A three-year-old male patient was brought to the emergency room due to elbow pain and limited range of motion three days after having his left forearm suddenly pulled upward by his mother. Clinically, he presented pain during forearm pronosupination. After an unsuccessful closed reduction, radiographs [Figure 1] and magnetic resonance imaging (MRI) [Figure 2] were performed. Post-treatment MRI was also performed [Figure 3].
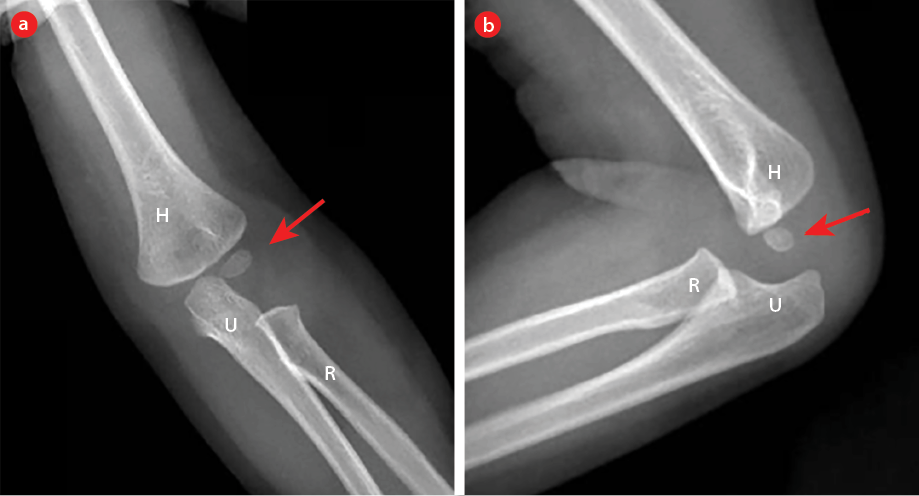 Figure 1: Elbow radiographs after failed closed reduction of the forearm. (a) Anteroposterior and (b) lateral views. There are no radiograph signs of fractures. The ossification center of the capitellum (red arrows) is normal and should not be interpreted as a fracture. H: humerus; U: ulna; R: radius.
Figure 1: Elbow radiographs after failed closed reduction of the forearm. (a) Anteroposterior and (b) lateral views. There are no radiograph signs of fractures. The ossification center of the capitellum (red arrows) is normal and should not be interpreted as a fracture. H: humerus; U: ulna; R: radius.
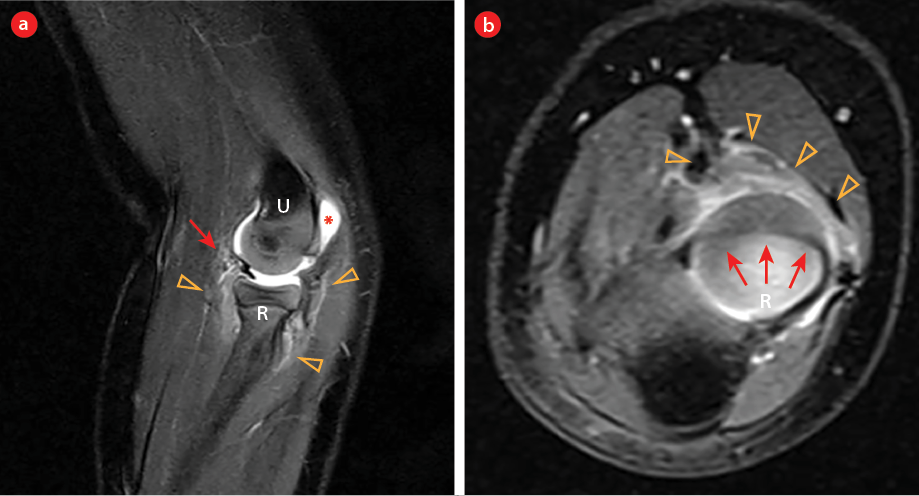 Figure 2: MRI Fat-Sat T2 weighted images of the elbow after failed closed reduction of the forearm show the annular ligament (red arrows) in the articular space: (a) sagittal and (b) axial views. Notice the areas of soft-tissue swelling (yellow arrowheads) and mild joint effusion (*). U: ulna; R: radius.
Figure 2: MRI Fat-Sat T2 weighted images of the elbow after failed closed reduction of the forearm show the annular ligament (red arrows) in the articular space: (a) sagittal and (b) axial views. Notice the areas of soft-tissue swelling (yellow arrowheads) and mild joint effusion (*). U: ulna; R: radius.
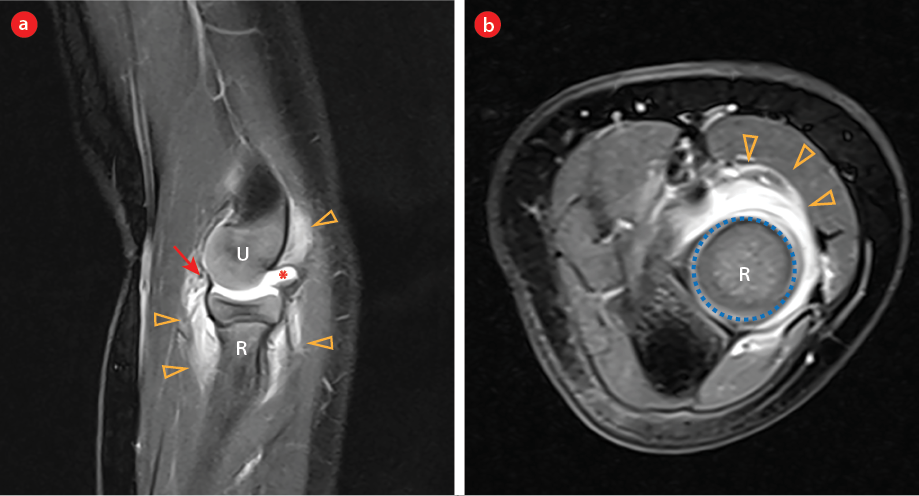 Figure 3: MRI Fat-Sat T2 weighted images of the elbow after successful closed reduction of the forearm. (a) The sagittal view shows the annular ligament in its normal position (red arrow). (b) In the axial view, notice the clear articular surface of the radius (dotted circle) without ligament entrapment. The areas of soft-tissue swelling (yellow arrowheads) and mild joint effusion (*) persist. U: ulna; R: radius.
Figure 3: MRI Fat-Sat T2 weighted images of the elbow after successful closed reduction of the forearm. (a) The sagittal view shows the annular ligament in its normal position (red arrow). (b) In the axial view, notice the clear articular surface of the radius (dotted circle) without ligament entrapment. The areas of soft-tissue swelling (yellow arrowheads) and mild joint effusion (*) persist. U: ulna; R: radius.
Questions
- What is the diagnosis?
- Was the MRI well indicated?
Answers
- Pulled elbow.
- Yes, MRI should be performed if a closed reduction of the elbow fails.
Discussion
Pulled elbow was suspected in the emergency room. The following closed reduction of the elbow was unsuccessful. Elbow radiographs did not show any abnormality [Figure 1]. Subsequent MRI confirmed the clinical hypothesis and showed the annular ligament interposed in the radiocapitellar joint [Figure 2]. Soft-tissue swelling and joint effusion were also noted [Figure 2]. A second reduction was performed, and a new MRI confirmed that the annular ligament was in its usual
topography [Figure 3].
Trauma is the most common cause of morbidity and mortality in the population < 19 years and the forearm is the main site of fractures in this population.1 Pulled elbow, also known as radial head subluxation or nursemaid’s elbow, is the most prevalent traumatic elbow injury in children under five, representing approximately 20% of upper extremity conditions.2,3 It is defined by interposing the annular ligament over the head of the radius and the humerus into the joint space, where it becomes entrapped.4 This entity usually occurs in situations in which children are abruptly picked up from the floor, lifted, or swung by the hand.5,6 The radial head then slips distally beneath the annular ligament, which is partially torn from the radial neck.4
The trapped ligament leads to a typical clinical condition in which the child holds the affected arm in pronation, refusing to move it due to pain.2,4 A well-defined and typical history associated with the classic clinical presentation is sufficient for diagnosis in most cases. Radiographic examination is often unremarkable.5 Elbow radiographs should be taken to rule out fractures, especially of the supracondylar humerus. It is important to note the ossification centers of the elbow [Figure 1], which may be misinterpreted as a fracture in the context of trauma.2 However, elbow radiographs should be taken to rule out fractures, especially of the supracondylar humerus.4 Sonography has an important role in assessing the musculoskeletal system, markedly in the pediatric population, as it does not involve radiation and is a noninvasive imaging modality.7 Ultrasound may detect limited radial head rotation during pronation and supination as well as characterize a torn or displaced annular ligament. However, sonography accuracy for the pulled elbow diagnosis is unknown, and its operator-dependence is a major disadvantage.6,7 MRI should be performed when the clinical history is unclear or when the reduction is unsuccessful.2,5 MRI may show dislocation and rupture of the annular ligament and damage to the synovial membrane of the elbow joint. Soft parts swelling and joint effusion are common associated findings related to the trauma itself.3
There are two standard methods of closed reduction for pulled elbow treatment: flexion and supination or forced pronation of the affected arm.2 A characteristic palpable click generally accompanies successful treatment.4 Recurrence rates are estimated between 5% and 39% of the patients.6
Disclosure
The authors declared no conflicts of interest. Consent was obtained from the patient’s parents.
references
- 1. Elhusseiny K, El-Sobky TA. Imaging pitfalls of the acutely traumatized pediatric elbow. Oman Med J 2018 Sep;33(5):444-446.
- 2. Park K, Kim TE, Cho YH, Yi JH. MRI of spontaneous reduction of an entrapped annular ligament in an atypical pulled elbow patient: a case report. J Korean Soc Radiol 2014;70(6):444-447.
- 3. Mak S, Beltran LS, Bencardino J, Orr J, Jazrawi L, Cerezal L, et al. MRI of the annular ligament of the elbow: review of anatomic considerations and pathologic findings in patients with posterolateral elbow instability. AJR Am J Roentgenol 2014 Dec;203(6):1272-1279.
- 4. Eismann EA, Cosco ED, Wall EJ. Absence of radiographic abnormalities in nursemaid’s elbows. J Pediatr Orthop 2014 Jun;34(4):426-431.
- 5. Diab HS, Hamed MM, Allam Y. Obscure pathology of pulled elbow: dynamic high-resolution ultrasound-assisted classification. J Child Orthop 2010 Dec;4(6):539-543.
- 6. Dhar D, Varghese T. Audit of inpatient management and outcome of limb fractures in children. Oman Med J 2011 Mar;26(2):131-135.
- 7. Razek AA, Fouda NS, Elmetwaley N, Elbogdady E. Sonography of the knee joint. J Ultrasound 2009 Jun;12(2):53-60.