|
Introduction
Chronic disease burdens on society are expected to rise in the future, alongside the increasing and aging population. Osteoarthritis (OA) is common among the elderly, with a global impact; ranks fourth among medical problems in women and risk factors associated with it are many.1-3 Risk factors such as age, sex, trauma, overuse, genetics, and obesity can each make contributions to the process of injury in different compartments of the joint.4 Co-morbid conditions and other enabling factors such as depression; low educational level; and poor socioeconomic status are component risks.5,6 The risk for osteoarthritis only becomes apparent at age 40 years and above.7 These risk factors contribute to the progressive nature of the disease which serves as targets of behavioral and pharmacologic interventions.
Among the multiple physio-pathological mechanisms involved in osteoarthritis, those related to sex hormone, in particular those involving estrogens,8 fulfill a relevant role in maintaining the homeostasis of articular tissues and, hence, of the joint itself. There is a dramatic rise in osteoarthritis prevalence among postmenopausal women,9,10
Persons who are overweight have a high prevalence of knee osteoarthritis. For many years, it was not clear whether being overweight preceded or was a consequence of osteoarthritis, given the immobility and disability the disease can produce. Recent studies have proved that being overweight antedates the development of the disease.11,12 Furthermore, in persons with osteoarthritis, being overweight increases the risk for radiographic progression.13,14 In most but not all studies, the increased risk for osteoarthritis of the knee among overweight persons is stronger in women than men.
Osteoarthritis of the knee and hip may be associated with different risk factors, suggesting that they should be regarded as unique diseases.15 Osteoarthritis in the weight-bearing joints (knees and hips) has a great clinical impact. Generalized osteoarthritis may be a distinct disease;16 although many of the same pathologic changes of the disease occur in the back and neck, it is not clear whether clinical syndromes of back and neck pain is necessarily related to osteoarthritis. Osteoarthritis of small joints of hands and feet in isolation are less frequent.
During the summer of 2010, students of public health program, college of health sciences, Kingdom of Bahrain, carried out this study adjoining community service. It was intended: to motivate, sensitize and train public health students to conduct a public health survey; correlate the proven risk factors of osteoarthritis in the study population and to identify modifiable risk factors for health promotion, thus contributing to the public health policy in Bahrain.
Methods
Feasibility of the study and pre-testing of the questionnaire was carried out at Naeem health center, Bahrain. Pre-testing of the questionnaire was done on small sample (n=30) of patients in the presence of two physicians and necessary changes to the questionnaire were made before beginning the study.
Broadly, the questionnaire had two sections: 1) The personal information which included CPR Number; Age; Height and Weight for BMI calculation; marital status and number of Children; Employment status with type of employment and hours of standing during employment; physical activity: household, walking, treadmill and other. 2) The clinical information which included status of menopause, years since menopause, hormone replacement therapy status; Information on fractures, accidents; Diagnosis of OA clinical/radiological; types of OA: knee and hip-OA of major joints; 3 or more joints or group of joints, commonly occurring in spine, knees, hips, base of the thumb, big toe, tips of the fingers - generalized OA; joints of hands and feet- OA of small joints ; Treatment of OA medical, surgical, details of surgery and details on joint replacement; how long on medical and nonmedical treatment including physiotherapy; and status of chronic morbidities (diabetes, hypertension, hypercholesterolemia), as well as information on family history of OA.
Ten different health centers, assigned randomly and a tertiary care center (Salmanya Hospital) of the ministry of health were the study sites, during June and July of 2010. Two/Three students constituted a team in each of the health center/hospital.
By convenient sampling, female residents of Bahrain, aged above 40 years, who are physician-diagnosed of primary osteoarthritis with the clinical/ radiological criteria, undergoing treatment in the health centers of Bahrain, were interviewed. Patients who were not ambulatory and diagnosed of secondary osteoarthritis were not included. Participation in the study was voluntary and anonymous. The purpose of the study and questions were explained in Arabic and informed consent was obtained from all participants.
Classification of osteoarthritis was based on previous reports.15,16, Briefly, osteoarthritis of the knee and hip was considered as the osteoarthritis of the major joints; generalized osteoarthritis was characterized by involvement of 3 or more joints or group of joints, commonly occurring in the spine, knees, hips, base of the thumb, big toe, tips of the fingers; osteoarthritis of the small joints consisted of joints of hands and feet. We adopted the WHO criteria,17 for body mass index (BMI) classification for the weight and height measurements. Co-morbidities of diabetes, hypertension and hypercholesterolemia were based on history of diagnosis.
Data from the questionnaire were coded and captured in Excel (Microsoft, Redmond, WA,USA) exported to SPSS. Version 18.0.0 (SPSSInc. Chicago, IL) for analysis. Additionally EpiInfo. Version.3.5.3 (CDC, Atlanta, GA) and OpenEpi.Version 2.3.1 (Emory University, Atlanta, GA) were employed. Multivariate analysis of ordinal regression followed univariate analysis.
Results
Of the 420 cases of osteoarthritis (response rate of 100%) who were interviewed in the study, 22 cases had to be excluded from the
study owing to incomplete information, leaving 398 (95%) cases for analysis.
Muharraq health center returned the maximum number of cases of 65 (16.3%) followed by Salmanya hospital with 58 cases and the least number of cases (n=15; 3.8%) were contributed by health centers of A’Ali, Kanoo and National Bank of Bahrain (Fig. 1). The age distribution in the study was normal (range: 40-85) with a mean age of 57 and most cases (n=154; 39%) were from the age group of 50-59.
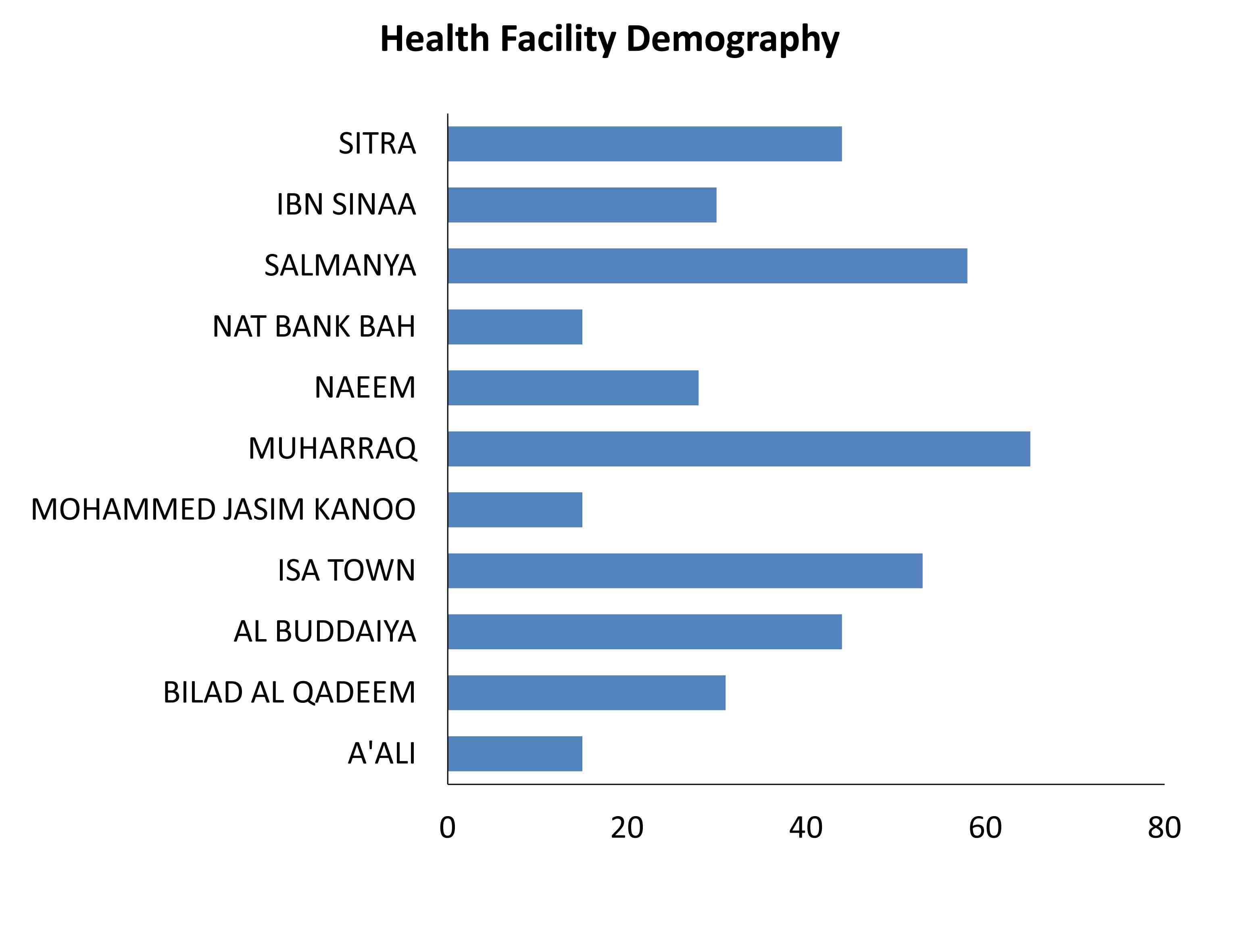
Figure 1: Health Facility Demography.
Osteoarthritis of major joints alone accounted for 293 (74%) cases; generalized osteoarthritis accounted for 84 (21%) and osteoarthritis of small joints of hands and feet accounted for 21 (5%) cases. Among the types of major osteoarthritis: osteoarthritis of the knee was 135 (47%); osteoarthritis of the hip was just 7 (2%) and osteoarthritis of knee and hip together was 151 (51%). Among
the 21 cases of osteoarthritis of smaller joints: osteoarthritis of the hands was 6 (29%); osteoarthritis of feet was 2 (9%) and osteoarthritis of both hands and feet together was 13 (62%).
There were no chronic morbidities among 120 (29%) of the cases; whereas 43% had a combination of co-morbidities. History of diagnosed: diabetes was found in 10% of cases, hypertension among 13% and hypercholesterolemia in 5% of cases. Half (142) of the cases in the study were obese and 30% (89) were overweight. Osteoarthritis of the knee (76) and the combination of the osteoarthritis of knee and hip (64) was highest among obese followed by overweight cases. (Table 1)
Table 1: Cross tabulation of major osteoarthritis types and BMI groups, Bahrain, 2010.

Table 2: Multivariate Ordinal Regression Analyses of Risk Factors for osteoarthritis among women, Bahrain, 2010.
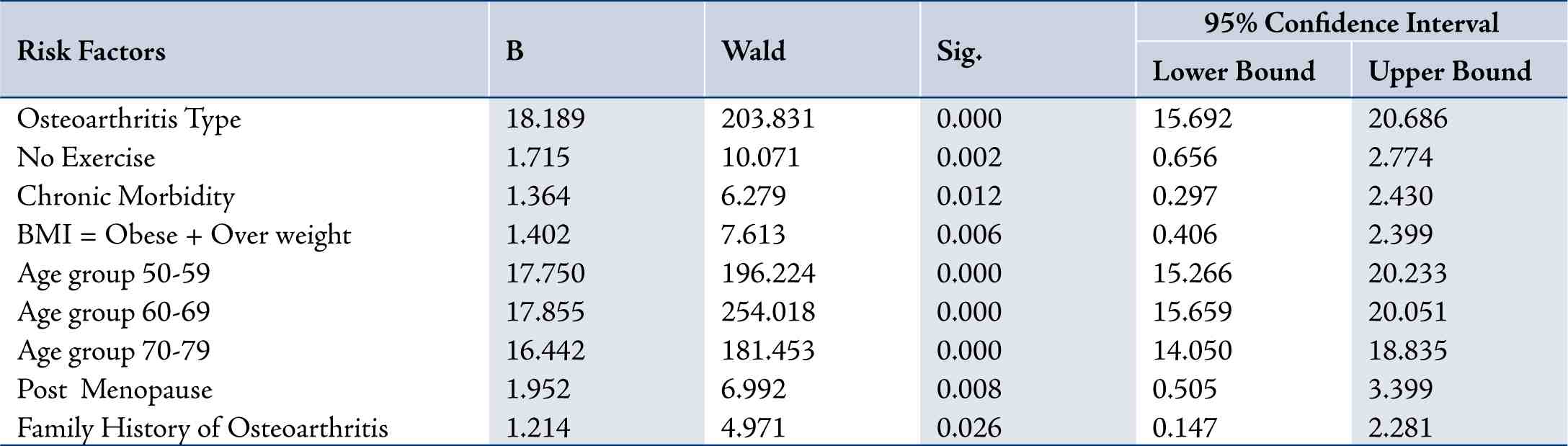
Link function: Logit. Nagelkerke pseudo R square = 0.293
Independent risk factors are shown. Risk factors which are not statistically significant in multivariate analysis are not depicted. B denotes parameter estimate of each variable in ordinal regression model. Wald denotes importance of each factor.
Only 65 cases, 16% stated that they do exercise. Menopause was found among 272 (68%). The median duration of illness was 4 yrs with a range of 35 yrs (Min: 1 yr; Max: 36 yrs); 85% of the patients were on medication; 75% were on Physiotherapy. Only 23 (6%) had their joints replaced. Over 90% (363) of the cases were less educated (less than or equal to Intermediate level) compared to educated to secondary level or more. Odds Ratio for being housewife was 3.085 (95%; CI: 1.75-5.43). Family history of osteoarthritis was 219 (55%) in the sample.
The multivariate analysis of ordinal regression using “Logit” link function with location component returned pseudo R2 (Nagelkerke) of 30% for the model (Table 2). Variables included in the model were age, BMI, menopause status, exercise, chronic morbidities and family history of osteoarthritis. The goodness of fit for pearson’s chi square and deviance was not significant.
Discussion
Non communicable diseases are on the rise, moving along the trend of epidemiological transition. Prevalence of chronic diseases among Arab women is increasing and mainly linked to obesity.7 Osteoarthritis is not only the most common multi-factorial non communicable disease, but also the most prevalent form of arthritis among women and the elderly, causing physical disability and impaired quality of life. Available treatment strategies are focused at reducing pain and improving joint function. This study was necessitated for a situational analysis - first in Bahrain - on osteoarthritis among women above the age of 40, and to explore an enhanced scope for health promotion on modifiable risk factors as a primary preventive strategy. Further, the students of public health program of the college of health sciences have learned the art of interviewing and realized the gravity of community survey.
Our results demonstrate and support previous study findings on the risk factors for osteoarthritis. Higher BMI, advancing age, sedentary life style, estrogen insufficiency, genetic predisposition and chronic morbidities were the risk factors uniquely identified by this study among Bahraini women above 40 years of age. (Table 2)
Many cross sectional and longitudinal studies have established the association between obesity and osteoarthritis.18-22 The Arab women study,7 has identified that at age 40-49 years ,obese women had twice the risk for osteoarthritis than non-obese women and then the risk turns four-fold at age 50 years and above. The National non-communicable diseases risk factor (NNCD) survey of Bahrain,23 and our study had many similarities: Obesity in our study was close to 50% and the NNCD survey showed 40% among females in general; while overweight in females was very similar and around 30% both in our study and the NNCD survey. Although the NNCD did not explore osteoarthritis; comparable results prevailed between BMIs in both the study group and NNCD sample; our study sample represents the population as that of NNCD. Predominantly, osteoarthritis of the knee was close to 50% in our study and was similar in the general population as reported by Felson and Zhang.24 Osteoarthritis of the weight bearing joints in our study was: major osteoarthritis three fourths and the generalized osteoarthritis which often included osteoarthritis of weight bearing joints was one fifths. Notably, our study found increasing trend on higher BMI with osteoarthritis of the weight bearing joints, indicating obesity as a major modifiable risk factor.
Studies in both developed and developing countries have shown the prevalence of hypertension, diabetes, obesity and osteoarthritis interlinked.25 Whereas, less similarities were noticed between our study and NNCD survey in the history of diagnosed diseases like: diabetes was 10% in our study and 13% in all female sex according the NNCD survey; hypercholesterolemia was 5% in our study and it was 40% in all female sex by NNCD survey; hypertension among 13% in our study and 19% in all female sex by NNCD survey. Lower prevalence rates of diabetes, hypertension and hypercholesterolemia in our study sample need not be construed as a lower risk for osteoarthritis. It is still a risk for osteoarthritis according to our findings from the multivariate ordinal regression model. Possibly, this low prevalence is due to monitoring and controlling the parameters by the study patients as their visits to health centers/hospital are frequent due to osteoarthritis.
Half of the study patients had a family history of osteoarthritis recognizing NIH conference report,26 that all heterogeneous forms of osteoarthritis are genetically determined and likely that most genes affecting osteoarthritis will cause disease in many joints.
Two thirds of the study participants were post-menopausal suggesting that estrogen insufficiency plays a role in causing osteoarthritis as has been reported by Felson et al.26 Majority of the patients were on medication and physiotherapy; thus doing regular exercise was uncommon. Joint replacement in the study was very low. The bulk of the cases were less educated and staying at home.
This study had few limitations, which is not uncommon in any cross sectional study. Pregnant women, non ambulatory cases and cases of osteoarthritis who have not sought treatment other than ministry of health facility were not interviewed. Cases from households were not included in the study owing to socio-cultural factors. Although, the questionnaire was pre-tested and found satisfied before beginning the study, there would have been some errors in patient responses compared to medical records, due to low recall which is not uncommon in any study of this nature.
Conclusion
Despite these limitations, this study has underlined the increasing trends of non-communicable diseases moving along the epidemiological transition. Proportion of major osteoarthritis is very high, predominantly knee osteoarthritis, and combination of hip and knee osteoarthritis of the weight bearing joints. The modifiable risk factors for health promotion identified from this study are sedentary lifestyle, obesity and overweight and chronic morbidities of diabetes, cholesterol and hypertension. In order to achieve this, we need a joint effort for the diseases of the joints at all levels.
Acknowledgements
We are grateful to all the participants in the study, DR. Mariam A Al Jalahima-Assistant under secretary of primary care and public health, Dr. Fawzi A Ameen- Assistant undersecretary of training and planning, physicians and staff of ministry of health facilities. We thank Dr. Shawqi A Ameen-Chairamn, National Health Regulatory Authority; Dr. Aneesa Mohammed Al Sindi-Dean; Mrs. Raja Radhi Al-Qumaish-Chairperson, Allied Health Division; Dr. Wedad Al Banna-student counselor and Dr. Mahmood Alawi Al-Gallaf-Chairperson research committee of College of Health Sciences for their support in the study.
References
1. Al-Arfaj A, Al-Boukai AA. Prevalence of radiographic knee osteoarthritis in Saudi Arabia. Clin Rheumatol 2002 May;21(2):142-145.
2. Aspden RM, Scheven BA, Hutchison JD. Osteoarthritis as a systemic disorder including stromal cell differentiation and lipid metabolism. Lancet 2001 Apr;357(9262):1118-1120.
3. Al-Shammari S, Khoja T, Alballa S, Kremlin M, Charles ST. Obesity and clinical osteoarthritis of the knee in primary healthcare. Med Sci Res 1995;23:255-256.
4. Abramson SB, Attur M. Developments in the scientific understanding of osteoarthritis. Arthritis Res Ther 2009;11(3):227.
5. Fries JF. Exercise and the health of the elderly. Am J Geriatr Cardiol 1997 May;6(3):24-32.
6. Vita AJ, Terry RB, Hubert HB, Fries JF. Aging, health risks, and cumulative disability. N Engl J Med 1998 Apr;338(15):1035-1041.
7. Abdulrahman O. Musaiger and Nora E. Shahbeek. The relationship between obesity and prevalence of chronic diseases in the Arab women. Chapter 13.Human Ecology special issue No.13:97-100(2005)
8. Gokhale JA, Frenkel SR, Dicesare PE. Estrogen and osteoarthritis. Am J Orthop (Belle Mead NJ) 2004 Feb;33(2):71-80.
9. Srikanth VK, Fryer JL, Zhai G, Winzenberg TM, Hosmer D, Jones G. A meta-analysis of sex differences prevalence, incidence and severity of osteoarthritis. Osteoarthritis Cartilage 2005 Sep;13(9):769-781.
10. Lawrence RC, Helmick CG, Arnett FC, Deyo RA, Felson DT, Giannini EH, et al. Estimates of the prevalence of arthritis and selected musculoskeletal disorders in the United States. Arthritis Rheum 1998 May;41(5):778-799.
11. Manninen P, Riihimäki H, Heliövaara M, Mäkelä P. Overweight, gender and knee osteoarthritis. Int J Obes Relat Metab Disord 1996 Jun;20(6):595-597.
12. Felson DT, Zhang Y, Hannan MT, Naimark A, Weissman B, Aliabadi P, et al. Risk factors for incident radiographic knee osteoarthritis in the elderly: the Framingham Study. Arthritis Rheum 1997 Apr;40(4):728-733.
13. Dougados M, Gueguen A, Nguyen M, Thiesce A, Listrat VV, Jacob L, et al. Longitudinal radiologic evaluation of osteoarthritis of the knee. J Rheumatol 1992 Mar;19(3):378-384.
14. Schouten JS, van den Ouweland FA, Valkenburg HA. A 12 year follow up study in the general population on prognostic factors of cartilage loss in osteoarthritis of the knee. Ann Rheum Dis 1992 Aug;51(8):932-937.
15. Felson D. The epidemiology of osteoarthritis: prevalence and risk factors. In: Kuettner KE, Goldberg VM, eds. Osteoarthritic Disorders. Rosemont, IL: American Academy of Orthopaedic Surgeons; 1995:13-24.
16. Kellgren JH, Moore R. Generalized osteoarthritis and Heberden’s nodes. Br Med J 1952 Jan;1(4751):181-187.
17. BMI classification. Available at: http://apps.who.int/bmi/index. jsp?introPage=intro_3.html
18. Hochberg MC, Lethbridge-Cejku M, Scott WW Jr, Reichle R, Plato CC, Tobin JD. The association of body weight, body fatness and body fat distribution with osteoarthritis of the knee: data from the Baltimore Longitudinal Study of Aging. J Rheumatol 1995 Mar;22(3):488-493.
19. van Saase JL, Vandenbroucke JP, van Romunde LK, Valkenburg HA. Osteoarthritis and obesity in the general population. A relationship calling for an explanation. J Rheumatol 1988 Jul;15(7):1152-1158.
20. Hart DJ, Doyle DV, Spector TD. Association between metabolic factors and knee osteoarthritis in women: the Chingford Study. J Rheumatol 1995 Jun;22(6):1118-1123.
21. Schouten JS, van den Ouweland FA, Valkenburg HA. A 12 year follow up study in the general population on prognostic factors of cartilage loss in osteoarthritis of the knee. Ann Rheum Dis 1992 Aug;51(8):932-937.
22. Martin K, Lethbridge-Cejku M, Muller DC, Elahi D, Andres R, Tobin JD, et al. Metabolic correlates of obesity and radiographic features of knee osteoarthritis: data from the Baltimore Longitudinal Study of Aging. J Rheumatol 1997 Apr;24(4):702-707.
23. National Non-communicable Diseases Risk Factors survey-2007. Available at http://intranet.health.gov.bh/Docs/Reports%20%20Studies/NCD%20 Survey%20 Report.pdf
24. Felson DT, Zhang Y. An update on the epidemiology of knee and hip osteoarthritis with a view to prevention. Arthritis Rheum 1998
Aug;41(8):1343-1355.
25. World Health Organization. obesity: prevention and managing the global epidemic. WHO, Geneva (2000).
26. Felson DT, Lawrence RC, Dieppe PA, Hirsch R, Helmick CG, Jordan JM, et al. Osteoarthritis: new insights. Part 1: the disease and its risk factors. Ann Intern Med 2000 Oct;133(8):635-646.
|