Sesamoid bones are small sized bones present within tendons where they cross joints in various locations in the limbs, including the hands, wrists, knees, and feet. They are usually ovoid or round with sizes varying from 5–10 mm. They are mostly formed from a single ossification center. If they are formed from multi-ossification centers, then they remain unfused.1,2 By facilitating the gliding movements, these bony nodules reduce the friction over tendons and thereby protect them from injuries. Galen was the first to describe them as ‘sesamoid’ due to their resemblance with sesame seeds.3 The presence of two sesamoid bones in the first metatarsophalangeal (MTP) joint is not considered to be an anatomical abnormality of the human skeleton.4,5 However, sesamoid bones are also found at the tendons over other MTP joints. The highest prevalence of sesamoid bones was reported to be at the first MTP joint followed by the fifth MTP joint, while the lowest were seen at the third and fourth MTP joints.4 Most of these variations are recognized incidentally during radiological imaging in clinical practice. Evidence from reported studies demonstrates that the prevalence and appearance of sesamoid bones in the foot varies considerably among different populations and ethnic groups.4,6–10 In Bahraini Arabs, the reported prevalence of sesamoid bones was 2.1% and 11.6% in the second and fifth MTP joints, respectively.10 A low prevalence was observed at the third and fourth MTP joints (0.6%).10 Rare variations of sesamoid bones in the foot, including the occurrence of six bones or the presence of a single bone, were also reported.11 Recently scientific evidence of coincidental development of sesamoid bones at MTP joints has also been documented.7
Sesamoid bones are associated with various pathological conditions including fractures, sub-sesamoid joint degeneration, and sesamoiditis.12–14 A fracture involving a unipartite sesamoid bone may cause diagnostic confusion with a congenital bipartite sesamoid bone.15 Due to poor blood supply, sesamoid bones are more susceptible to avascular necrosis.16 Sesamoiditis is one of the common causes of foot pain, which generally results from cartilage abnormalities or inflammation of peritendinous structures.17 Sesamoids may compress the plantar digital nerves due to their close relation.5 Prior knowledge of prevalence rates and specific distribution patterns is of clinical significance as sesamoid bones are associated with various disabling problems of the forefoot and often are misdiagnosed with other pathologies resulting in a delay in appropriate treatment. Despite its clinical significance, the data of sesamoid bone prevalence in Middle Eastern populations is less explored. Hence, our study aimed to investigate the prevalence, distribution patterns, and coexistence of foot sesamoid bones among Omani patients referred to a tertiary care hospital.
Methods
We conducted a retrospective study among patients (aged ≥ 18 years) who had been referred for a foot X-ray to the Department of Radiology and Molecular Imaging, Sultan Qaboos University Hospital (SQUH), Muscat, Oman, in 2018. Patients’ data was obtained from the computerized database ‘TRACK CARE’. We reviewed the antero-posterior and lateral radiograms of the foot using the picture archiving and communication system (PACS, Version 4.4.516.21; Philips, Foster City, USA). The sesamoid bones were noted from each radiograph manually. Patients with a history of foot fractures and injuries, amputated toes, and non-Omani patients were excluded from the study. We also collected patient demographics, such as age and gender. Institutional ethical approval was granted before the start of the study. The data was collected independently by two observers. The uncertain cases were noted from the two independent data files. Later, a final decision on these uncertain cases was taken with consensus. Based on a study on a Bahraini population,10 we assumed on an average a sesamoid bone prevalence rate of 2.1%, 0.6%, 0.6%, 12.1%, and 3.1% at second, third, fourth, fifth MTP joints, and first interphalangeal (IP) joint of hallux, respectively, in the Omani population to determine the required sample size for this study. We considered an absolute precision of 2.5% and confidence level of 95%, and the minimum sample size required for our study was 120, 37, 37, 649, and 236, respectively, for the above-mentioned joints (nMaster 2.0. Sample Size Software, Biostatistics Resource and Training Centre, Biostatistics Department, Christian Medical College, Vellore-632 002, India (2012)). Although it was decided that a minimum sample size of 649 was needed, we managed to include all the patients who had foot X-rays during the study year 2018. Ultimately, 711 patients were included in the study.
Table 1: Association of sesamoid bones presence at each joint in the foot with respect to gender.
|
1st IP |
26 (9.6) |
15 (8.7) |
19 (11.1) |
17 (10.7) |
45 (10.2) |
32 (9.6) |
|
1st MTP |
271 (100) |
173 (100) |
171 (100) |
159 (100) |
442 (100) |
332 (100) |
|
2nd MTP |
16 (5.9) |
5 (2.9) |
6 (3.5) |
2 (1.3) |
22 (5.0) |
7 (2.1) |
|
3rd MTP |
4 (1.5) |
2 (1.2) |
2 (1.2) |
0 (0.0) |
6 (1.4) |
2 (0.6) |
|
4th MTP |
3 (1.1) |
1 (0.6) |
2 (1.2) |
1 (0.6) |
5 (1.1) |
2 (0.6) |
IP: interphalangeal; MTP: metatarsophalangeal.
Table 2: Association of sesamoid bones presence at each joint in the foot with respect to age.
|
1st IP* |
27 (9.8) |
19 (10.1) |
8 (7.5) |
10 (10.8) |
10 (18.9) |
3 (6.7) |
0 (0.0) |
0 (0.0) |
|
1st MTP* |
276 (100) |
188 (100) |
106 (100) |
93 (100) |
53 (100) |
45 (100) |
7 (100) |
6 (100) |
|
2nd MTP* |
11 (4.0) |
3 (1.6) |
6 (5.7) |
3 (3.2) |
5 (9.4) |
1 (2.2) |
0 (0.0) |
0 (0.0) |
|
3rd MTP* |
3 (1.1) |
1 (0.5) |
1 (0.9) |
1 (1.1) |
2 (3.8) |
0 (0.0) |
0 (0.0) |
0 (0.0) |
|
4th MTP* |
1 (0.4) |
0 (0.0) |
3 (2.8) |
1 (1.1) |
1 (1.9) |
0 (0.0) |
0 (0.0) |
1 (16.7) |
IP: interphalangeal; MTP: metatarsophalangeal.
*No significant difference across age groups for right and left side joints; #p = 0.030 (right side joint across age groups);#p < 0.010 (left side joint across age groups).

Figure 1: Radiographs (anterior-posterior views) showing rare distributions of sesamoid bones at the first metatarsophalangeal joint. (a) Single sesamoid bone (red arrow); (b) and (c) unilateral bipartite sesamoids (red arrows); and (d) bilateral bipartite sesamoids (red arrows).
Table 3: Sex-wise distribution patterns of sesamoid bones at the metatarsophalangeal (MTP) joints.
|
1st MTP only |
286 |
375 |
661 (85.4) |
|
1st and 2nd MTP |
1 |
5 |
6 (0.8) |
|
1st and 3rd MTP |
0 |
1 |
1 (0.1) |
|
1st and 5th MTP |
36 |
44 |
80 (10.3) |
|
1st, 2nd, 5th MTP |
2 |
11 |
13 (1.7) |
|
1st, 4th, and 5th MTP |
0 |
2 |
2 (0.3) |
|
1st, 2nd, 3rd, and 5th MTP |
2 |
4 |
6 (0.8) |
|
1st, 2nd, 4th, and 5th MTP |
3 |
1 |
4 (0.5) |
|
1st, 3rd, 4th and 5th MTP |
0 |
1 |
1 (0.1) |

Figure 2: Radiographs (anterior-posterior views) showing various distribution patterns of sesamoid bones across metatarsophalangeal (MTP) joints: (a) sesamoids only at first MTP joint (red arrows); (b) first and second MTP joints (red arrows); (c) first and third MTP joints (red arrows); and (d) first and fifth MTP joints in (red arrows).
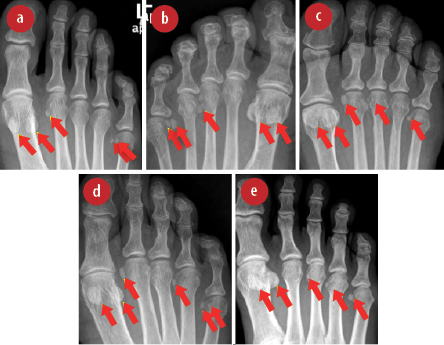
Figure 3: Radiographs (anterior–posterior views) showing various distribution patterns of sesamoid bones across metatarsophalangeal (MTP) joints: (a) first, second, and fifth MTP joints (red arrows); (b) first, fourth, and fifth MTP joints (red arrows); (c) first, second, third, and fifth MTP joints (red arrows); (d) first, second, fourth, and fifth MTP joints (red arrows); and (e) first, third, fourth, and fifth MTP joints (red arrows).
Table 4: Coincidence of sesamoid bones at metatarsophalangeal (MTP) joints.
|
Hallux |
|
|
|
|
|
r |
a |
a |
a |
a |
|
p-value |
- |
- |
- |
- |
|
Second toe |
|
|
|
|
|
r |
- |
0.383 |
0.269 |
0.377 |
|
p-value |
- |
< 0.050 |
< 0.050 |
< 0.050 |
|
Third toe |
|
|
|
|
|
r |
- |
- |
0.125 |
0.219 |
|
p-value |
- |
- |
< 0.050 |
< 0.050 |
|
Fourth toe |
|
|
|
|
|
r |
- |
- |
- |
0.240 |
r: Spearman’s correlation coefficient; a: no correlation.
Table 5: Distribution of sesamoid bones in the foot reported by various studies.a
|
1st MTP |
100 |
100 |
100 |
100 |
100 |
99.96 |
100;100 |
100 |
|
2nd MTP |
1.6 |
1 |
- |
2.1 |
0.4 |
3.08 |
5;8 |
3.7 |
|
3rd MTP |
- |
1 |
- |
0.6 |
0.2 |
0.39 |
2;1 |
1 |
|
4th MTP |
- |
2 |
- |
0.6 |
0.1 |
0.69 |
2;2 |
0.9 |
|
5th MTP |
5.5-6.2 |
10 |
10.8 |
12.1 |
4.3 |
8.94 |
14;25 |
13.7 |
|
1st IP |
50.6 |
5 |
- |
3.9 |
2 |
59.22 |
68;65 |
9.9 |
|
2nd IP |
1.2 |
1 |
- |
- |
- |
- |
- |
- |
MTP: metatarsophalangeal; IP: interphalangeal; CR: conventional radiograph; DTS: digital tomosynthesis tool.
aadapted from Bizarro (1921) and Yammine (2014).
The statistical analysis was performed using SPSS Statistics (IBM Corp. Released 2015. IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp.). Descriptive statistics were used to present the data. The associations between the presence or absence of sesamoid bones at different locations and the age and gender were studied using the chi-square test. Spearman’s correlation coefficient was used to evaluate the coincidence of specific distributions of sesamoid bones at the MTP joints. A p-value < 0.050 was considered statistically significant.
Results
We reviewed a total of 774 foot X-ray radiographs from 711 patients for the presence of sesamoid bones. Among these patients, 419 were men (58.9%) and 292 were women (41.1%). All patients contributed to an overall 442 (57.1%) radiographs of right foot and 332 (42.9%) radiographs of left foot. The two observers agreed 90.0% of the time in their opinions regarding the identification of the presence of sesamoid bones in the plain radiographs. For the remaining 10.0% of cases, the discrepancy was resolved by mutual discussion and agreement. The presence of sesamoid bones was noted plantar to all the MTP joints and IP joint of the great toe. The prevalence of sesamoid bones at each of the five MTP joints and IP joint of great toe with respect to gender, on the right and left foot, is reported in Table 1. The overall prevalence rate was 100% (n = 774) at the first MTP joint, 3.7% (n = 29) at the second MTP, 1.0% (n = 8) at the third MTP, 0.9% (n = 7) at the fourth MTP, 13.7% (n = 106) at the fifth MTP, and 9.9% (n = 77) at the IP of great toe. Sesamoid bones were not found on the plantar surface of the proximal and distal IP joints of second, third, fourth, and fifth toes. Around 40 (5.2%) subjects showed bipartite sesamoid bones at first MTP. Among them, there were 4.3% bipartite medial sesamoid, 0.5% bipartite lateral sesamoid, and 0.2% bilaterally partitioned sesamoids. A rare variation for the presence of single sesamoid bones was noted at the first MTP joints in 0.4% of radiographs [Figure 1]. There was no association between the prevalence of sesamoid bones and gender at each joint in the foot.
The prevalence rate of sesamoid bones in the different age groups is given in Table 2. The mean age of study subjects was 39.8±17.2 years (range: 18–101 years). No association between age and presence or absence of sesamoid bones was identified at the first, second, third, and fourth MTP joints. However, a positive association between age and presence or absence sesamoid bones was observed at the fifth MTP joint (right side p = 0.030; left side p < 0.010). As the timeline of ossification extends through the old age, our study observation reveals that with increasing age, the occurrence of sesamoid bones is likely to increase at the fifth MTP joint.
Various distribution patterns of sesamoid bones were identified and presented in Table 3. The presence of sesamoid bones at two or more joints was noted in 14.6% of radiographs. There were nine coexisting sesamoid bone patterns observed [Figure 2 and 3].
Spearman’s correlation test was performed to test for correlation between the prevalence and distribution patterns of sesamoid bones at all the MTP joints [Table 4]. We found no correlation between the hallux and any other MTP joints of the foot as the sesamoid bone is consistently present at the hallux and seems to exist independently. We observed a positive correlation between the presence of sesamoid bones at any two of the other four MTP joints
(p < 0.001) [Table 4]. These results also confirm that in the absence of sesamoid bone at the first MTP joint, sesamoid bones are unlikely to occur at other MTP joints.
Discussion
To the best of our knowledge, our study is the first to report the prevalence, distribution patterns, and coexistence of foot sesamoid bones in Oman. The overall prevalence of sesamoid bones at first MTP joint was 100%, which is consistent with previous findings.6–10 All sesamoid bones were found on the plantar surface. Similar to other reports in the literature, in the majority of radiographs (99.6%) at least two sesamoid bones (medial sesamoid and lateral sesamoid) found at this joint.6–10 However, in three (0.4%) cases , there was only one bone found at the lateral side tendon of the hallux. Partitioning of the sesamoids at the first MTP has been frequently reported. Generally, a partition is seen on the medial sesamoid bone due to the high weight-bearing load on the medial side tendon of the flexor hallucis brevis. The reported prevalence of partitioning varies from 7.8–33%. Among the reported cases of partitioned sesamoid bones, bilateral involvement seems to occur between 13.5–90%.18 Furthermore, partitioned sesamoids at hallux tendons may undergo or simulate fractures.12 The prevalence of bipartite hallux sesamoid bones observed in Omani subjects is much lower than in Americans (16%) and Europeans (12.7%), but slightly higher than those in Middle Eastern populations (3%).3 Though the frequency of partition of sesamoids is low in Omani subjects (5.2%), it should be considered during the differential diagnosis of sesamoid bone fractures.
A recently reported systematic review found a pooled prevalence estimate of 22.4% at IP joints of the great toe.3 However, a higher prevalence of 71.6% was noted in cadaveric studies. In radiological studies, it varied between 2.3%–68%. When different ethnic groups were considered, the prevalence varied considerably. In Far Eastern, European, and African populations, it was 83%, 4.4%, and 0.07%, respectively.3 In our study, the observed prevalence at this joint is relatively high (9.9%) when compared to that of other Middle Eastern populations such as Bahrain (3.9%)10 and Turkey (2%).8
At the fifth MTP joint, a prevalence rate of 5.5–10% was reported in Caucasians,6 10.8% in Africans,6 and 11.6% in Bahrainis.10 The prevalence reported in our study is closer to that of Bahraini Arabs. Surprisingly, the presence of two sesamoid bones was also reported at this joint. Similar to Bahraini Arabs, 26 (3.4%) subjects in our study had two sesamoid bones in the little toe. The presence of sesamoid bones at the little toe may be one of the causes of lateral foot pain. Generally, weight-bearing force on the little toe may cause discomfort leading to lateral forefoot pain or even fractures. The presence of two sesamoid bones at the little toe, as seen in some of our subjects, is less likely to result in lateral foot pain. This could be explained based on the fact that the two bones could probably distribute the weight evenly, which may reduce their risk of injury.
In previous studies, the reported prevalence of sesamoid bones at the second, third, and fourth MTP joints is much lower when compared to that of the first and fifth MTP joints.1,6,8,10,19–21 Sesamoid bones were rarely found in the second, third, and fourth MTP joints. The observed prevalence rate in Omani subjects at these joints is comparable with the other studied populations across the world [Table 5]. Similar to previous studies, no statistically significant gender association was found with regard to the presence or absence of sesamoid bones at all forefoot joints.6–10 Age could be one of the independent factors that influence the sesamoid bone prevalence as the ossification process extends through adulthood. The onset of sesamoid bones ossification usually occurs before age 20.7 Evidence suggests that ossification of first MTP joint sesamoid bones usually occurs at eight years old in females and 9–11 years old in males.10,13 However, the ossification timeline of sesamoids at the other MTP joints is yet to be studied. A recent study on Chinese subjects observed a weak but significant association between the age and presence of sesamoid bones.7 Contrary to these results, we found a positive association only at the fifth MTP joint. A sample size difference between the two studies could be one of the possible reasons for these contradictory results. However, further research is required to explore the ossification timeline of sesamoid bones at other MTP joints.
We identified nine typical distribution patterns of sesamoid bones among the MTP joints. Very few studies have documented the various distribution patterns of sesamoid bones and their coexistence.7,8 Our study is the first to report the coexistence of sesamoid bones across the MTP joints in Arab populations. Omani subjects showed a relatively high proportion of the coexistence of sesamoid bones (14.6%) compared to Chinese subjects (10.9%). In our study, we noted only six distinctive patterns compared to 16 distinctive patterns seen in the Chinese study.7 These results indicate that Omani subjects are more likely to have sesamoid bones at two or more MTP joints, particularly at first and fifth MTP joints. However, we did not find the coexistence of sesamoid bones across all MTP joints though previous studies reported it.3,7 Our results confirm the previously reported evidence of coincidental development of sesamoid bones at the MTP joints.7 It has been postulated that genetic factors and local mechanical stress influence the development of specific patterns of sesamoid bones.22,23 In experimental mice, mutations in Hox genes, homeotic genes, growth factor 5, and bone morphogenetic protein 5 have resulted in altered development of sesamoid bones.24,25 In a recent study, it has been shown that sesamoid bones develop from sry-type HMG box 9+ (Sox9+)/scleraxis (Scx+) progenitors independently of mechanical stimuli from muscles. Furthermore, these progenitors depend on transforming growth factor beta (TGF-b) and bone morphogenetic protein 2 (BMP2) signaling and interaction between BMP4 and BMP2 signaling for their specification, growth, and differentiation.26 Based on these evidences, we propose that a high frequency of coincidence of sesamoid bones at first and fifth MTP joints in Omani subjects could be attributed to genetic factors. Since the tendency of specific distribution patterns of sesamoid bones development increases the risk of pathological changes in the forefoot, more research exploring the genetic and epigenetic factor involvement on coincidental development of sesamoid bones at MTP joints is warranted.
Conclusion
The results of our study provide baseline data that could be helpful for clinicians and musculoskeletal radiologists in particular, to consider ailments of sesamoid bones during differential diagnosis in Omani patients who present with foot pain or discomfort.
Disclosure
The authors declared no conflicts of interest. No funding was received for this study.
references
- 1. Bizarro AH. On sesamoid and supernumerary bones of the limbs. J Anat 1921 Jul;55(Pt 4):256-268.
- 2. Vickaryous MK, Olson WM. Sesamoids and ossicles in the appendicular skeleton. In: Hall BK, editor. Fins into Limbs. Evolution, Development, and Transformation. University of Chicago Press; 2007. p. 323-341.
- 3. Yammine K. The sesamoids of the feet in humans: a systematic review and meta-analysis. Anat Sci Int 2015 Jun;90(3):144-160.
- 4. Coughlin MJ. Sesamoid and accessory bones of the foot. In: Surgery of the foot and ankle. 8th ed. Elsevier, Amsterdam; 2006. p. 438-494.
- 5. Anwar R, Anjum SN, Nicholl JE. Sesamoids of the foot. Curr Orthop 2005;19(1):40-48.
- 6. Msamati BC, Igbigbi PS. Radiographic appearance of sesamoid bones in the hands and feet of Malawian subjects. Clin Anat 2001 Jul;14(4):248-253.
- 7. Sun T, Zhao H, Wang L, Wu W, Hu W. Distribution patterns and coincidence of sesamoid bones at metatarsophalangeal joints. Surg Radiol Anat 2017 Apr;39(4):427-432.
- 8. Coskun N, Yuksel M, Cevener M, Arican RY, Ozdemir H, Bircan O, et al. Incidence of accessory ossicles and sesamoid bones in the feet: a radiographic study of the Turkish subjects. Surg Radiol Anat 2009 Jan;31(1):19-24.
- 9. Kiter E, Akkaya S, Kiliç BA, Demirkan F. Distribution of the metatarsophalangeal sesamoids in Turkish subjects. J Am Podiatr Med Assoc 2006 Sep-Oct;96(5):437-441.
- 10. Dharap AS, Al-Hashimi H, Kassab S, Abu-Hijleh MF. Incidence and ossification of sesamoid bones in the hands and feet: a radiographic study in an Arab population. Clin Anat 2007 May;20(4):416-423.
- 11. Nwawka OK, Hayashi D, Diaz LE, Goud AR, Arndt WF III, Roemer FW, et al. Sesamoids and accessory ossicles of the foot: anatomical variability and related pathology. Insights Imaging 2013 Oct;4(5):581-593.
- 12. Mellado JM, Ramos A, Salvado E, Camins A, Danus M, Sauri A. Accessory ossicles and sesamoid bones of the ankle and foot: imaging findings, clinical significance and differential diagnosis. Eur Radiol 2003 Dec;13(6):L164-L177.
- 13. Miller TT. Painful accessory bones of the foot. Semin Musculoskelet Radiol 2002 Jun;6(2):153-161.
- 14. Sims AL, Kurup HV. Painful sesamoid of the great toe. World J Orthop 2014 Apr;5(2):146-150.
- 15. Blundell CM, Nicholson P, Blackney MW. Percutaneous screw fixation for fractures of the sesamoid bones of the hallux. J Bone Joint Surg Br 2002 Nov;84(8):1138-1141.
- 16. Richardson EG. Hallucal sesamoid pain: causes and surgical treatment. J Am Acad Orthop Surg 1999 Jul-Aug;7(4):270-278.
- 17. Apley AG. Open sesamoid. A re-appraisal of the medial sesamoid of the hallux. Proc R Soc Med 1966 Feb;59(2):120-121.
- 18. Sarin VK, Carter DR. Mechanobiology and joint conformity regulate endochondral ossification of sesamoids. J Orthop Res 2000 Sep;18(5):706-712.
- 19. Pfitzner. Morphologischearbeiten de Schwalbe. 1892. Cited from Bizarro 1921.
- 20. Sun T, Wang L, Zhao H, Wu W, Hu W. Prevalence, morphological variation and ossification of sesamoid bones of the forefoot: a retrospective radiographic study of 8,716 Chinese subjects. J Clin Transl Res 2016 Aug;2(3):91-96.
- 21. Koo BS, Song Y, Lee S, Sung YK, Sung IH, Jun JB. Prevalence and distribution of sesamoid bones and accessory ossicles of the foot as determined by digital tomosynthesis. Clin Anat 2017 Nov;30(8):1072-1076.
- 22. Hall BK. Bones and cartilage: developmental and evolutionary skeletal biology. Elsevier; 2005.
- 23. Berthaume MA, Bull AM. Human biological variation in sesamoid bone prevalence: the curious case of the fabella. J Anat 2020;236(2):228-242.
- 24. Small KM, Potter SS. Homeotic transformations and limb defects in Hox A11 mutant mice. Genes Dev 1993 Dec;7(12A):2318-2328.
- 25. Storm EE, Kingsley DM. Joint patterning defects caused by single and double mutations in members of the bone morphogenetic protein (BMP) family. Development 1996 Dec;122(12):3969-3979.
- 26. Eyal S, Rubin S, Krief S, Levin L, Zelzer E. Common cellular origin and diverging developmental programs for different sesamoid bones. Development 2019 Feb;146(4):dev167452.