Thyroid cartilage, the largest structure in the larynx, features the superior cornu projecting upwards from its posterior part. It is an elongated narrow structure that curves upwards, backward, and medially.1 It is also the weakest part of the thyroid cartilage, making it susceptible to anatomical variations resulting from trauma and intubation. Patients with these variations often present with symptoms of odynophagia and foreign body sensations. We report a case of an asymptomatic medialized superior thyroid cornu caused by the mass effect of an associated thyroid lesion.
Case report
A 49-year-old man was referred to the otorhinolaryngology clinic for indirect laryngoscopy before thyroidectomy for a thyroid colloid nodule. He denied experiencing odynophagia, dysphagia, globus sensation, hoarseness, neck pain, intubation, or neck trauma before his presentation. On neck examination, there was a large anterior neck swelling with no tenderness. The mass had pushed the trachea toward the left. Flexible nasopharyngolaryngoscopy revealed a well-defined protruding mass originating from the right lateral laryngopharyngeal wall. The mass was covered by a smooth pharyngeal mucosa, without any irregularities or ulcerations [Figure 1]. Possible differential diagnoses for the protruding mass included a variant or dislocated superior cornu of the thyroid cartilage, fracture, or dislocation of the greater horn of the hyoid bone. Computed tomography (CT) scan images [Figure 2] with a 3D reconstruction [Figure 3] of the neck demonstrated a large well-defined cystic lesion measuring 6.6 × 8.2 × 9.8 cm in the right thyroid lobe that displaced the superior cornu of the thyroid cartilage medially. The length of the superior thyroid cornu measured 5 mm on the right side and 54 mm on the left side. The protrusion resulted from the mass effect of the huge thyroid mass, as an evident in the CT scan. The final histopathology report of the thyroid mass confirmed nodular hyperplasia with cystic degeneration. Post-thyroidectomy, the patient remained asymptomatic. A follow-up scope revealed a reduced protrusion of the right superior thyroid cornu at the laryngopharynx. However, the patient refused surgical removal of the superior cornu of the thyroid cartilage and subsequently did not attend follow-up appointments.
 Figure 1: A well-defined, smooth surface protruding mass seen at the right laryngopharyngeal wall, at the level of epiglottis (black arrows).
Figure 1: A well-defined, smooth surface protruding mass seen at the right laryngopharyngeal wall, at the level of epiglottis (black arrows).
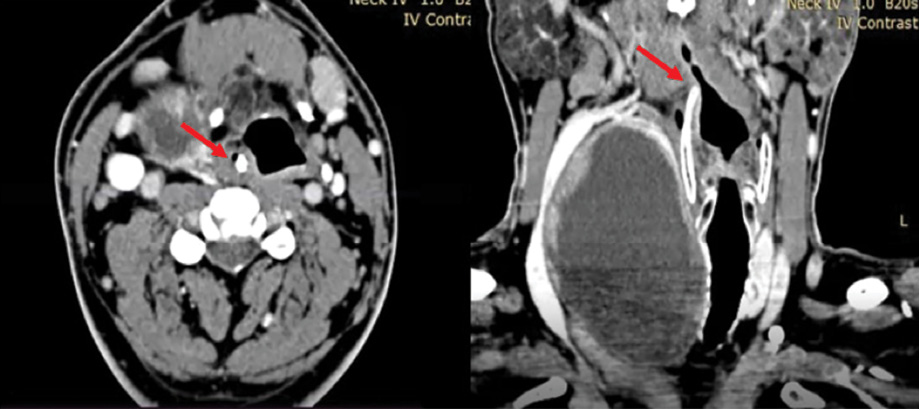 Figure 2: A neck CT scan from axial and coronal view showing a well-demarcated cystic lesion at the right thyroid lobe that pushed the larynx and trachea to the left superior (red arrows).
Figure 2: A neck CT scan from axial and coronal view showing a well-demarcated cystic lesion at the right thyroid lobe that pushed the larynx and trachea to the left superior (red arrows).
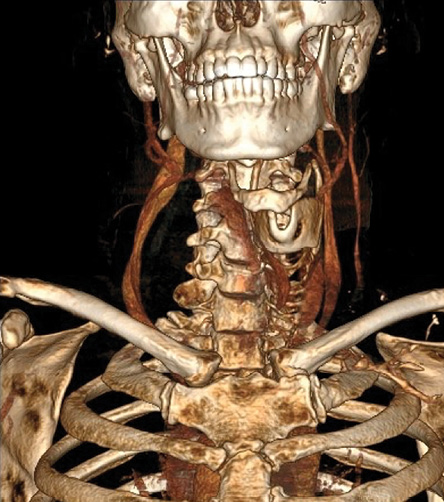 Figure 3: A 3D reconstruction CT scan revealed that the laryngeal framework was pushed to the
Figure 3: A 3D reconstruction CT scan revealed that the laryngeal framework was pushed to the
left side.
Discussion
The thyroid cartilage is the largest cartilage within the larynx and is one of the hyaline cartilages comprising the laryngeal framework, apart from the cricoid and arytenoid cartilages. It forms articulations with the greater cornu of the hyoid bone through the superior cornu and the lateral thyrohyoid ligament. Ossification of the thyroid cartilage typically begins around 18 to 20 years old, starting at the posterior aspect of the thyroid cartilage.2
The superior cornu of the thyroid cartilage is a long, narrow structure that curves upwards, backward, and medially, ending in a conical apex. Conversely, the inferior cornu is shorter, thicker, and curves downward and slightly anteromedially. The average length of the superior cornu, as determined by the dissection of 28 cadavers to determine the normal measurement of the laryngeal framework, is approximately 14.5 to 14.9 mm.3 However, it can elongate further, resulting in an abnormally long or medially displaced cornu.
The superior cornu is the weakest point in the thyroid cartilage. Traumatic events such as road traffic accidents, strangulation, traumatic intubation, and sports injury can lead to distortion of the thyrohyoid complex, resulting in the medial displacement of the contralateral superior cornu.4 In some cases, a congenital variant of the displaced superior cornu may exist in patients without any history of trauma, possibly due to abnormal development of the fourth brachial arch. However, it remains unclear why certain individuals become symptomatic at an older age.5
This patient denied any trauma to the larynx; however, he had a huge benign thyroid mass. The most plausible explanation for the anatomical variant of the right superior cornu in this patient is the mass effect exerted by the thyroid mass that pushes the right superior cornu, causing medial displacement of the right superior cornu. The CT scan revealed elongation of the right superior cornu, which further contributed to its indentation and medial protrusion. This is the first case report of an anatomical variant of superior thyroid cornu caused by a thyroid gland mass.
The variant anatomy of the thyroid cartilage, specifically the superior cornu, has been documented in the medical literature by Counter in 1980.1 Counter described a patient with superior thyroid cornu syndrome, characterized by the anatomical variant of the right superior cornu that passes posteriorly, instead of the normal variant which is vertical and detected during neck exploration. The patient is pain-free following a successful excision of the superior cornu.
Anatomical variations of the thyroid cartilage, whether congenital or acquired, may cause unpleasant symptoms and clinical challenges for patients and medical practitioners, particularly in airway management. Patients with the variant anatomy of the superior cornu often experience symptoms such as odynophagia, dysphagia, ear pain, baseline throat pain, globus sensation, clicking of the throat, constant choking, and throat clearing. A clinical case series of 12 patients documented that patients usually show these symptoms, with an average age of onset at 54.6 years and a range of 44 –58 years.6
Patients with a medially displaced or elongated superior horn of thyroid cornu may complain of globus sensation, odynophagia, and coughing, which may cause aspiration due to hindered food passage through the recessus piriformis. This can eventually result in the entry of food into the laryngeal inlet.5,7 Superior cornu of the thyroid that deviated medially and posteriorly may reach prevertebral fascia causing ulceration due to direct contact injury, and in some cases may even reach up to the arytenoid and trigger cough and pharyngeal reflex.8 Our patient was asymptomatic, and only presented to the otolaryngology clinic for preoperative evaluation of the vocal cord before thyroid surgery.
In patients undergoing intubation or general anesthesia, an anatomical variant of the superior cornu of the thyroid can pose difficulties or obstruct access to the larynx, potentially leading to intubation failure. Browning et al,9 described a case of failed intubation due to cornu abnormality. Fortunately our patient had no issues with intubation for the thyroid surgery, as an experienced anesthetist intubated him. The literature does not mention the association of difficult intubation due to the prominent superior thyroid cornu.
While a flexible endoscope is often a valuable tool for diagnosis, it may be helpful to proceed with a CT scan to confirm the diagnosis. CT scan with 3D reconstruction is useful in diagnosing patients with anatomical variations and in determining the relationships among the laryngeal structures.10
Although the condition is benign, it is important to explain and offer treatment options to symptomatic patients. The most common treatment is a local injection of steroids at the site of pain. Physical therapy, triamcinolone 40 mg injection, lidocaine 10 mg injection at the painful site, and surgical reduction via the transcervical approach of hyoid and thyroid cartilages are also potential treatment options.10 In Dewan et al's,10 case study on symptomatic patients, all patients had tried at least two treatments. It was found that 56% of the patients who underwent bilateral surgical reduction of hyoid and thyroid cartilages experienced complete resolution of anterior cervical pain symptoms within one month. On the other hand, those patients who opted for triamcinolone or lignocaine injections only experienced temporary relief of symptoms. However, the authors did not elaborate on the delivery method for the injections. There is a lack of data regarding the role of conservative versus surgical management for anterolateral cervical pain syndrome, as the study done by Dewan et al,10 had a small sample size, and no literature studies have investigated the effectiveness of conservative management. In the present case, since the patient was asymptomatic, he refused both medical and surgical intervention for the medialized superior thyroid cornu. He also defaulted on his clinic appointment post-thyroidectomy.
Conclusion
It is important to consider thyroid mass as a factor contributing to medialized superior thyroid cornu, in addition to known laryngeal trauma.
Disclosure
The authors declared no conflicts of interest. Informed consent was obtained from the patient.
Acknowledgments
We thank all the staff in the otorhinolaryngology and radiology departments at Queen Elizabeth Hospital, Sabah.
references
- 1. Counter RT. A superior thyroid cornu anomaly: a report of a case. J Laryngol Otol 1980 Sep;94(9):1087-1088.
- 2. Mupparapu M, Vuppalapati A. Detection of an early ossification of thyroid cartilage in an adolescent on a lateral cephalometric radiograph. Angle Orthod 2002 Dec;72(6):576-578.
- 3. Eckel HE, Sittel C, Zorowka P, Jerke A. Dimensions of the laryngeal framework in adults. Surg Radiol Anat 1994;16(1):31-36.
- 4. Nadig SK, Uppal S, Back GW, Coatesworth AP, Grace AR. Foreign body sensation in the throat due to displacement of the superior cornu of the thyroid cartilage: two cases and a literature review. J Laryngol Otol 2006 Jul;120(7):608-609.
- 5. Lin D, Fischbein N, Eisele DW. Odynophagia secondary to variant thyroid cartilage anatomy. Dysphagia 2005;20(3):232-234.
- 6. Mortensen M, Ivey CM, Iida M, Woo P. Superior thyroid cornu syndrome: an unusual cause of cervical dysphagia. Ann Otol Rhinol Laryngol 2009 Dec;118(12):833-838.
- 7. Karaman E, Saritzali G, Albayram S, Kara B. An unusual cause of foreign-body sensation in the throat: a displaced superior cornu of the thyroid cartilage. Ear Nose Throat J 2011 Jun;90(6):E22-E24.
- 8. Smith ME, Berke GS, Gray SD, Dove H, Harnsberger R. Clicking in the throat: cinematic fiction or surgical fact? Arch Otolaryngol Head Neck Surg 2001 Sep;127(9):1129-1131.
- 9. Browning ST, Whittet HB, Williams A. Failure of insertion of a laryngeal mask airway caused by a variation in the anatomy of the thyroid cartilage. Anaesthesia 1999 Sep;54(9):884-886.
- 10. Dewan K, Yang C, Penta M. Anterior cervical pain syndrome: risk factor, variations in hyolaryngeal anatomy, and treatments. Laryngoscope 2020 Mar;130(3):702-705.