thirty cases. J Bone Joint Surg Am 1977 Sep;59(6):792-801.
|