|
Abstract
This review aims to summarize the major changes in the2010 Heart and Stroke foundation of Canada (HSFC) andthe American Heart Association (AHA) Pediatric Basic andAdvanced Life Support Guidelines. The Guidelines were based onthe International Liaison Committee on Resuscitation’s (ILCOR)comprehensive, evidence-based review of the resuscitationliterature. The key recommendations from the Guidelines include:the removal of “look, listen and feel” and a de-emphasis on theuse of the pulse check by healthcare providers to diagnose cardiacarrest; a change in the sequence of resuscitation for patientsin cardiac arrest from the previously well-known “A-B-C” i.e.Airway, Breathing, and Chest Compressions to “C-A-B” i.e.Chest Compressions first; modification to the appropriate depthof compression (at least 1/3 of the anterior-posterior depth of thechest wall or about 4 cm in infants and 5 cm in children); end-tidalCO2 monitoring (in intubated patients) to assess the quality ofchest compressions and optimize cardiopulmonary resuscitation(CPR); and titrating Fi0O2 once “Return of SpontaneousCirculation” (ROSC) is achieved to maintain an oxygen saturationbetween 94-99%. Overall, pediatricians, family and communityphysicians who may care for acutely ill children should be aware ofthese updated guidelines in order to provide the best possible careto their patients.
Keywords: Pediatric Resuscitation; Pediatric basic life support; paediatric advanced life support, 2010 ACC/AHA guidelines.
Introduction
In October 2010, the American Heart Association (AHA) and Heart and Stroke Foundation of Canada (HSFC) published updated Guidelines on Pediatric Basic Life Support (PBLS) and Pediatric Advanced Life Support (PALS). The present review highlights the significant changes made to the PBLS and PALS Guidelines relevant to pediatricians as well as family and community physicians. The complete guidelines are published in the journal Circulation, and can be accessed at www.circulationaha.org. Neonatal resuscitation is not included in this article, however the complete Neonatal Resuscitation Guidelines are available on-line at Circulation (Circulation, 2010; 122(suppl 3): S909-S919). 1
Quality of evidence
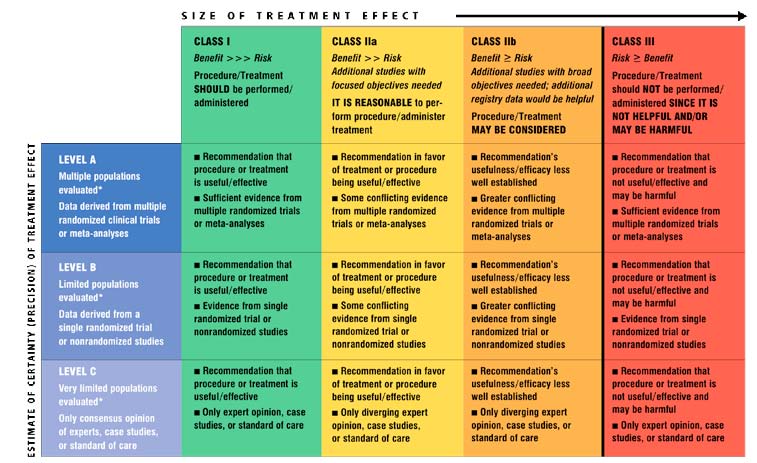
The AHA/HSFC Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiovascular Care (ECC) are based on the ILCOR “Consensus on Science and Treatment Recommendations”, the most up-to-date and comprehensive review of resuscitation literature.2 The ‘Levels of Evidence’ of these Guidelines is consistent with the format used by the American College of Cardiology Foundation and the American Heart Association. (Table 1)
Part I: Pediatric Basic Life Support (PBLS)
A number of changes have been made to the Pediatric Basic Life Support Gguidelines and a summary of the key changes is presented below.
Key PBLS issues and major changes in the 2010 HSFC and AHA Guidelines:
- Elimination of “Look, Listen and Feel” for assessment of cardiac arrest
- No Pulse check for lay rescuers. Healthcare providers (HCPs) may take up to 10 sec to feel for a pulse. If in doubt, start CPR.
- C-A-B instead of A-B-C: Initiate chest compressions before giving rescue breaths
- Increased emphasis on high quality CPR
- An automated external defibrillator (AED)* may be used for an infant if a manual defibrillator is not available.
Elimination of “look, listen and feel”
The Guidelines have removed the use of “look, listen and feel” to diagnose a potential cardiac arrest victim. The new recommendation is to initiate CPR if the victim is unresponsive and not breathing (or only gasping). (Table 1 Class IIa, LOE C)
Table 1: Classification of recommendation and level of Evidence
The Utility of the Pulse Check
Lay rescuers should not use the pulse check to diagnose cardiac arrest. In addition, the assessment of a pulse by healthcare providers is not reliable. They should take no more than 10 seconds to check for a pulse (brachial in infant and carotid or femoral in a child). If within 10 seconds, no pulse can be felt or the provider is unsure of its presence, chest compressions should be started immediately. (Table 1 Class IIa, LOE C)
The Change of Sequence from ABC to CAB
The 2010 HSFC and AHA Guidelines for PBLS changed the sequence of resuscitation for patients in cardiac arrest from the previously well-known “A-B-C” i.e. Airway, Breathing, and Chest Compression to “C-A-B” i.e. Chest Compressions first. The rationale for this change is as follows:
1. Bystander CPR dramatically improves survival from out-of-hospital cardiac arrest in both pediatric and adult populations.3-5 Unfortunately, only 15-30% of out-of-hospital sudden cardiac arrest victims receive CPR prior to the arrival of Emergency Medical Services (EMS).6,7 Reluctance to initiate CPR may, in part, relate to the technical difficulty in opening the airway and delivering rescue breaths. Therefore, starting with chest compressions (the ‘simpler’ component of CPR) may encourage more witnesses to act when faced with victims of cardiac arrest.
2. The majority of cardiac arrest victims are adults where Ventricular Fibrillation (VF) or pulseless Ventricular Tachycardia (VT) is common. Those victims have better survival when the arrest is witnessed and when chest compression and defibrillation are initiated rapidly. The change to the CAB sequence will simplify BLS training and make teaching consistent for arrest victims of all age groups (infants, children and adults) with the hope that more bystanders will be willing to provide at least chest compressions when faced with a cardiac arrest victim.
3. In contrast to adults, cardiac arrests in infants and children are usually asphyxial in nature i.e. secondary to hypoxia or shock (which, if left untreated, leads to progressive bradycardia and ultimately asystole, not primary VF as in adults). Thus ventilation is critically important in pediatric resuscitation. However, performing 30 chest compressions before ventilation will theoretically only delay ventilation by approximately 18 seconds (for the lone rescuer) and even less for two healthcare providers. This minimal delay is unlikely to affect the outcome of resuscitation, but will probably generate blood flow to vital organs sooner. There is no evidence to suggest that starting with ventilation (as in ABC) is superior to starting with chest compressions (as in CAB).
Compression-Ventilation Ratio for Infants and Children
The compression-to-ventilation ratio of 30:2, for the lone rescuer, and 15:2, for two healthcare providers, is the same as the previous 2005 Guidelines. Once an advanced airway is in place, synchronization of chest compressions with ventilation is not required. Instead, chest compressions should be continued with no /or minimal interruption, at a rate of at least 100/min without pause for ventilation. The ventilation rate should be 8-10 breaths/min to avoid excessive ventilation. It is important to note the differences in resuscitation of the newly born in the delivery room as compared to that in infants and children. The compression-to-ventilation ratio for neonatal resuscitation is 3:1 with a pause for ventilation whether or not the infant has an advanced airway. This compression-to-ventilation ratio applies only to newborns in the delivery room and in the newborn nursery /or neonatal intensive care unit (NICU). Once the infant leaves the hospital, the resuscitation should be conducted with the usual 30:2 (one rescuer) or 15:2 (two rescuer) compression-to-ventilation ratios.
Hands-only CPR is NOT Recommended for Children
Cardiac arrests in children are typically asphyxial in nature precipitated by hypoxia or shock which progresses to cardiac arrest compared to that in adults where sudden cardiac arrest is frequent from a primary cardiac etiology. Animal studies demonstrate that hands-only CPR is sufficient to resuscitate VF cardiac arrest (which is common in adults) but not asphyxial cardiac arrest (which is common in children).8,9
A recent meta-analysis of randomized control trials showed an increase in survival to hospital discharge with hands-only compared to conventional CPR in adult cardiac arrest victims.10 However, a large pediatric out-of-hospital cardiac arrest study showed that cardiac arrest victims receiving conventional CPR had more favourable neurological outcomes compared to those who received hands-only CPR.
Thus, the new guidelines consider optimal CPR for infants and children to include both ventilation and chest compression (Table 1 Class I, LOE B). However, chest compression alone is preferable to no CPR if the bystander is unwilling or unable to perform conventional CPR.
Emphasis on Effective Chest Compression
High quality chest compressions are the cornerstone of successful CPR. Inadequate chest compression rate and depth are common during CPR even among healthcare providers.11,12 Evidence shows that cardiac arrest victims frequently receive excessive ventilation during CPR which increases intrathoracic pressure causing a decrease in venous return and cardiac output, barotrauma and aspiration.11 The new Guidelines recommend using only the force and tidal volume (TV) needed to just make the chest rise visibly. Each breath should be given over approximately one second at a rate of 8-10 breaths/minute if the patient is intubated.
Key elements of high quality CPR:
- Push fast (at least 100/min)
- Push hard (4 cm in infant, 5 cm or 1/3 of chest depth in children)
- Allow full chest recoil between compressions
- Avoid excessive ventilation
- Minimize interruptions
- Avoid pre-shock pause
- Resume CPR immediately after a shock
- Rotate compressor role every 2 min (to avoid fatigue).
Defibrillation and the use of Automated External Defibrillators (AEDs)
Pediatric cardiac arrest victims with a shockable rhythm (VF or pulseless VT) require rapid defibrillation, which may be achieved through either a manual defibrillator or an AED. Manual defibrillation is preferred in infants and children and the recommended first shock energy dose is 2-4 J/kg. Subsequent defibrillation attempts should use energy doses of at least 4 J/kg (but not to exceed 10 J/kg). If a manual defibrillator is not available, an AED with a pediatric dose attenuator is preferred for both infants (below one year of age) and in children below eight years of age. However, if neither is available, an AED without a dose attenuator may be used (Table 1 Class IIb, LOE C). It is important to resume chest compressions immediately after the shock, without stopping to analyze the cardiac rhythm, and continue until it is time for the next rhythm check (2 minutes or about 5 cycles of CPR).
Part II: Pediatric Advanced Life Support (PALS)
Several changes have been made to the Pediatric Advanced Life Support Guidelines and a summary of the key changes is presented below.
Key PALS issues and major changes in the 2010 HSFC and AHA Guidelines:
- End Tidal (ET) CO2 monitoring is recommended to confirm endotracheal intubation and may be used to assess and improve the quality of chest compressions.
- Cuffed endotracheal tubes are acceptable for use in infants and children.
- Routine use of cricoid pressure is not recommended.
- Once ROSC is achieved, titrate FiO2 to achieve arterial oxyhemoglobin saturation between 94% and 99% to limit the risk of hyperoxemia.
- Therapeutic hypothermia may be considered for infants and children if they remain comatose after resuscitation from cardiac arrest.
- Limit administration of calcium in resuscitation to specific circumstances (e.g. documented hypocalcemia, calcium channel blocker overdose, hypermagnesemia or hyperkalemia).
- Adenosine may be used for the diagnosis and treatment of regular, monomorphic wide-complex tachycardia in patients who are not known to have Wolff-Parkinson-White (WPW) syndrome.
- Young victims with unexplained sudden cardiac death should have an unrestricted, complete autopsy with preservation of tissue for genetic analysis. The results may help identify other family members with an inherited channelopathy.
End-Tidal CO2 Monitoring and the Quality of CPR
ETCO2 monitoring may be used as an indicator of the quality of chest compressions and be useful to guide therapy. If the ETCO2 is consistently <10-15 mm Hg, CPR may need to be modified to ensure adequate cardiac output by pushing fast and hard, avoiding hyperventilation and minimizing interruptions. Hyperventilation increases intra-thoracic pressure, decreases preload to the heart and hence decreases cardiac output.
Return of Spontaneous Circulation (ROSC) may be preceded by an abrupt and sustained increase in ETCO2 which is a marker of increased pulmonary blood flow. It can be used as a physiological marker of ROSC, instead of pulse checks, thus avoiding unnecessary interruptions in chest compressions.
Cuffed versus Uncuffed Endotracheal Tubes
The use of both cuffed and uncuffed endotracheal tubes are acceptable when intubating infants and children (Table 1 Class IIa, LOE C). The cuffed endotracheal tube size can be estimated by using the following formula for children older than two years of age:
Cuffed endotracheal tube size ID (mm) = 3.5 + (age/4)
For infants less than 1 year of age, and children between 1 and 2 years of age, it is reasonable to use a cuffed endotracheal tube with an internal diameter of 3.0 mm and 3.5 mm, respectively.
Cricoid Pressure
There is inadequate evidence to recommend the routine use of cricoid pressure when intubating a child or infant with cardiac arrest. (Table 1 Class III, LOC C)
Post-Resuscitation Care
Titrating oxygen to appropriate levels after ROSC
Resuscitation should be conducted with 100% oxygen until circulation is restored. Once ROSC is achieved, adjust the FiO2 to maintain oxygen saturation between 94% and 99% (Table 1 Class IIb, LOE C), as hyperoxia can increase reperfusion injury after an ischemic insult. In a recent multicenter, cohort study of patients admitted to ICU after resuscitation from cardiac arrest, the mortality was significantly higher in the hyperoxia group compared to the hypoxia and normoxia groups.13
Therapeutic hypothermia after cardiac arrest
The use of therapeutic hypothermia (32°C-34°C) is reasonable for adolescents who remain comatose after resuscitation from sudden, witnessed, out-of-hospital VF arrest (Table 1 Class IIb, LOE C). It may be considered for infants and children who remain comatose after cardiac arrest (Table 1 Class IIb, LOE C).
The Key highlights with regards to medications during cardiac arrest
Medication Dose Calculation
To calculate resuscitation medication, use the actual (and not the ideal) body weight of the child, or use a body length tape with pre-calculated doses (Table 1 Class IIa, LOE C) regardless of the habitus of the child, but not to exceed the standard dose recommended for adults.
Adenosine
Wide complex tachycardia may be ventricular or supraventricular in origin. Consultation with an expert in pediatric arrhythmias is strongly recommended before treatment in stable patients as all anti-arrhythmics can cause serious side effects. Recent evidence suggests that adenosine is relatively safe for both treatment and diagnosis of regular, monomorphic, wide-complex tachycardia (Table 1 Class IIb, LOE B). However, adenosine should not be given if the rhythm is irregular, or polymorphic and/or an unstable wide-complex tachycardia as it may cause VF. Adenosine should not be used for wide-complex tachycardia in patients with known Wolff-Parkinson-White syndrome.
Evaluation of unexplained, Sudden Cardiac Death victims
Cardiac ion channelopathies such as long QT syndrome are increasingly recognized as an important cause of Sudden Cardiac Death (SCD) in young people. When SCD occurs in children or young adults, a complete past medical and family history are essential (see important screening questions) and review of previous ECGs, if available, may be helpful in identifying families at risk. Victims of unexplained SCD should, if resources allow, have an unrestricted, complete autopsy ideally performed by a pathologist with experience in cardiovascular pathology. Their family members should be referred for screening (Table 1 Class I, LOE C) to healthcare providers or centers with expertise in arrhythmias.
Important past medical and family screening questions for sudden cardiac arrest include:
- History of syncopal episodes
- History of seizures
- Unexplained accidents or drowning
- Sudden, unexplained death at <50 years of age
Education and Implementation
Cardiac arrest outcomes depend heavily on the performance of CPR by lay rescuers and healthcare providers. Maximizing survival from cardiac arrest requires improvements in education and the implementation of systems that support the delivery of high-quality resuscitation and post-arrest care, including mechanisms to systematically monitor resuscitation performance of community-based and hospital-based systems.
For lay rescuers, one significant factor that can affect their willingness to perform CPR (a major determinant of survival) is recent training.14 Family physicians may be able to improve survival from cardiac arrest by promoting CPR training of their patients and families and may themselves serve as examples by keeping their basic life support certification up to date. Interestingly, CPR skills can be learned equally well and retained with short (e.g. 22 minutes) video-based self-instruction courses combined with synchronous hands-on practice and by longer traditional training courses. (Table 1 Class I, LOE A)
Emergency Medical Services dispatchers should provide CPR instructions to callers reporting a potential cardiac arrest victim who is unresponsive and not breathing or gasping as this has been shown to increase the willingness of bystanders to perform CPR and patient survival. For a complete reference on the important issues in education and implementation of resuscitation programs, the reader is referred to the complete guidelines in the journal Circulation (Circulation, 2010;122(suppl 3):S920-S933).
Conclusion
Cardiac arrest remains an important issue in the care of pediatric and adult patients. This article reminds practitioners of the differences in the etiology of pediatric and adult cardiac arrests while also describing the major updates to the new guidelines for the management of pediatric cardiac arrest. Further improvement in the care of all cardiac arrest patients is likely to occur through education and appropriate implementation of resuscitation programs and quality assurance.
References
1. Perlman JM, Wyllie J, Kattwinkel J, Atkins DL, Chameides L, Goldsmith JP, et al. Part 11: Neonatal resuscitation: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 2010; 122(16 Suppl 2):S516-538.
2. de Caen AR, Kleinman ME, Chameides L, Atkins DL, Berg RA, Berg MD, et al. Part 10: Paediatric basic and advanced life support: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Resuscitation 2010; 81 Suppl 1:e213-259.
3. Sasson C, Rogers MA, Dahl J, Kellermann AL. Predictors of survival from out-of-hospital cardiac arrest: a systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes 2010; 3(1):63-81.
4. Kitamura T, Iwami T, Kawamura T, Nagao K, Tanaka H, Nadkarni VM, et al. Conventional and chest-compression-only cardiopulmonary resuscitation by bystanders for children who have out-of-hospital cardiac arrests: a prospective, nationwide, population-based cohort study. Lancet 2010; 375(9723):1347-1354.
5. SOS-KANTO Study Group, Cardiopulmonary resuscitation by bystanders with chest compression only (SOS-KANTO): an observational study. Lancet 2007; 369(9565):920-926.
6. Abella BS, Aufderheide TP, Eigel B, Hickey RW, Longstreth WT, Nadkarni V, et al. Reducing barriers for implementation of bystander-initiated cardiopulmonary resuscitation: a scientific statement from the American Heart Association for healthcare providers, policymakers, and community leaders regarding the effectiveness of cardiopulmonary resuscitation. Circulation 2008; 117(5):704-709.
7. Donoghue AJ, Nadkarni V, Berg RA, Osmond MH, Wells G, Nesbitt L, et al. Out-of-hospital pediatric cardiac arrest: an epidemiologic review and assessment of current knowledge. Ann Emerg Med 2005; 46(6):512-522.
8. Berg RA, Kern KB, Hilwig RW, Berg MD, Sanders AB, Otto CW, et al.Assisted ventilation does not improve outcome in a porcine model of single-rescuer bystander cardiopulmonary resuscitation, Circulation 1997; 95(6):1635-1641.
9. Berg RA, Kern KB, Hilwig RW, Ewy GA. Assisted ventilation during 'bystander' CPR in a swine acute myocardial infarction model does not improve outcome. Circulation 1997; 96(12):4364-4371.
10. Hüpfl M, Selig HF, Nagele P. Chest-compression-only versus standard cardiopulmonary resuscitation: a meta-analysis. Lancet 2010; 376(9752):1552-1557.
11. Abella BS, Alvarado JP, Myklebust H, Edelson DP, Barry A, O'Hearn N, et al. Quality of cardiopulmonary resuscitation during in-hospital cardiac arrest. JAMA 2005; 293(3):305-310.
12. Wik L, Kramer-Johansen J, Myklebust H, Sørebø H, Svensson L, Fellows B, et al. Quality of cardiopulmonary resuscitation during out-of-hospital cardiac arrest. JAMA 2005; 293(3):299-304.
13. Kilgannon JH, Jones AE, Shapiro NI, Angelos MG, Milcarek B, Hunter K, et al. Association between arterial hyperoxia following resuscitation from cardiac arrest and in-hospital mortality. JAMA 2010; 303(21):2165-2171.
14. Bhanji F, Mancini ME, Sinz E, Rodgers DL, McNeil MA, Hoadley TA, et al. Part 16: education, implementation, and teams: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2010; 122(18 Suppl 3):S920-933.
|