A 37-year-old man presented to the vascular surgery outpatient clinic at Sultan Qaboos University Hospital for a second opinion following an incidental computed tomography (CT) scan finding that was performed for a work-related promotion. He gave a history of being involved in a motor vehicle collision 18 years prior that required a laparotomy and splenectomy, from which he completely recovered. On presentation, he had no complaints. His physical examination was unremarkable. His CT scan images are shown in Figure 1.
|

|
|
|
|
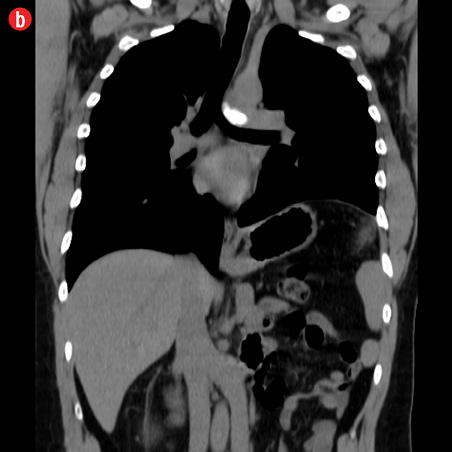
Figure 1: (a) Plain and (b) contrast chest computed tomography images of the patient. |
Questions
1. What is the abnormality on the CT-scan?
2. What is the clinical significance of such a finding?
Answers
1. Inferior Vena Cava (IVC) duplication.
Inferior vena cava (IVC) duplication has an estimated prevalence of 1–3%,1 making it the most frequently encountered IVC anomaly.2 The increased detection rate may be attributed to the wider use of cross-sectional imaging such as CT and magnetic resonance imaging.3 Development of the venous system occurs between four and eight weeks gestation.4 At this point, three pairs of veins contribute to the formation of the IVC (the posterior cardinal, subcardinal, and supracardinal veins).5 These veins normally undergo a complex process of formation and regression, ultimately, giving rise to the different segments of the IVC.6 Abnormalities would result in congenital IVC anomalies.7 Defective regression of the left supracardinal vein leads to formation of a duplicate IVC.8
2. Clinical significance.
The majority of IVC anomalies represent incidental findings in asymptomatic individuals.5 However, it continues to carry prognostic significance to clinicians for accurate identification before any invasive intervention and subsequent avoidance of morbidity associated with inadvertent injury.
IVC anomalies, including duplication, provide technical challenges intraoperatively with surgeries in the retroperitoneum. It can potentially complicate abdominal aortic aneurysm reconstruction and increase its technical difficulty.9 Moreover, it is implicated in urological surgeries such as nephrectomies10 and ureteric surgeries.11 Without prior identification, misidentification as a metastatic retroperitoneal lymph node in testicular cancer may occur, further prolonging and complicating treatment for a presumed recurrence.4
Another implication of IVC duplication lies in IVC filters insertion for prevention of fatal pulmonary embolism (PE). Failure to identify the duplicate IVC with subsequent misplacement of IVC filters may lead to inadequate PE prevention.12
Discussion
The development of the venous system in an embryo takes place in intricate order; any deviation of the normal process results in a myriad of anomalies. IVC duplication remains clinically silent in most individuals. Nevertheless, obtaining knowledge of the anatomy of the retroperitoneal structures is of vital importance before planning any interventions such as aortic surgeries, venous surgeries, IVC filters insertion, urological procedures, retroperitoneal lymph node dissection, and spinal surgeries. Proper identification of such an anomaly will play an important role in reducing morbidity due to inadvertent injury and misidentification for another structure.
Our patient was asymptomatic. Nevertheless, documenting such findings will potentially avoid future complications associated with invasive interventions.
Disclosure
No conflicts of interest, financial or otherwise, were declared by the author.
references
- 1. Zhang L, Yang G, Shen W, Qi S. Spectrum of the inferior vena cava: MDCT findings. Abdom Imaging 2007;32:495-503.
- 2. Artico M, Lorenzini D, Mancini P, Gobbi P, Carloia S, David V. Radiological evidence of anatomical variation of the inferior vena cava: report of two cases. Surg Radiol Anat 2004 Apr;26(2):153-156.
- 3. Bass JE, Redwine MD, Kramer LA, Huynh PT, Harris JH Jr. Spectrum of congenital anomalies of the inferior vena cava: cross-sectional imaging findings. Radiographics 2000 May-Jun;20(3):639-652.
- 4. Hashmi ZA, Smaroff GG. Dual inferior vena cava: two inferior vena cava filters. Ann Thorac Surg 2007 Aug;84(2):661-663.
- 5. Cho BC, Choi HJ, Kang SM, Chang J, Lee SM, Yang DG, et al. Congenital absence of inferior vena cava as a rare cause of pulmonary thromboembolism. Yonsei Med J 2004 Oct;45(5):947-951.
- 6. Saad KR, Saad PF, Amorim CA, Armstrong D, Soares BLF, Neves PCF, et al. Duplication of the inferior vena cava; case report and a literature review of anatomical variation.2012;29(1):60-64.
- 7. Spentzouris G, Zandian A, Cesmebasi A, Kinsella CR, Muhleman M, Mirzayan N, et al. The clinical anatomy of the inferior vena cava: a review of common congenital anomalies and considerations for clinicians. Clin Anat 2014 Nov;27(8):1234-1243.
- 8. Natsis K, Apostolidis S, Noussios G, Papathanasiou E, Kyriazidou A, Vyzas V. Duplication of the inferior vena cava: anatomy, embryology and classification proposal. Anat Sci Int 2010 Mar;85(1):56-60.
- 9. Truty MJ, Bower TC. Congenital anomalies of the inferior vena cava and left renal vein: implications during open abdominal aortic aneurysm reconstruction. Ann Vasc Surg 2007 Mar;21(2):186-197.
- 10. Habuchi T, Okagaki T, Arai K, Miyakawa M. Renal cell carcinoma extending into left side of double inferior vena cava. Urology 1993 Feb;41(2):181-184.
- 11. Shingleton WB, Hutton M, Resnick MI. Duplication of inferior vena cava: its importance in retroperitoneal surgery. Urology 1994 Jan;43(1):113-115.
- 12. Sartori MT, Zampieri P, Andres AL, Prandoni P, Motta R, Miotto D. Double vena cava filter insertion in congenital duplicated inferior vena cava: a case report and literature review. Haematologica 2006 Jun;91(6)(Suppl):ECR30.