|
Abstract
Objective: The aim of this study was to explore the physicians' perspectives and practices in relation to breaking bad news (BBN) to patients.
Methods: A quantitative survey was performed in the Qassim Region from January to July 2011. A cross-sectional study was conducted using a questionnaire administered to all practicing physicians working in both hospitals and Primary Healthcare centers in the Qassim Region. Anonymity was maintained throughout. The target groups received a self-administered questionnaire with a covering letter introducing the study and explaining their rights.
Results: A total of 458 physicians participated in the study. Physicians with higher qualifications had lower total scores of the mean in BBN skills. The majority (70%) preferred to discuss information with close relatives rather than the patients. In case of serious diseases, only 32% said that they would inform the patient’s family without the patient’s consent. More than 90% of our study sample did not avoid telling their patients the bad news; however, physicians working in Primary Healthcare centers were less reserved.
Conclusion: Although most of the participating physicians were keen to help their patients, they lacked the essential knowledge and skills for breaking bad news. Thus, they are in need of specific training in this regard.
Keywords: Physician-patient communication; Breaking bad news; Saudi Arabia.
Introduction
The growth of the "patient-centered" approach to healthcare has highlighted the importance of quality communication practices. An area that still remains problematic; however, it is the process of breaking bad news (BBN) either to patients and/or relatives, which calls for more research and training in this domain.1 Patients expect to meaningfully participate in the decision making process when they visit doctors for consultation about their health. Achieving this requires a sea of change in the doctor patient relationship. In its traditional form, the doctor dominates decision making without much regard to the patient’s feelings. However, a patient oriented approach demands a more informed, shared and negotiated transaction in which the patient can exchange information with health-related staff and actively participates in the decision making process.2 All health systems aim to achieve maximum patient satisfaction. Evidence shows that a patient-centered health consultation results in greater patient satisfaction, which amply emphasizes the fact that communication is a core clinical skill that forms an essential part of clinical competence.3
The common denominator in the bad news is a message, which has the potential to shatter hopes and dreams leading to very different lifestyles and futures. Examples include: a) A patient who is told they are HIV positive; b) The man who is told his partner has Alzheimer's disease; c) The patient who is told the lump has been diagnosed as cancer; and d) The couple who are told they cannot have children.4
In the eighties, a study was conducted in Riyadh, Saudi Arabia showing that only 16% of the cancer patients and 69% of the companions of patients were informed by the physician in charge about the nature of the illness prior to referring the patients to the oncologist. The study observed that "the question in the Eastern as opposed to the Western world is "whether" rather than "how" to inform the patient".5 Another study conducted in three large cities in Saudi Arabia showed that only 47% of the physicians indicated that they provided information on the diagnosis and prognosis of serious diseases and most physicians (75%) preferred to talk with close family members.6
There is now ample evidence that patients cope better with serious illnesses if they are kept informed. Many cancer patients in Saudi Arabia remain unaware about the extent and prognosis of their disease.7 Another survey in Saudi Arabia has shown that in the case of patients with incurable cancer, 67% of doctors indicated that they would inform the patient rather than the family of the diagnosis.8 Also, 99% of patients preferred knowing all about their disease and 100% rejected withholding information.9,10
In the Western culture the rights of individuals are considered paramount and are reflected in the patient autonomy models. Following this model, bad news is communicated directly and honestly to the patient, who is then able to choose whether or not to be actively involved in all aspects of decision-making about the management of their illness.11 Based on the autonomy model, guidelines for breaking bad news were developed by Rabow and McPhee,12 and later adapted by VandeKieft.13 Common features in these guidelines are a truthful explanation of a diagnosis with a poor prognosis, providing time to the patient to respond, and then offering support.
Studies in Western countries show that truth telling - centered strategies are supported by evidence of benefits in many aspects like quality of life.14 Which is different from many other societies with high levels of family involvement who are opposed to diagnosis disclosure such as Spain, Greece, China, Singapore, Japan, Saudi Arabia and Korean-Americans and even Mexican-Americans in the USA?15 But doctors in the Saudi Community sometimes find themselves unable to disclose full information to cancer patients about their disease. This is usually because of family wishes and some other factors.16
However, some authors have reported that disparity between opinions of physicians about truthful disclosure, the stress experienced while breaking bad news and the need for more training is notable.17 In addition, requests for nondisclosure are not rare. But they cause considerable distress to physicians who are used to an autonomy-focused approach to clinical decision making, which is after all, the goal. It is the patient and not the physician or the family who ultimately has the right to decide how they want to exercise autonomy about their own illness.18
In general, studies have shown that most of the the patients' complaints about doctors are related to issues of communication rather than clinical competency. Patients would like doctors who can diagnose and treat their illnesses as well as communicate with them effectively.19 In the West, a recognition that doctors may require further training to help them improve their communication skills, has led to the development of countless training courses and workshops on "how to break bad news" for undergraduates and postgraduates physicians. Most of the participants in these studies reported that the training courses were helpful. However, there is little empirical data to show that these courses lead to improvements that successfully translate into practice or that any measurable improvements are achieved over time.17 The aim of this study therefore, is to explore physicians' perspectives and their practices in relation to BBN to patients.
Methods
A cross-sectional study was conducted in the Qassim Region from January to July 2011. A self-administered questionnaire was designed to elicit information on physicians’ knowledge and practices about breaking bad news to patients and their families. The questionnaire was sent to all practicing physicians working in public hospitals and primary healthcare (PHC) centers in the Qassim Region. We sent the questionnaires to hospital directors and administrators/supervisors of PHC centers, with the request to pass them on to the eligible respondents. Physicians not directly in contact with patients, for instance, forensic and public health physicians etc., were excluded from the study. Anonymity was maintained throughout. The respondents received a short and simple self-administered questionnaire in English, with a covering letter explaining the project and stating their rights as respondents to the survey.
We also provided a working definition of ‘bad news’ as "any information which adversely and seriously affects an individual's view of his or her future (in the context of a patient suffering from a grave disease)".20 The questionnaire also elicited information on the manner in which the bad news was transmitted; for example, an important step of breaking bad news is a ‘warning shot’ which is considered as an effective way of reducing the element of shock.21 In other words, it is a statement used to alert the recipient to the seriousness of what is about to be said.22
The questionnaire consisted of two sections. The first section asked physicians to give personal details including age, gender, clinical position, specialty, qualifications, year of graduation, and work setting. The second section was related to their opinions and practices about breaking bad news which consisted of 25 items. Each item was measured on a 5-point Likert scale ranging from strongly agree, agree, no difference, disagree, and strongly disagree. The items were based on the main steps of breaking bad news especially SPIKES model.12,13,20,22,23
All items were verified and subjected to content validation by three major experts in communication skills. They were given copies of the questionnaire, as well as the purpose and objectives of the study. They evaluated the questionnaire on an individual basis. Comparisons were made between these evaluations and the questionnaire was slightly amended. The questionnaire was pretested on a small sample and modifications were made accordingly.
Likert scale was used to explore physicians’ opinions and practices. A typical test item in this scale is a statement, the respondent is asked to indicate their degree of agreement with the statement. A five-point scale was used here.24 All questionnaires were coded and entered into an electronic database. For the purpose of analysis, the total score was computed as follows: strongly agree +2; agree +1; no difference 0; disagree –1; strongly disagree –2. Negative statements were re-coded using Statistical Package for Social Sciences (SPSS) to be treated in a similar way. Data analysis was carried out using SPSS version 12. Frequency distributions with numbers and percentages of all variables were produced.
The study proposal was scrutinized and approved by the Medical Research Center of Qassim College of Medicine. An anonymous self-administered questionnaire was used and raw data were treated with strict confidentiality, and used only for research purposes.
Results
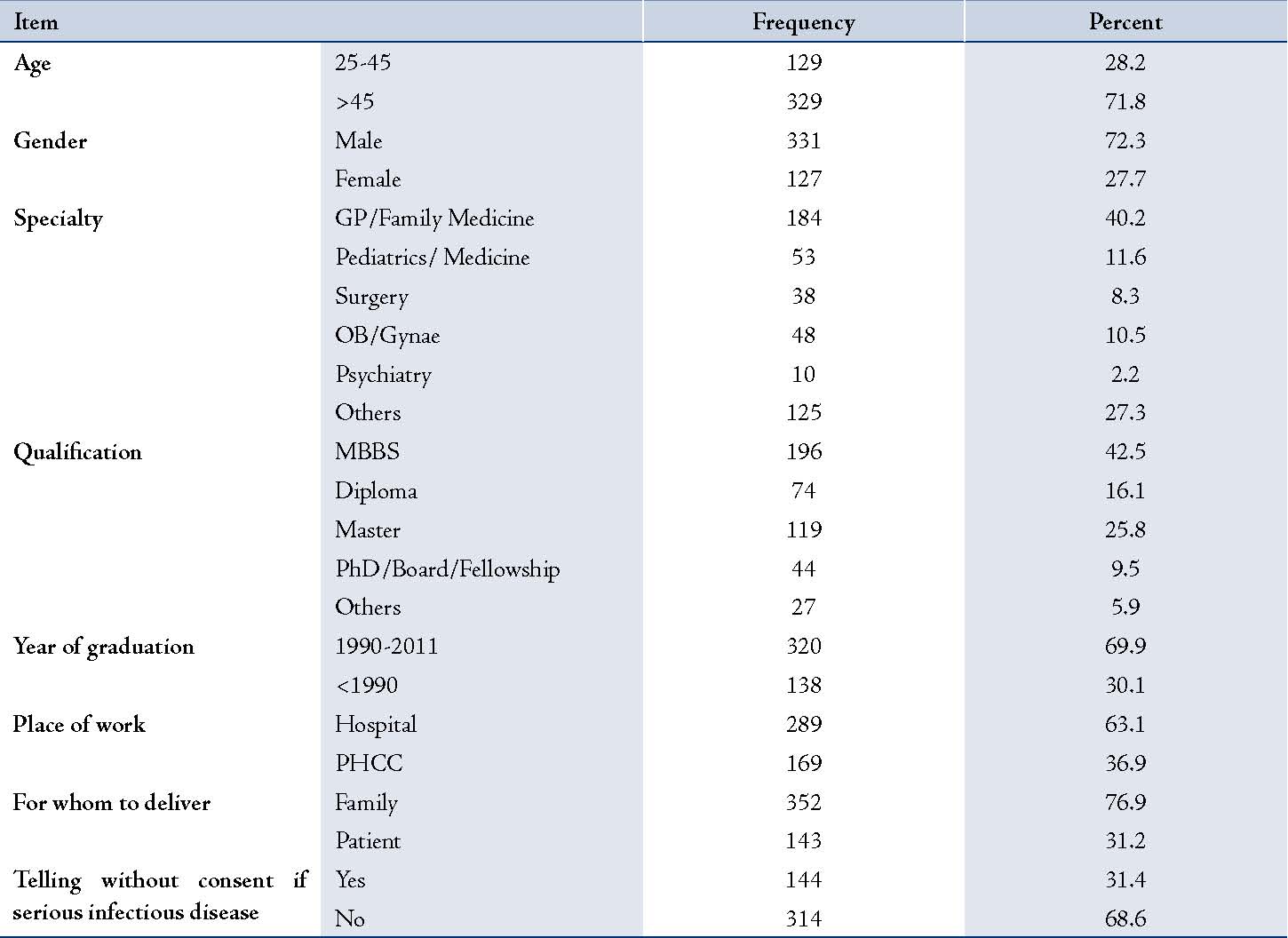
There were a total of 1,546 practicing physicians working in public health facilities in the Qassim region. The questionnaires with covering letters were sent to them all through their supervisors/administrators. However, only 458 completely filled questionnaires were returned (30% response rate). The primary reason for non-response was not the refusal to participate in the study, but that the respondents did not receive the questionnaire in the first place. Out of those who did receive the questionnaire, approximately 45% responded. For the purpose of this study however, we consider the response rate to be 30%. This was a cause for concern and we compared the profiles of our respondents with that of the non-respondents (Table 1). Information about the non-respondents was available through the Ministry of Health. There were significant differences between respondents and non-respondents with regards to all the variables except gender. Respondents were more likely to be working in PHC center, have no postgraduate qualification and working as general or family practitioners.
Table 1: Characteristics of the respondents.
The total score of the mean indicates that the junior physicians with lower qualifications have a better total score than the highly qualified. Other variables (gender, specialty, age, and year of qualification) did not show any significant difference (Table 2). On the other hand, the results suggest that younger physicians do not hesitate delivering bad news in a multi-bed hospital room. (Table 3)
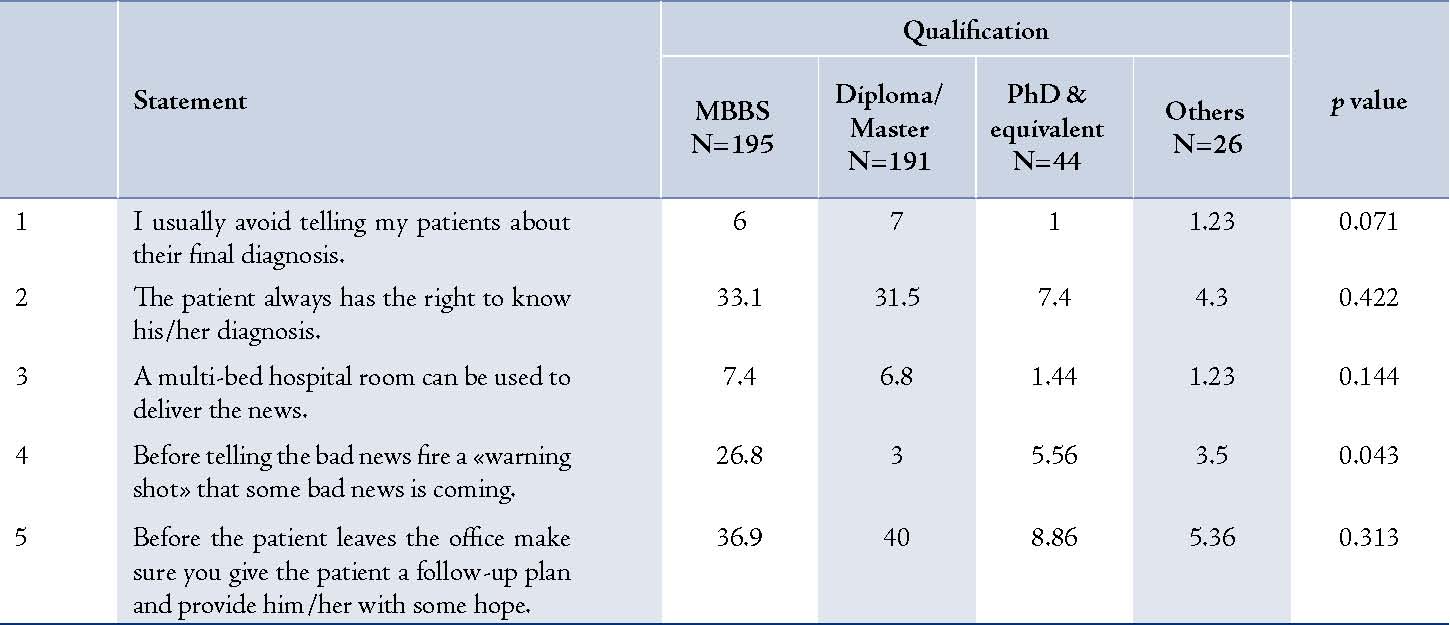
Most physicians in our study (more than 90%) usually do not avoid telling their patients the bad news; however, PHC physicians are less restrained. Almost half of hospital physicians believed that the patient has the right to know the diagnosis while a third of PHC physicians had similar views, (Table 4). Almost one third of "MBBS-only qualified" physicians indicated a better knowledge of the importance of a 'warning shot' while highly qualified physicians did not. (Table 5)
Table 2: Mean knowledge scores by selected characteristics of the respondents.
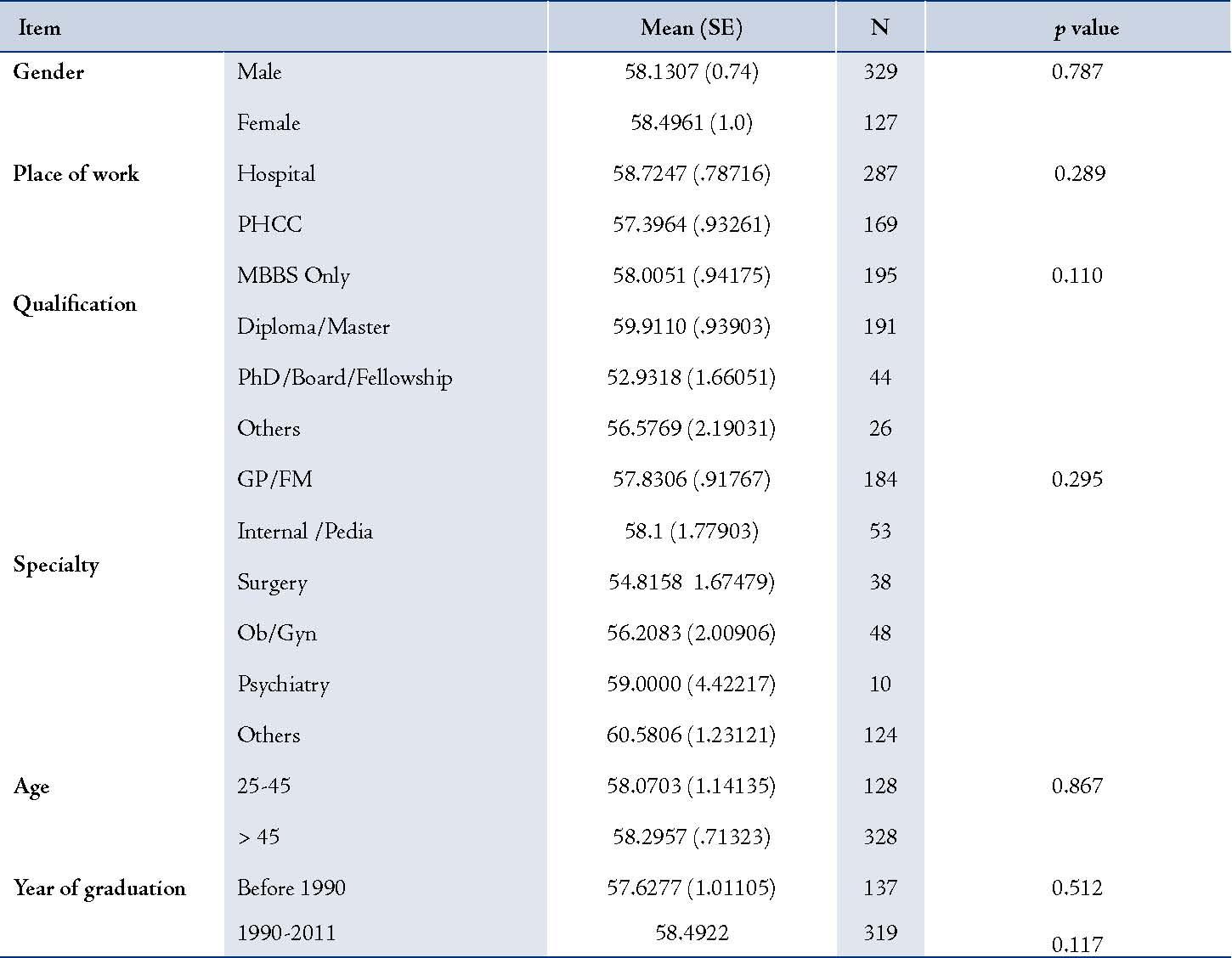
Table 3: Percentage distribution of responses to selected questions by age of the respondents.
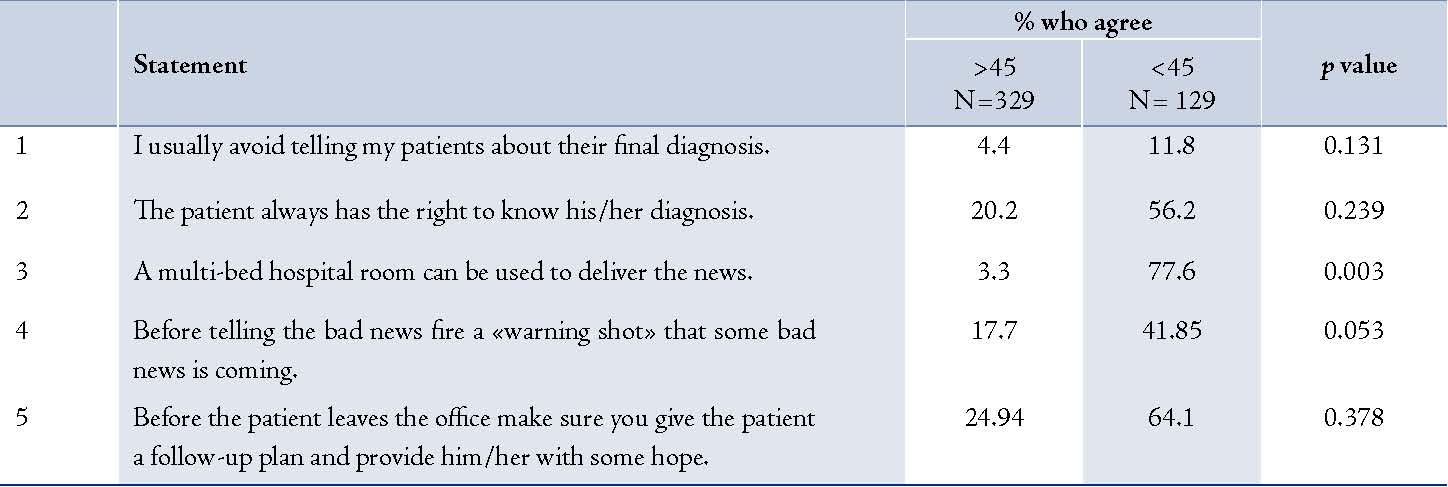
Table 4: Percentage distribution of responses to selected questions by place of work of the respondents.
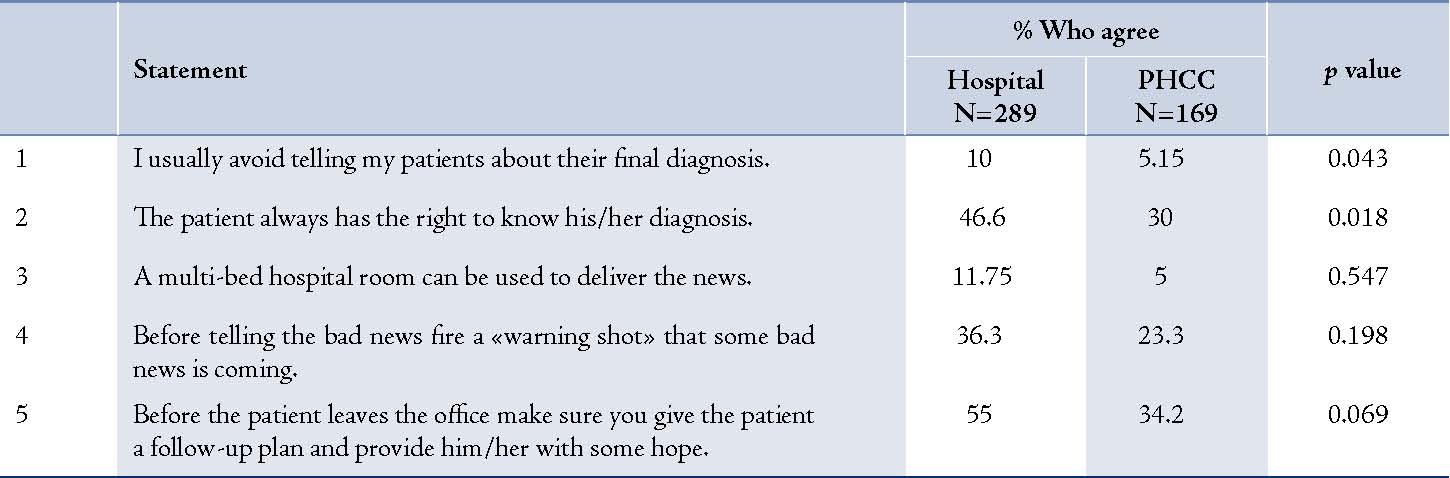
Table 5: Percentage distribution of responses to selected questions by qualification of the respondents.
Discussion
The results of the study raised issues centered on physician - patient communication or more precisely, patient centered communication. The lack of awareness about patients’ rights, lack of appropriate training of physicians, absence of an operational framework governing physician-patient communication, prevalent cultural considerations dominating physician-patient communication or a combination of these factors branch out of the core issue. Let us first rule out the possibility of a void at the policy level. It should be noted that Saudi Arabia has a policy framework that grants certain rights to patients and at the same time expects some responsibilities. This document ensures patients' right to confidentiality; confidential information can only be disclosed if the patient gives explicit consent or if expressly provided for in the law. Information can be disclosed to other healthcare providers only on a strictly "need to know" basis unless the patient has given explicit consent.25 This document could be compared with similar documents from other countries granting rights to patients, e.g., the General Medical Council, the United Kingdom recommends that "If a patient refuses to allow you to inform someone outside the healthcare team of their infection status, you must respect their wishes unless you consider that failure to disclose the information will put healthcare workers or other patients at risk of infection. But such situations are likely to be very rare, not least because of the use of universal precautions to protect healthcare workers and patients, particularly during exposure-prone procedures".26
It could be deduced from the results that our sampled physicians were not aware of the patients’ rights, especially the right to confidentiality. Medical treatment of the patient was more important for them rather than issues related to rights and confidentiality.
Cultural influences sometimes override professional considerations. Perhaps that was the motivating factor for sharing patient information more with relatives than with the patient. Cultural considerations could strongly influence decision making processes about breaking bad news. Cultures where family bonds are strong and families are predominantly patriarchic, such as Saudi culture, tend to place the decision making with elders of the family without really caring about rights or confidentiality. Physicians have to comply with the cultural norms. This situation is compounded by the lack of training in breaking bad news. It increases the vulnerability of the physician to difficult situations and he or she is likely to find it easier to share patient related information with families or relatives without asking for the patient’s permission.
Our survey reveals that physicians find it easier to speak to the relatives of patients than the patients themselves. The underlying factor here is the possibility that the physicians are not giving due importance to the patient who is the owner of the information. This has also been found previously in Saudi Arabia.6
On the other hand, the majority of physicians in the States agreed that a patient should be informed of an incurable cancer diagnosis before it is made known to their family.10 However, there are some reported observations of doctors avoiding such a discussion because it distressed them, either they could not handle these issues or they did not have the time to do so adequately. This situation had a negative effect on doctors’ emotions and tended to increase patients’ distress. This avoidance behavior may result in patients being unwilling to disclose problems, which could delay and adversely impact their recovery.19 Breaking bad news is stressful for both the patient and the physician and it is quite natural that a physician would avoid it, if he or she could.17
In our study, junior physicians had better scores than seniors; this could be due to the fact that medical schools now incorporate BBN in the undergraduate curriculum.27 Traditionally, medical schools devoted more time towards teaching medical skills rather than communication skills. However, this trend is changing. Modern curricula have realized the importance of effective communication between physicians and are giving due importance to this skill.
Hence, physicians who have attended relatively newer curricula are better trained in communicating with patients than their older and experienced colleagues. A study in Germany indicates that pre-registration house officers (PRHOs) are frequently involved in breaking bad news. Their perceptions of competency would indicate that the extensive and compulsory undergraduate teaching they had received on this subject has served to prepare them for this difficult task.28
One of the significant limitations in this study was the low response rate which may give rise to sampling bias. Some authors have challenged the presumption that a lower response rate reflects lower survey accuracy, an example of a finding was reported by Visser, Krosnick, Marquette and Curtin (1996), who showed that surveys with lower response rates (near 20%) yielded more accurate measurements than did surveys with higher response rates (near 60 or 70%).29 In general, however, there is consensus that low response rate is a cause for concern and that researchers should make every effort to motivate their respondents, for example, by using reminders, etc. Assessment of non-response bias should be a part of all such studies.30
Other limitations which should also be noted are; the instrument used needed to be improved to cover more important aspects in patient-doctor communication related to BBN, or an in-depth study on a single aspect. Further research is needed to study this important issue in our practice, a qualitative study may be more helpful.
Conclusion
We conclude that the issue in Saudi Arabia is still "whether" rather than "how" to inform the patient. This is true for our study as well as in similar studies conducted in Saudi Arabia. We believe that although the physicians are keen to help their patients, most of them lack the essential knowledge and skills of breaking bad news. BBN should be ideally a skill learned at medical school. Practicing physicians at all levels should be trained in the skills required for breaking bad news.
Acknowledgements
The authors would like to thank the study participants for taking the time to complete the questionnaire. No conflicts of interest or funding to disclose.
References
1. Dickson D, Hargie O, Brunger K, Stapleton K. Health professionals’ perceptions of breaking bad news. Int J Health Care Qual Assur Inc Leadersh Health Serv 2002;15(6-7):324-336. doi:10.1108/09526860210448492.
2. Alrashdi I. Evaluation of quality of healthcare: to what extent can we rely on patient expectations and preferences. Oman Med J 2012 Nov;27(6):448-449.
3. Al-Wahaibi A, Almahrezi A. An application of educational theories and principles of teaching and learning communication skills for general practitioners in oman. Oman Med J 2009 Apr;24(2):119-127. doi:10.5001/omj.2009.26.
4. Department of Health. Social Services and Public Safety, Castle Buildings, Belfast BT4 3SJ, Ref: 261/02, Breaking Bad News, Regional Guidelines, February 2003 (www.dhsspsni.gov.uk)
5. Bedikian AY, Saleh V, Ibrahim S. Saudi patient and companion attitudes toward cancer. King Faisal Spec Hosp Med J 1985;5:17-25.
6. Mobeireek AF, al-Kassimi FA, al-Majid SA, al-Shimemry A. Communication with the seriously ill: physicians’ attitudes in Saudi Arabia. J Med Ethics 1996 Oct;22(5):282-285. PMC free article. PubMed.
7. Younge D, Moreau P, Ezzat A, Gray A. Communicating with cancer patients in Saudi Arabia. Ann N Y Acad Sci 1997 Feb;809:309-316. PubMed.
8. Mobeireek AF, Al-Kassimi F, Al-Zahrani K, Al-Shimemeri A, al-Damegh S, Al-Amoudi O, et al. Information disclosure and decision-making: the Middle East versus the Far East and the West. J Med Ethics 2008 Apr;34(4):225-229. PubMed.
9. Al-Amri AM. Cancer patients’ desire for information: a study in a teaching hospital in Saudi Arabia. East Mediterr Health J 2009 Jan-Feb;15(1):19-24. PubMed.
10. Aljubran AH. The attitude towards disclosure of bad news to cancer patients in Saudi Arabia. Ann Saudi Med 2010 Mar-Apr;30(2):141-144.
11. Windsor JA, Rossaak JI, Chaung D. Alexander Ng, Bissett IP, Johnson MH. Telling the truth to Asian patients in the hospital setting. NZMJ 28 November 2008, Vol 121 No 1286. http://www.nzma.org.nz/journal/121-1286/3378/
12. Rabow MW, McPhee SJ. Beyond breaking bad news: how to help patients who suffer. West J Med 1999 Oct;171(4):260-263.
13. VandeKieft GK. Breaking bad news. Am Fam Physician 2001 Dec;64(12):1975-1978.
14. Annunziata MA, Foladore S, Magri MD, Crivellari D, Feltrin A, Bidoli E, et al. Does the information level of cancer patients correlate with quality of life? Aprospective study. Tumori 1998;84:623.
15. Mystakidou K, Parpa E, Tsilila E, Katsouda E, Vlahos L. Cancer information disclosure in different cultural contexts. Support Care Cancer 2004 Mar;12(3):147-154.
16. Al-Ahwal M. Cancer patients’ awareness of their disease and prognosis. Ann Saudi Med 1998 Mar-Apr;18(2):187-189.
17. Fallowfield L, Jenkins V. Communicating sad, bad, and difficult news in medicine. Lancet 2004 Jan;363(9405):312-319.
18. McCabe MS, Wood WA, and Goldberg RM. When the Family Requests Withholding the Diagnosis: Who Owns the Truth? Journal of Oncology Practice. Vol. 6, Issue 2. Doi: 10.1200/Jop.091086
19. Ha JF, Longnecker N. Doctor-patient communication: a review. Ochsner J 2010;10(1):38-43.
20. Buckman R. Communication in palliative care: a practical guide. In: Dickenson D, Johnson M, Katz JS, eds.Death, Dying and Bereavement. 2nd edn. Sage, London 2000:146-73.
21. Ptacek JT, Eberhardt TL. Breaking bad news. A review of the literature. JAMA 1996 Aug;276(6):496-502.
22. Buckman R. Breaking Bad News: A Guide for Health Care Professionals. Baltimore: Johns Hopkins.
23. Baile WF, Buckman R, Lenzi R, Glober G, Beale EA, Kudelka AP. SPIKES-A six-step protocol for delivering bad news: application to the patient with cancer. Oncologist 2000;5(4):302-311.
24. Johns R. Likert items and scales, survey question bank: Methods Fact Sheet 1 (March 2010) (University of Strathclyde) http://surveynet.ac.uk/sqb/datacollection/likertfactsheet.pdf
25. Saudi Ministry of Health, Administrative Policy and Procedure titled ‘Patient Rights and Responsibilities’, Policy number ICU-APP-MOH-005E(1) of 01-09-1432, Section 5.8 - Right to Confidentiality, para 5.8.2.
26. General Medical Council. Confidentiality: disclosing information about serious communicable diseases. September 2009. http://www.gmc-uk.org/guidance/ethical_guidance/confidentiality_serious _communicable_diseases.asp
27. Simmenroth-Nayda A, Alt-Epping B, Gágyor I. Breaking bad news - an interdisciplinary curricular teaching-concept. GMS Z Med Ausbild 2011;28(4):Doc52.
28. Schildmann J, Cushing A, Doyal L, Vollmann J. Breaking bad news: experiences, views and difficulties of pre-registration house officers. Palliative Medicine 2005; 19: 93_/98
29. Visser, Penny S, Krosnick JA, Marquette J, Curtin M. Mail Surveys for Election Forecasting? An Evaluation of the Colombia Dispatch Poll. Public Opin Q 1996;60:181-227.
30. Cook JV, Dickinson HO, Eccles MP. Response rates in postal surveys of healthcare professionals between 1996 and 2005: An observational study. BMC Health Services Research. 2009; 9:160 doi:10.1186/1472-6963-9-160.This article is available from: http://www.biomedcentral.com/1472-6963/9/160.
|