| |
Abstract
Elongated styloid process causing Eagle's Syndrome is a rare clinical entity and the diagnosis is often difficult as a result of its vague symptomatology. However, palpation of tonsillar fossa with radiological demonstration of the elongated styloid process confirms the diagnosis. This is a report of a retrospective study conducted at the KVG Medical College, Hospital, Sullia, Karnataka, India where 15 patients who were surgically treated for Eagle’s syndrome in the ENT department were retrospectively studied. Fourteen patients became symptom free after surgery within three months of follow up. Tonsillo-styloidectomy is the treatment of choice for Eagle’s syndrome with a high success rate.
Introduction
Eagle's Syndrome is a rare clinical condition, which often presents with recurrent pain in the oropharynx and face, foreign body sensation in the throat, dysphagia and referred otalgia due to an elongated styloid process or calcified stylohyoid ligament.1,2
The styloid process is a slender outgrowth at the base of the temporal bone, immediately posterior to the mastoid apex.3,4 It arises from the inferior surface of the temporal bone at the junction of its petrous and tympanic portions.3,4 It lies caudally, medially, and anteriorly towards the maxillo-vertebro-pharyngeal recess (which contains carotid arteries, internal jugular vein, facial nerve, glossopharyngeal nerve, vagal nerve, and hypoglossal nerve).1,3
With the stylohyoid ligament and the small horn of the hyoid bone, the styloid process forms the stylohyoid apparatus, which arises embryonically from the Reichert cartilage of the second branchial arch.1,3
Eagle defined the length of a normal styloid process at 2.5-3.0 cm.1,2,4 The styloid process may vary from 5 to 50 mm in length and the stylohyoid ligament may ossify from its origin at the styloid process to its attachment at the hyoid bone.5 Moffat,6 described the normal length of styloid process as 1.52-4.77 cm, Kaufman,7 described it as less than 3 cm, Lindeman,8 described it as 2-3 cm, Correl,9 Langlais,10 and Montalbetti11 described it as less than 2.5 cm, while Monsour and Young,12 described it as less than 4 cm and Balcioglu,13 defined it as 40 +/- 4.72 mm.
When the patient presents to the otolaryngologist with symptoms of pain in the throat not consistent with tonsillitis, foreign body sensation, referred otalgia and headache, a differential diagnosis of Eagle’s syndrome should be considered.2,4 Diagnosis is usually made by palpating the tonsillar fossa for an unusually elongated styloid process, (Fig. 1).14-16 The diagnosis is confirmed by soft tissue lateral radiograph of the neck, skull Towne’s view or a computed tomography (CT) scan.14 Approximately 4% of the general population have an elongated styloid process and a calcified stylohyoid ligament, but only a small percent are symptomatic.14,15
Case Report
In this is a case series, of the 15 cases with elongated styloid process with symptoms presenting to the ENT/OPD KVG Medical College, Sullia. KVG Hospital, Sullia is a 750 bedded medical college in South India. The daily ENT 0PD patient input is 60-70. The hospital has a catchment area of 6 towns with nearly one lakh population each. All presented with history of pain and foreign body sensation in the throat. Of these, nine were females and six were males. Examination of the oropharynx revealed a chronic tonsillitis in all the cases. As the pain did not coincide with the clinical symptoms of tonsillitis, palpation of the upper part of both the tonsillar fossa were performed using gloved fingers. A sharp prick or a blunt bony elevation was felt in most of the cases on palpation.
A clinical diagnosis of elongated styloid process was done. X-ray Towne’s view, (Figs. 1, 2) and lateral view of the skull base, as well as the upper neck were done for all cases. The patients were injected with 1 ml of 2% lidocaine into the area and the symptoms subsided on local anaesthesia.14,17,18 CT scan of the skull base was done confirming the diagnosis.

Figure 1: Intra-oral palpation of elongated styloid process.
Figure 2: X-ray Townes view showing elongated styloid process.
The length of the styloid process was measured on CT scan from the skull base to the tip of the styloid process.14 In terms of the length, 30 mm was considered as normal and processes longer than, 30 mm were considered as elongated.3,4 The patients underwent tonsillectomy (dissection snare cautery) under general anaesthesia. After removal of the tonsil, a sharp elongated styloid process was palpated in the tonsillar fossa. The tip of the elongated styloid process was dissected, stripped of all attachments, and nibbled off using a bone nibbler. The procedure was repeated on the other side in cases of bilateral enlarged styloid processes. (Figs. 3,4,5,6)
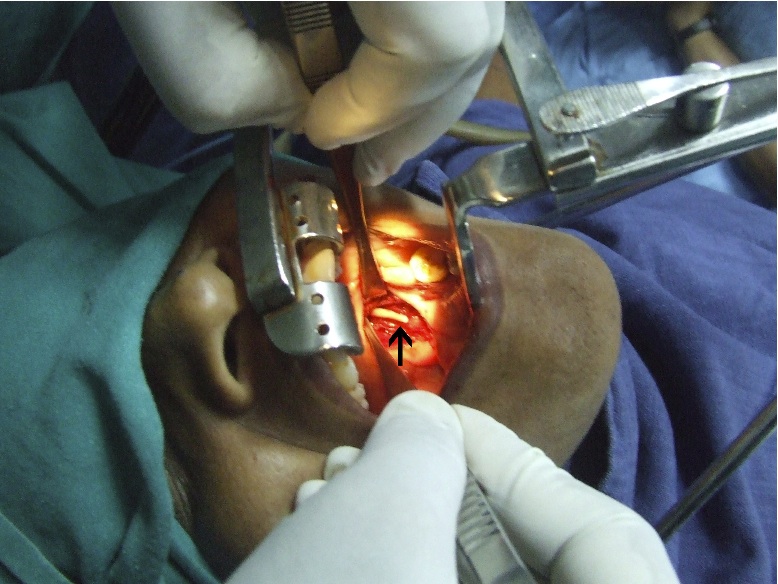
Figure 3: Intra operative photographs showing elongated styloid process in tonsillar fossa.
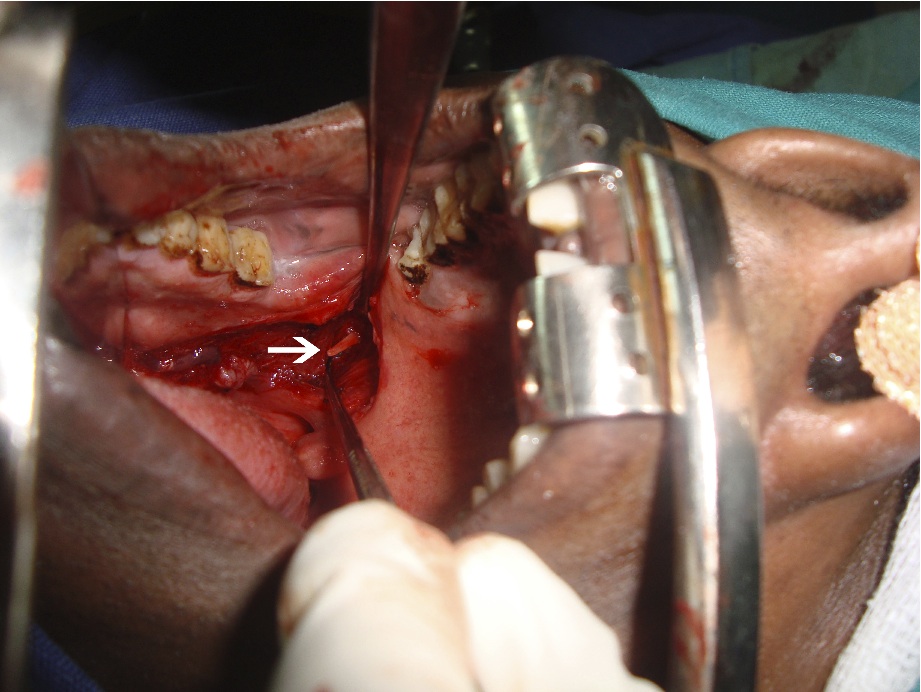
Figure 4: Intra operative photographs showing elongated styloid process in tonsillar fossa.
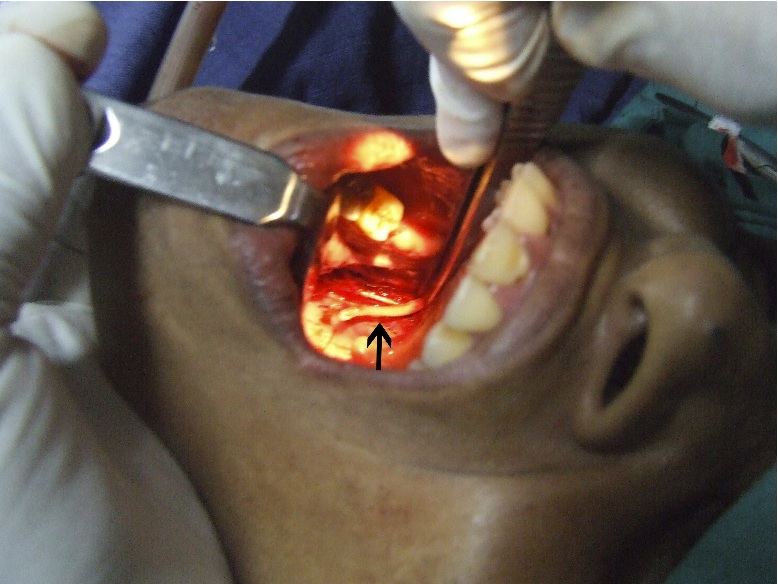
Figure 5: Intra operative photographs showing elongated styloid process in tonsillar fossa.
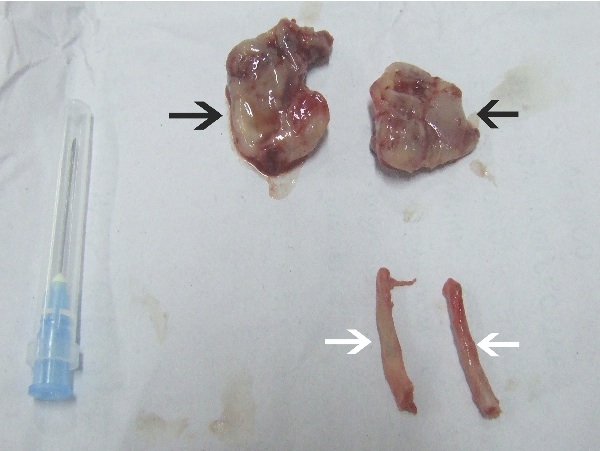
Figure 6: Styloid processes and tonsillar tissue after resection.
All patients were discharged within 4-7 days. All the patients were prescribed oral antibiotics and anti-inflammatory drugs for 7 days at discharge. Four patients belonged to the fourth, six patients to the fifth, 4 patients to the sixth, and one patient to the seventh decade. The youngest patient was of 32 years and the oldest was 62 years. The mean age group was 46.3 years. (Table 1)
The mean duration of symptoms was 7.53 months with main presenting symptom being pain in the throat, foreign body sensation, referred otalgia, headache, carotidynia, dizziness and dysphagia. Other clinical symptoms in literature such as pulsatile tinnitus, palpable neck mass and globus pharyngeus were not reported. In 12 patients, elongated styloid process was bilateral and in three patients, elongation was unilateral.
The patient with 43 mm styloid process had the maximum symptoms, while the patient with 26 mm styloid process had the minimum symptoms. Therefore, according to this report, there is a definite correlation between the length of the elongated styloid process and clinical symptoms. After surgery, nine patients became symptom free in 7 days, three patients in 15 days, two patients in 30 days, but 1 patient had pain even after 1 month of surgery, (Table 2). He was re-evaluated and was treated with oral carbamazepine for one month.
Table 1: Association of clinical features with length of styloid process
| Sl no |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
11 |
12 |
13 |
14 |
15 |
| Length of styloid |
37 |
36 |
43 |
33 |
29 |
26 |
29 |
40 |
31 |
30 |
29 |
31 |
33 |
32 |
33 |
| Age |
46 |
55 |
45 |
56 |
37 |
44 |
62 |
32 |
34 |
47 |
49 |
52 |
44 |
53 |
38 |
| Laterality |
b/l |
u/l |
b/l |
b/l |
b/l |
b/l |
b/l |
u/l |
b/l |
u/l |
b/l |
b/l |
b/l |
b/l |
b/l |
| Sex |
f |
f |
m |
f |
m |
f |
m |
f |
f |
f |
m |
f |
m |
f |
m |
| Duration |
3 |
4 |
6 |
18 |
6 |
12 |
8 |
8 |
14 |
6 |
12 |
4 |
2 |
4 |
6 |
| Pain in throat |
+ |
+ |
+ |
+ |
+
|
+ |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
| Referred otalgia |
- |
- |
- |
- |
+
|
- |
+
|
- |
+
|
+
|
- |
- |
- |
- |
- |
| Foreign body sensation |
+ |
+
|
- |
+
|
+
|
+
|
+
|
- |
+
|
+
|
+
|
- |
+
|
+
|
+
|
| Headache |
+ |
- |
+
|
- |
- |
- |
+
|
- |
- |
+
|
- |
- |
+
|
- |
- |
| Dizziness |
+ |
- |
- |
- |
- |
- |
- |
- |
+
|
- |
- |
- |
- |
+
|
- |
| Pulsatile tinnitus |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
| Dysphagia |
- |
- |
- |
- |
- |
+
|
- |
- |
- |
- |
- |
- |
- |
- |
- |
| Globus phryngeous |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
| Carotidynia |
- |
- |
- |
- |
+
|
- |
- |
+
|
- |
+
|
- |
- |
- |
- |
- |
| Palpable neck |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
Table 2: Follow up of the patients after surgery.
| No of patients |
Follow up in days after discharge |
| 7 days |
15 days |
30 days |
90 days |
| 9 Patients |
Symptom free |
Symptom free |
Symptom free |
Symptom free |
| 3 patients |
Pain & FB sensation present |
Symptom free |
Symptom free |
Symptom free |
| 2 patients |
Pain & FB sensation present |
Pain & FB sensation present |
Symptom free |
Symptom free |
| 1 patient |
Pain & FB sensation present |
Pain & FB sensation present |
Pain & FB sensation present |
Treated with carbamazepine for 3 months |
Discussion
Eagle's Syndrome or Stylalgia caused by elongated styloid process is an uncommon and under diagnosed clinical entity.1,10 Often, it presents with vague pain in the throat, facial pain, referred otalgia and difficulty in swallowing.1,10,19 The first mention of elongated styloid process as a clinical entity in literature was by Lucke and Weinlecher.1,2 Eagle described it as a syndrome complex mainly in two varieties.1,2,4 The classical variety presents as pain in the throat, referred to as otalgia and foreign body sensation in the throat.1,2,4 A second variety is styloid process compressing the carotid artery presenting as carotodynia, headache and dizziness.1,2,4 He found that these patients were relieved of symptoms by shortening the styloid process.1,2,4
Styloid process is part of the temporal bone lying anteromedial to the mastoid process, measuring about 2-3 cm.3,4 Embryologically, it is a derivative of the second branchial arch along with styloid ligament and the lesser cornu of the hyoid bone.3,4 The cause of elongated styloid process is not well understood but several theories have been put forward.3,4 The most popular one is growth of the osseous tissue along stylohyoid ligament.3,4
The clinical symptoms with which the patient presents is due to compression of the adjacent nerves, mainly the glossopharyngeal, lower branch of trigeminal and the chordatympani.14,20 Pain may be due to proliferation of granulation tissue after a traumatic fracture of the styloid process insert into tendinosis or impingement on the carotid vessels.14,20
Pathogenic mechanisms for pain arising from an elongated styloid process usually involve impingement of the pharyngeal mucosa as it is drawn against an elongated process during normal function or impingement of the carotid vessels and their associated sympathetic chain.21 Pain from an elongated styloid process is due to "constant mechanoreceptor discharge in the area of the 5th, 7th, 9th and 10th cranial nerve endings" initiated by a mechanical irritation from the styloid process.21
If a soft tissue lesion at the styloid process results in an inflammatory response, any post-trauma inflammatory edema that may result from such a chronic lesion could create an elevation in intra-compartmental pressure which may affect the neurovascular contents of this space.22,23 Symptoms of styalgia may be due to previous trauma or an inflammatory process that proliferates the granulation tissue, resulting in the calcification or ossification of the stylohyoid ligament.20
Calcification leads to compression of the adjacent structures that are innervated by the glossopharyngeal, trigeminal and chorda tympani nerves.20 There might also be impingement of the plexus of the carotid sheath, which produces irritation of the sympathetic nerves.20
Eagle's Syndrome that follows a tonsillectomy procedure is characterized by symptoms of dysphagia, pain, referred otalgia, dysphagia and foreign body sensation in the pharynx.2,4 Healing tonsillectomy scar tightens the mucosa across the tip of the elongated styloid process.2,4 Upon normal function such as yawning, eating and swallowing, the movements of this mucosa across the styloid process give rise to symptoms.2,4
Diagnosis can be made by plain radiography and CT scan.14,24,25 The length of the styloid process is better demonstrated on lateral views because there is less superimposition.14,24,25 CT scans with coronal images of the upper cervical region provide excellent definition of the complex and adjacent soft tissues, thus it is used to evaluate the length of the stylohyoid complex.26 Axial images provide information about the location and immediate relations of the stylohyoid chain.26 Currently, 3D spiral CT is the most advanced diagnostic imaging technique to evaluate the stylohyoid chain in spatial geometry, with accurate length measurements.26 The detailed information about the course and relations of the stylohyoid chain and the relation of important adjacent anatomic structures also allows pre-operative planning, thereby reducing the potential for iatrogenic intra-operative injury.26,27
Injection of local anaesthetic into the tonsillar fossa relieves pain.14,15,18 Despite the striking radiographic appearance of an ossified and elongated stylohyoid process, the significance of this abnormality has not been appreciated except by otolaryngolists who are familiar with the symptom complex.14
Treatment is mainly surgical, where the elongated styloid process is shortened by trans-tonsillar or by external approach.14,28 Injection of steroid into the lower tonsillar fossa is advised for patients unfit for surgery.14,18
Eagle initially described tonsillo-styloidectomy by the intra- oral route, where a trans-pharyngeal approach was used to extract the styloid process after tonsillectomy.2,4 There is no external scarring with this approach and low post operative morbidity and complications.2,4
Styloidectomy can also be performed by the extra-oral approach through an incision that extends from the mastoid process along the sternocleidomastoid to the level of the hyoid, then up across the neck to the midline of the chin. This approach is aesthetically less pleasing with more morbidity compared to the intra-oral route.14,28,29
Conclusion
Eagle's syndrome associated with elongated styloid process is a rare clinical entity. Clinical palpation of tonsillar fossa was complemented with a plain radiography of skull base Towne’s view, lateral view of the skull base and CT scan to make a diagnosis. The length of the styloid process correlates with the clinical signs and symptoms. Tonsillo-styloidectomy is the treatment of choice in all cases of Eagle’s syndrome and has definitely proven to relieve the patients of styalgia. Awareness of this syndrome is important to all health practitioners involved in the diagnosis and treatment of neck and head pain.
Acknowledgements
The authors reported no conflict of interest and no funding was received for this work.
|
|
| |
1. Eagle WW. Elongated Styloid process. Arch Otolaryngol 1937;25:584-587.
2. Eagle WW. Elongated styloid process; symptoms and treatment. AMA Arch Otolaryngol 1958 Feb;67(2):172-176.
3. Feldman VB. Eagle's syndrome: a case of symptomatic calcification of the stylohyoid ligaments. J Can Chiropr Assoc. 2003;47(1):21-27.
4. Eagle WW. The symptoms, diagnosis and treatment of the elongated styloid process. Am Surg 1962 Jan;28:1-5.
5. Chandler SR. Anatomic variations of the stylohyoid complex and clinical significance Laryngscope 87: 1692-1701, 1977.
6. Moffat DA, Ramsden RT, Shaw HJ. The styloid process syndrome: aetiological factors and surgical management. J Laryngol Otol 1977 Apr;91(4):279-294.
7. Kaufman SM, Elzay RP, Irish EF. Styloid process variation. Radiologic and clinical study. Arch Otolaryngol 1970 May;91(5):460-463.
8. Lindeman P. The elongated styloid process as cause of throat discomfort:4 case reports. J Laryngol 1985;99:505-508.
9. Correll RW, Jensen JL, et al. Mineralization of stylohyoid-stylomandibular ligament complex. Oral surg Oral med Oral path 1979; 48:286–291.
10. Langlais RP, Miles DA, Van Dis ML. Elongated and mineralized stylohyoid ligament complex: a proposed classification and report of a case of Eagle’s syndrome. Oral Surg Oral Med Oral Pathol 1986 May;61(5):527-532.
11. Montalbetti L, Ferrandi D, Pergami P, Savoldi F. Elongated styloid process and Eagle’s syndrome. Cephalalgia 1995 Apr;15(2):80-93.
12. Monsour PA, Young WG. Variability of the styloid process and stylohyoid ligament in panoramic radiographs. Oral Surg Oral Med Oral Pathol 1986 May;61(5):522-526.
13. Balcioglu HA, Kilic C, Akyol M, Ozan H, Kokten G. Length of the styloid process & anatomical implications for Eagle’s syndrome.Folia Morphol. Nov2009; 68:265:70.
14. Murtagh RD, Caracciolo JT, Fernandez G. CT findings associated with Eagle syndrome. AJNR Am J Neuroradiol 2001 Aug;22(7):1401-1402.
15. Rechtweg JS, Wax MK. Eagle’s syndrome: a review. Am J Otolaryngol 1998 Sep-Oct;19(5):316-321.
16. Balasubramanian S. The ossification of styloid ligament and its relation to facial pain. Br Dent J 1964;116:108-111.
17. Baugh RF, Stocks RM. Eagle’s syndrome: a reappraisal. Ear Nose Throat J 1993 May;72(5):341-344.
18. Beech TJ, McDermott A. An Interesting Presentation Of Eagle Syndrome: Internet J Otorhinolaryng. 2006; 5.
19. Gossman JR Jr, Tarsitano JJ. The styloid-stylohyoid syndrome. J Oral Surg 1977 Jul;35(7):555-560.
20. Balbuena L Jr, Hayes D, Ramirez SG, Johnson R. Eagle’s syndrome (elongated styloid process). South Med J 1997 Mar;90(3):331-334.
21. Baddour HM, Anear JT, Tilson AB. Eagles Syndrome, Case report. J Oral Surg 1978;36(6):486.
22. Hilding DA. Fractures of elongated styloid process masquerading as foreign body. Ann Otol Rhinol Laryngol 1961;70:689692.<
23. McGinnis JM Jr. Fracture of an ossified stylohyoid bone. Arch Otolaryngol 1981 Jul;107(7):460.
24. Keur JJ, Campbell JP, McCarthy JF, Ralph WJ. The clinical significance of the elongated styloid process. Oral Surg Oral Med Oral Pathol 1986 Apr;61(4):399-404.
25. Nickel J, Sonnenburg M, Scheufler O, Andresen R. Eagle syndrome: diagnostic imaging and therapy. Rontgenpraxis 2003;55(3):108-113.
26. Alcade RE, Ueyama Y, Nishiyama A, Misugughi T, Matsumura T, Kishi K. Diagnostic imaging of Eagle's syndrome. Oral Radiol 1994;10(2):143-148.
27. Alcade RE, Ueyama Y, Nishiyama A, Misugughi T, Matsumura T, Kishi K. Diagnostic imaging of Eagle's syndrome. Oral Radiol 1994;10(2):143-148.
28. Chase DC, Zarmen A, Bigelow WC, McCoy JM. Eagle’s syndrome: a comparison of intraoral versus extraoral surgical approaches. Oral Surg Oral Med Oral Pathol 1986 Dec;62(6):625-629.
29. Strauss M, Zohar Y, Laurian N. Elongated styloid process syndrome: intraoral versus external approach for styloid surgery. Laryngoscope 1985 Aug;95(8):976-979.
|
|