| |
Abstract
Objective: To evaluate the effect of mode of delivery on postpartum sexual functioning in primiparous women.
Methods: In this cross-sectional descriptive study, 150 primiparous women in postpartum period, who attended the family planning or vaccination clinics, were enrolled for the study. Eighty-one had vaginal delivery with episiotomy and 69 had experienced cesarean section. Sexual function was evaluated by the Female Sexual Function Index within 3 and 6 months postpartum.
Results: About 29% in vaginal delivery group and 37% in cesarean delivery group had resumed their sexual intercourses four weeks after delivery (p=0.280).There were no significant differences between mode of delivery and sexual functioning, including desire, arousal, lubrication, orgasm, satisfaction and pain.
Conclusion: The present study showed that postpartum sexual functioning was not associated with the type of delivery.
Keywords: Postpartum; Vaginal delivery; Cesarean section; Sexual functioning.
Introduction
Childbirth affects the body, especially the female genitalia; these changes trouble women in the resumption of sexual intercourses. Many women in postpartum suffer from problems such as: dyspareunia, loss of desire, loss of vaginal lubrication, pain on orgasm, post coital bleeding, itching and burning.1-3 It is estimated that 20% of women have dyspareunia in their first three months of postpartum in a way that the pain persisted in one woman out of five until 6 months after delivery and one ninth could not ever resume sexual intercourse.4 In a study in Iran, the prevalence of Physical-sexual problems after childbirth reported about 78%.5 Type of delivery and perineal trauma during childbirth is associated with sexual problems after childbirth and this pain in primiparous women in the first three months after birth is about 80%.2,6 Because cesarean delivery prevents damage to the perineum, it is thought that this may prevent the occurrence of sexual dysfunction after delivery.2 This is a major reason why some women even Obstetricians and Gynecologists choose cesarean delivery in some countries though there is no scientific data to support this opinions.2,7 Also, some studies have shown that the average score for sexual function after childbirth in women who have had a cesarean delivery is much better than women who have vaginal delivery with episiotomy.8,9 In Iran the cesarean rate has exceeded international standards and in some areas even up to 45% is reached, one reasons is the fear of vaginal and perineal injury.10 Sometimes sexual changes after childbirth cause substantial disruption in the relationship between spouses and only 15% of women who suffer from sexual dysfunction problems consult with health care providers.11 Hence awareness of such problems for health care providers can solve many problems in this field. In this study, by comparing sexual function in primiparous women who delivered vaginally with episiotomy or elective cesarean delivery, we tried to determine whether type of delivery could affect the incidence of sexual dysfunction in postpartum period.
Methods
This study was a cross-sectional descriptive study. The study was approved by the Ethics Committee of Hormozgan University of Medical Sciences (HUMS), Iran. After approval, we used the Female Sexual Function Index (FSFI) developed by Rosen et al. (2000).12 This questionnaire is brief, self- reported, multidimensional and has 19 items for the assessment of key dimensions of sexual function (desire, arousal, lubrication, orgasm, satisfaction and pain) in women. The FSFI provides scores on six domains and each domain is scored on a scale of 0-6, that higher scores means better sexual function. A domain score of zero indicated that the women did not have sexual intercourse during the last month and full score range was from 2.0 to 36.0. We selected primiparous women to avoid the confounding effect of a previous birth. Informed consent was taken before the study. Primiparous women who had brought their babies for vaccination or who attended the family planning clinics at the health and teaching clinics in Bandar Abbas from September 2010 to April 2011, were enrolled in this study. Subjects were asked to complete the questionnaire by themselves three and six months after delivery. Information about each woman (e.g., demographic characteristic, the time of resuming sexual intercourse after delivery and type of delivery) was recorded. The inclusion criteria were: primiparous women after a term singleton delivery, married and living with the husband, having at least five years of elementary education. Women who had preterm birth, cesarean section after labor begun, assisted vaginal delivery, extended episiotomy, birth weight more than 4000 gr, infant with any anomalies, any history of systematic disease (e.g., preeclampsia, diabetes mellitus), depression or postpartum depression and sexual dysfunction prior pregnancy were excluded. Then samples were divided into two groups of elective cesarean section and vaginal delivery with mediolateral episiotomy.
Statistical evaluation was carried out by SPSS for windows v.16. Independent samples of t test for equality of means and covariance used for comparison between groups and paired t test used for comparison within groups. Statistical significance was attained with a p-value <0.050.
Results
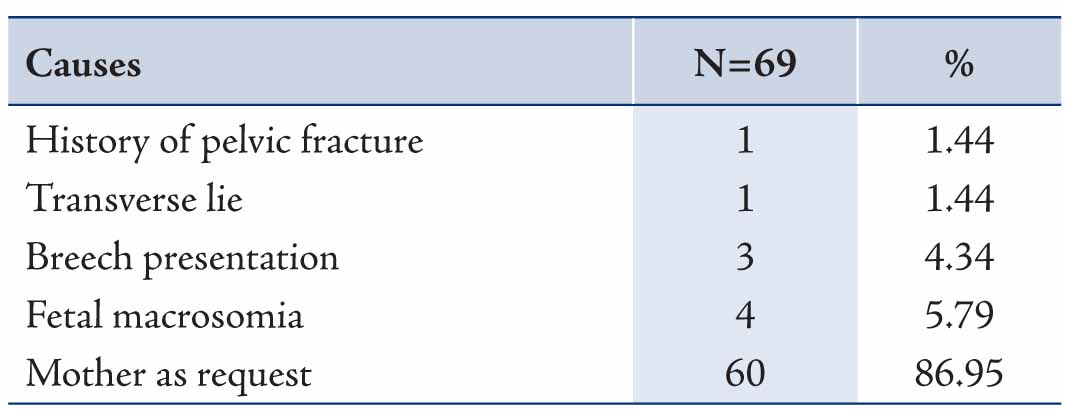
One hundred fifty women completed the FSFI questionnaire. Cesarean section accounted for 46% of all deliveries (n=69), the causes of elective cesarean are shown in Table 1. The demographic characteristics of the groups are shown in Table 2. There was no difference between the groups with regard to demographic characteristics. 24 cases (30%) in vaginal delivery group and 26 cases (38%) in cesarean delivery group had resumed their sexual intercourse one month after delivery and 55 cases (68%) in vaginal delivery group and 41 cases (59%) in cesarean delivery group had resumed their sexual intercourse two month after delivery and 2 cases in each group up to six months postpartum had not sexual intercourse and no statistically significant difference was observed between the two groups (p=0.280).
Table 1: Causes of elective cesarean.
The FSFI scores of both groups and the comparison between the two groups are given in Table 2. The comparison between three and six month’s postpartum scores for the vaginal delivery with mediolateral episiotomy group showed a significant increase in the desire and arousal scores at six months postpartum. In the cesarean section group, comparison between three and six month’s postpartum scores shows significant increase in all dimension of sexual function except satisfaction at six months postpartum. There was no statistically significant difference of female sexual function between two groups as it is shown in Table 3.
Table 2: Comparison of Demographic Characteristics among two Groups.
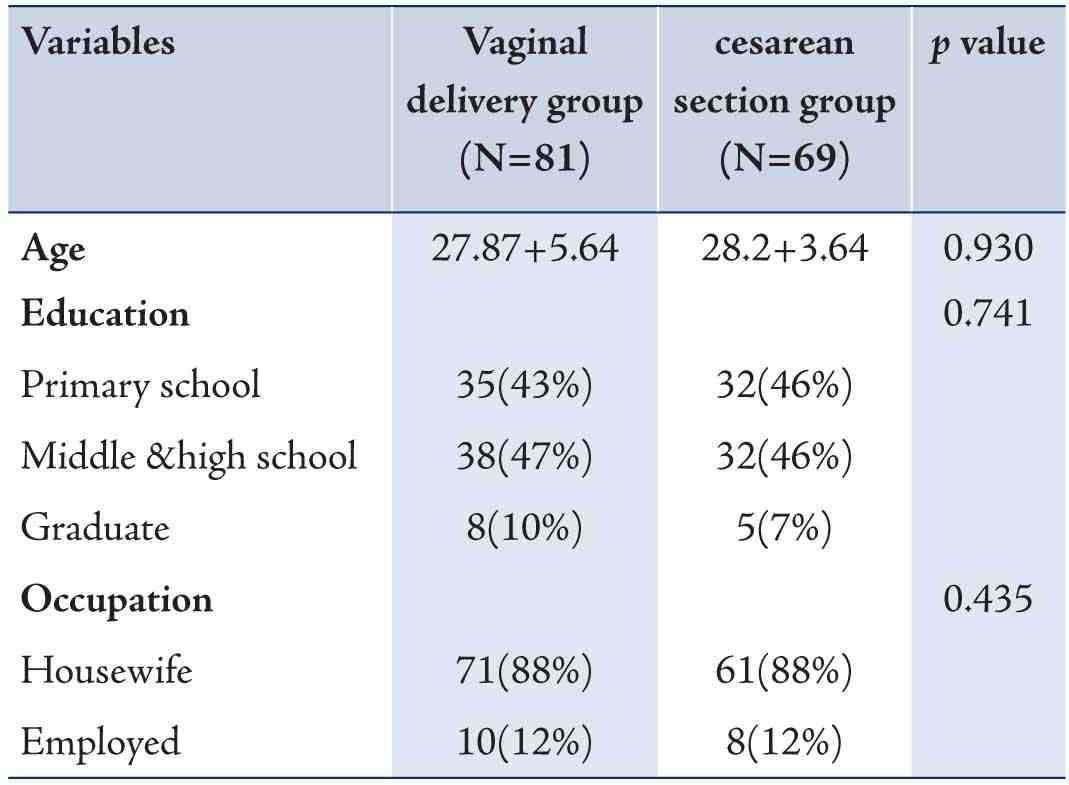
Table 3: Comparison of FSFI scores in two groups.
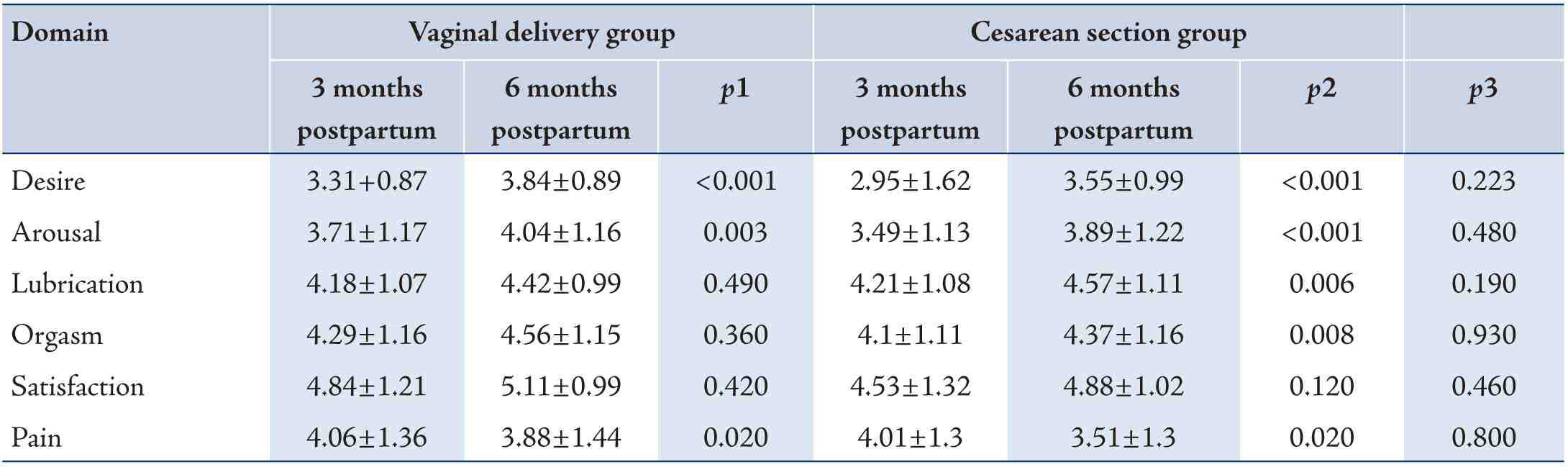
1. Comparison between 3months and 6months scores in the vaginal delivery group
Discussion
There are many factors that affect sexual function in women and pregnancy and childbirth is one of these factors. It has been reported that prevalence of short-term sexual problems in the postpartum period is about 22-86%.13 Time of resumption of sexual intercourse after delivery in women is different. In this study, we evaluated the impact of childbirth on women’s sexual function, each of up to 6 months after delivery because we expected, the majority of them has resumed their sexual intercourse up to 6 to this time. About 29% in vaginal delivery group and 37% in cesarean delivery group had resumed their sexual intercourse four weeks after delivery. These findings are similar to previous studies that about 90% of postpartum women had resumed their sexual intercourse by 3-4 months after delivery.2,11,13 Time of resumption of sexual intercourse after delivery depends on degree of perineal injuries, breast feeding, maternal age, race and nationality. Breast feeding seems to be associated with dyspareunia (because of vaginal dryness) or loss of desire. In our study all of subjects had breast feeding so its effect on sexual function is similar. Pain in genital area is one of the important factors that affect resumption of sexual intercourse after delivery. In a study, intensity of dyspareunia was associated with intensity perineal tear and damage.6 In our study, the average score of pain domain in both groups was reduced at 6 months postpartum than 3 months postpartum, which indicates that with more time of delivery reduced intensity of dysparenuia. However, between the two groups the average score of dyspareunia did not differ 3 and 6 months postpartum; this means that type of delivery does not affect the severity of dyspareunia after delivery. But, Safarinejad et al. reported the most intensity dyspareunia in instrumental delivery and the lowest intensity in elective cesarean delivery.14 Signorello et al. reported that at 3 months postpartum dyspareunia was related to degree of perineal damage but at 6 months postpartum most cases of dyspareunia were breast feeding and instrumental delivery.6 Hartmann et al. conducted a systematic review to evaluate the outcome of vaginal delivery with episiotomy, found that dyspareunia was more common among women with episiotomy.15 The data on type of delivery and postpartum sexuality are inconsistent. Woranitat and Taneepanichskul and Hicks et al. reported no statistically significant difference between type of delivery and sexual function.16,17 Hosseni et al. followed the women for two years after childbirth and showed that there was no difference between mode of delivery and sexual function.18 Botros et al. evaluated the effect of parity on sexual function and found that decreased sexual desire and excitement significantly affected by previous delivery and type of delivery (vaginal or cesarean section) had no obvious role.11 These findings are similar to our study. On the other hand Basksuet al. showed that vaginal delivery with episiotomy decreases level of all domains except pain at 6 months postpartum compared to elective cesarean section.8 Dean et al. followed the women for six years after childbirth and reported that sexual satisfaction and vaginal muscle tone were significantly lower in the women with normal delivery comparing the cesarean section.19 Safarinejad et al. showed that women with vaginal delivery and emergency cesarean section had lower FSFI scores comparing the elective cesarean section.14 Gungor et al. showed that vaginal delivery had a trend toward higher prevalence of dissatisfaction than cesarean delivery.1 Barrett et al. showed that any protective effects of cesarean section on sexual function was limited to the early postpartum period (0-3 months) and the difference in dysfunction levels are reduced after 6 months.2 But Mousavi et al. evaluated the quality of life after delivery and found that women with vaginal delivery were more satisfied with their sexual lives and bodily appearance in the postpartum period.20 These differences with our study could be due to study design, sample size or demographic differences. We did not evaluate the using of contraceptive methods by women in the present study, which some of these methods might be affected sexual function and this is the limitation of our study.
Since sexual problems between couples is an important factor in creating a sense of joy and satisfaction and effects on their quality of life, and it can even affect her disagreement with her maternal status, should be more emphasis on role of sexual counseling postpartum visit. In the present study sexual functioning was not associated with the type of delivery. The findings from our study is going along from most of the relevant articles published in this subject and no bases to advocate cesarean section for delivery in order to preserve sexual function. Some women due to fear of vaginal delivery, are requesting elective cesarean section and one of the causes of fear of vaginal delivery is fear of sexual problems after childbirth that this increases the rate of repeat cesarean section and maternal and fetal morbidity. Given the relatively high rate of elective cesarean section in this study (46%) and women’s fear of genital injury during vaginal delivery, healthcare provider can reduce the fear of vaginal delivery with consultation in prenatal visits.
Conclusion
There was no significant difference between the mode of delivery and sexual function. Therefore, it can be proposed that vaginal delivery has little impact on the sexual functioning after delivery. So in order to preserve sexual function after postpartum, elective cesarean section is ineffective and not recommended.
Acknowledgements
The authors reported no conflict of interest and no funding was received on this work.
References
1. Gungor S, Baser I, Ceyhan S, Karasahin E, Acikel CH. Mode of delivery and subsequent long-term sexual function of primiparous women. Int J Impot Res 2007 Jul-Aug;19(4):358-365.
2. Barrett G, Peacock J, Victor CR, Manyonda I. Cesarean section and postnatal sexual health. Birth 2005 Dec;32(4):306-311.
3. Odar E, Wandabwa J, Kiondo P. Sexual practices of women within six months of childbirth in Mulago hospital, Uganda. Afr Health Sci 2003 Dec;3(3):117-123.
4. Brubaker L, Handa VL, Bradly CS, Connoly AM, Moalli P, Brown MB, et al; Sexual function 6 months after first delivery. Obstet Gynecol 2008 May; 111(5):1040-4.
5. Nourouzi M, Bashardoust N.A. Farmahini faraahain M. Postpartum physico ـ sexual problems and related factors. Shahrekord University of Medical Sciences Journal 2005;7(3):28-32. Persian but abstract is available in English.
6. Signorello LB, Harlow BL, Chekos AK, Repke JT. Postpartum sexual functioning and its relationship to perineal trauma: a retrospective cohort study of primiparous women. Am J Obstet Gynecol 2001 Apr;184(5):881-888, discussion 888-890.
7. Groom KM, Paterson-Brown S, Fisk NM. Temporal and geographical variation in UK obstetricians’ personal preference regarding mode of delivery. Eur J Obstet Gynecol Reprod Biol 2002 Jan;100(2):185-188.
8. Baksu B, Davas I, Agar E, Akyol A, Varolan A. The effect of mode of delivery on
9. Baksu B, Davas I, Agar E, Akyol A, Varolan A. The effect of mode of delivery on postpartum sexual functioning in primiparous women. Int Urogynecol J Pelvic Floor Dysfunct 2007 Apr;18(4):401-406.
10. Saurel-Cubizolles MJ, Romito P, Lelong N, Ancel PY. Women’s health after childbirth: a longitudinal study in France and Italy. BJOG 2000 Oct;107(10):1202-1209.
11. Mohammadpoour Asl A. Rostami F, Torabi S.SH. Prevalence of cesarean section and its demographic correlates in Tabriz. Medical Journal of Tabriz University of Medical Sciences 2006 fall 6; 28(3); 101-105. (Persian but abstract is available in English)
12. Botros SM, Abramov Y, Miller JJ, Sand PK, Gandhi S, Nickolov A, et al. Effect of parity on sexual function: an identical twin study. Obstet Gynecol 2006 Apr;107(4):765-770.
13. Rosen R, Brown C, Heiman J, Leiblum S, Meston C, Shabsigh R, et al. The Female Sexual Function Index (FSFI): a multidimensional self-report instrument for the assessment of female sexual function. J Sex Marital Ther 2000 Apr-Jun;26(2):191-208.
14. Safarinejad MR, Kolahi AA, Hosseini L. The effect of the mode of delivery on the quality of life, sexual function, and sexual satisfaction in primiparous women and their husbands. J Sex Med 2009 Jun;6(6):1645-1667.
15. Hartmann K, Viswanathan M, Palmieri R, Gartlehner G, Thorp J Jr, Lohr KN. Outcomes of routine episiotomy: a systematic review. JAMA 2005 May;293(17):2141-2148.
16. Hicks TL, Goodall SF, Quattrone EM, Lydon-Rochelle MT. Postpartum sexual functioning and method of delivery: summary of the evidence. J Midwifery Womens Health 2004 Sep-Oct;49(5):430-436.
17. Woranitat W, Taneepanichskul S. Sexual function during the postpartum period. J Med Assoc Thai 2007 Sep;90(9):1744-1748.
18. Hosseini L Iran-Pour E, Safarinejad MR. Sexual function of primiparous women after elective cesarean section and normal vaginal delivery. Urology Journal 2012 spring; 9(2):498-504.
19. Dean N, Wilson D, Herbison P, Glazener C, Aung T, Macarthur C. Sexual function, delivery mode history, pelvic floor muscle exercises and incontinence: a cross-sectional study six years post-partum. Aust N Z J Obstet Gynaecol 2008 Jun;48(3):302-311.
20. Mousavi SA, Mortazavi F, Chaman R, Khosravi A. Quality of life after cesarean and vaginal delivery. Oman Med J 2013 Jul;28(4):245-251.
|