It has been suggested that students differ in their learning styles and that learning becomes more effective when the instructional style is in line with students’ learning style.1,2 A learning style or preference is the complex manner in which, and conditions under which, learners most efficiently and most effectively perceive, process, store, and recall what they are attempting to learn.3 The VARK learning style inventory tool, introduced by Fleming,4 defines the preferred mode of learning in terms of four sensory modalities: visual (V), auditory (A), read/write (R), and kinesthetic (K). Briefly, a visual learner prefers the depiction of information in the form of graphs, diagrams and maps, whereas an auditory learner assimilates information better if it is heard/spoken. Similarly, read/write learners prefer accessing information from printed words, while kinesthetic learners prefer to use all their senses and learn theory through its application.5
Preclinical medical students experience substantial stress in the process of adapting to a highly demanding new learning environment.6 It is the teachers’ responsibility to fulfill the learning requirements of the students and promote a positive learning environment.2
We conducted a cross-sectional study to determine the learning preferences of our students using the VARK questionnaire. We hoped that the findings of this study would help us to improve the learning experience of our students by matching our teaching style with their learning preferences.
Methods
Students studying in the preclinical years of their medical degree program at Oman Medical College, Sohar were included in the study. A total of 140 students (122 female and 18 male) consented to participate in the study and answered the VARK inventory tool4 (English version 7.1). The completed questionnaires were scored for each VARK category and the frequency of VARK preferences for each individual component and combination of components was analyzed as per VARK guidelines.4 The data was reported as percentage of respondents in each category of learning preference. The study was approved by the Institutional Review Board.
Results
Of the 140 students, 35% revealed their preference for a single stand-out mode of learning, either visual, auditory, read/write, or kinesthetic. The frequency of their distribution was similar across the four sensory modes (visual (8%), auditory (9%), read/write (9%), or kinesthetic (9%)). These students were labeled uni-modal learners. The remaining 65% preferred using either two (14%), three (19%), or four (32%)modes to assimilate information and were designated multi-modal learners. The majority of these learners used all four modes equally (quad-modal), while the rest preferred using three (tri-modal) or two (bi-modal) modes for acquiring knowledge [Figure 1]. Bi-modal and tri-modal learners preferred six and four possible learning preference combinations, respectively, and the kinesthetic style was preferred for use in combination with other modes [Figure 2].
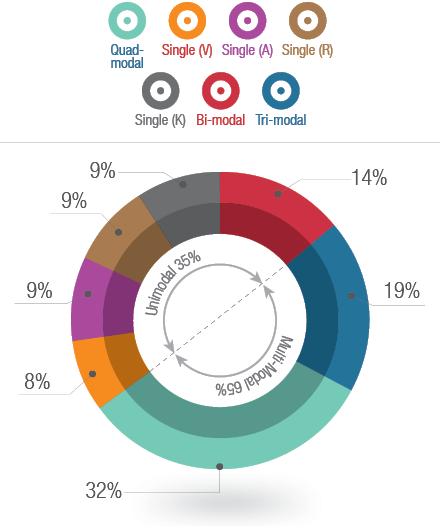
Figure 1: Percentage of uni-modal learners, who preferred a single mode of learning — visual (V), auditory (A), read/write (R), and kinesthetic (K). Percentage of multi-modal learners, who preferred two (bi-modal), three (tri-modal), and four (quad-modal) modes of learning (n=140).
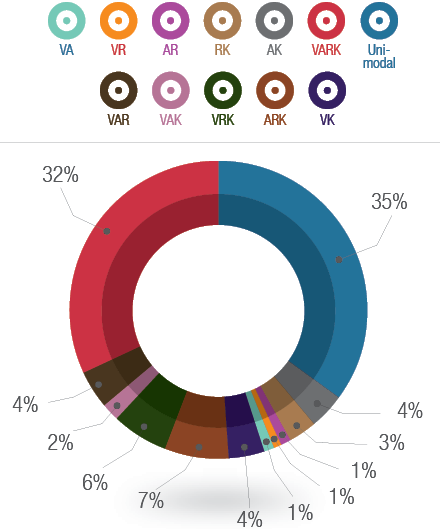
Figure 2: Percentage of students with six combinations of bi-modal, and four combinations of tri-modal learning preferences (n=140).
Key: V= visual, A= auditory, R= read/write, and
K= kinesthetic.
Discussion
Many studies have been done using the VARK questionnaire among preclinical medical students, but the preferred mode of learning was variable in different parts of the world.7 In this study, we administered the VARK questionnaire to preclinical medical students and found that most students (65%) preferred a multi-modal approach to learning, as reported in some previous studies.2,8-11 These students may be either context specific learners, who switch from mode to mode depending on what they are studying, or are not satisfied until they have had their input in all their preferred modes.4 While the uni-modal learners were homogenously distributed across the four VARK categories in our study, other studies find auditory8,10,11 and kinesthetic2,9 to be the most preferred single modes of learning.
Knowledge of students’ learning preferences will help overcome the predisposition of educators to treat all students similarly and can provide a focus for developing strategies that are tailored for individual learners.5 The teaching curriculum of our preclinical medical course predominantly consists of traditional lectures using PowerPoint slides. With this, and the availability of reading material in the library, the auditory and read/write type of learners benefit the most. Few hours are dedicated to laboratory demonstrations, interactive learning activities, and hands on learning which would, to some extent, fulfill the needs of visual and kinesthetic learners. Not all four types of learners are targeted by our current teaching strategy. Thirty-five percent of our students assimilate information only if it is presented in their preferred mode and, if not they are likely to struggle with understanding of the subject material. An equal number of them had preferences for four different modes, compelling us to incorporate necessary measures to address the needs of all four categories of learners evenly.
Active learning strategies reach all types of learners in the VARK schemes and students have better retention and understanding of knowledge when taught by active methods rather than passive methods. The presence of models and demonstrations targets visual learners and discussion during peer instruction, debates, games, and answering questions targets auditory learners. Finally, manipulating models and role playing satisfy kinesthetic learners.2 Co-operative learning exercises, role playing, simulations, models, debates, and games are all examples of active learning strategies that can be used effectively in large classrooms.2 The academic teaching format can be restructured by the addition of strategies that match the learners’ preferences. For example, teachers could reinforce text with colors, graphical depictions, pictures, symbols, and plenty of white space to cater to the visual population and expanded lecture notes, text-enriched PowerPoint slides, and access to library reading material and the internet might satisfy the needs of read/write learners.5 Kinesthetic learners want concrete, multi-sensory personal experiences in their learning so presenting concepts during lectures using suitable clinical case scenarios, analogies, real life examples, and metaphors will benefit kinesthetic learners, as will incorporating videos and movies.5 Teaching with multisensory approaches will also satisfy the need of multi-modal learners, especially those who are not satisfied until they have had input from all their preferred modes.
Knowledge of learning styles could also help teachers identify and solve learning problems among students, and might be valuable for academic underperformers. Students should be encouraged to use their learning preferences to their advantage through practice of appropriate learning strategies. At the same time, students should be motivated to develop the ability to use other learning styles and, hence, widen their repertoire of learning skills.
Conclusion
Using the VARK questionnaire, we learnt that our preclinical medical students differed in their learning preferences. This information encouraged us to accommodate the students’ learning preferences in our lesson plan and incorporate some of the learning strategies suitable for a large classroom setting. It is argued that learning style is not a stable construct and may vary with age and according to the task being undertaken. The correlation between students’ learning preferences and their academic performance is not well established and there remains much debate over the effectiveness of matching learning style and instructional style on students’ academic performance.1,7 These issues will be addressed in an extension of this pilot study that aims to longitudinally assess of the learning style preferences of the same cohort of students during their clinical years.
Disclosure
The authors declared no conflict of interest. No funding was received for this work.
Acknowledgements
VARK © Copyright Version 7.1 (2011) held by Neil D. Fleming, Christchurch, New Zealand.
references
- Robotham D. The application of learning style theory in higher education teaching. Available at: http://www2.glos.ac.uk/gdn/discuss/kolb2.htm. Accessed: February 17, 2014.
- Lujan HL, DiCarlo SE. First-year medical students prefer multiple learning styles. Adv Physiol Educ 2006 Mar;30(1):13-16.
- James W, Gardner D. Learning styles: implications for distance learning. New Dir Adult Contin Educ 1995;67:19-32 .
- Fleming N. VARK: a Guide to Learning Styles. Available at: http://honolulu.hawaii.edu/intranet/committees/FacDevCom/guidebk/teachtip/vark.htm. Accessed: February 18, 2014.
- Fleming ND. I'm different; not dumb. Modes of presentation (VARK) in the tertiary classroom. In: Research and Development in Higher Education, edited by Zelmer A. Proceedings of the1995 Annual Conference of the Higher Education and Research Development Society of Australasia, 1995;18: 308-313.
- Dyrbye LN, Thomas MR, Shanafelt TD. Medical student distress: causes, consequences, and proposed solutions. Mayo Clin Proc 2005 Dec;80(12):1613-1622.
- Khanal L, Shah S, Koirala S. Exploration of preferred learning styles in medical education using VARK modal. Russian Open Medical Journal 2014; 3:0305. Available at: http://www.romj.org/2014-0305. Accessed: November 23, 2014.
- Nuzhat A, Salem RO, Quadri MS, Al-Hamdan N. Learning style preferences of medical students: a single-institute experience from Saudi Arabia. Int J Med Educ (serial online) 2011; 2:70-73. Available at: http://www.ijme.net/archive/2/students-learning-style-preferences.pdf. Accessed: February 25, 2014.
- Choudhary R, Dullo P. Gender differences in learning style preferences of first year medical students. Pak J Physiol 2011;7:42-45.
- Samarakoon L, Fernando T, Rodrigo C. Learning styles and approaches to learning among medical undergraduates and postgraduates. BMC Med Educ 2013; 13: 42. Available at: http://www.biomedcentral.com/1472-6920/13/42. Accessed: February 17, 2014.
- Urval RP, Kamath A, Ullal S, Shenoy AK, Shenoy N, Udupa LA. Assessment of learning styles of undergraduate medical students using the VARK questionnaire and the influence of sex and academic performance. Adv Physiol Educ 2014 Sep;38(3):216-220.