
A Palatal Mass
Rashid Al-Abri,1 Sudesh Kumar,1 Salim Al-Sudairi2
Al-Abri R, et al. OMJ. 25, 55-56 (2010); doi:10.5001/omj.2010.16
From the 1Department of ENT, Sultan Qaboos University Hospital, Sultanate of Oman 2Department of Oral Health,
Sultan Qaboos University Hospital, Sultanate of Oman.
Received: 18 Sep 2009
Accepted: 02 Nov 2009
Address correspondence and reprint request to: Dr. Rashid Al-Abri, Department of ENT,
Sultan Qaboos University Hospital, Sultanate of Oman
E-mail: ralabri@hotmail.com
INTRODUCTION
A 19 year old female patient presented to the ENT department with complaints of slow growing, painless palatal mass for three months duration. On examination, there was a smooth surface 3x3 cm mass arising from the left side of hard palate (Fig. 1) which was firm in consistency on palpation. The rest of ENT examinations were normal.

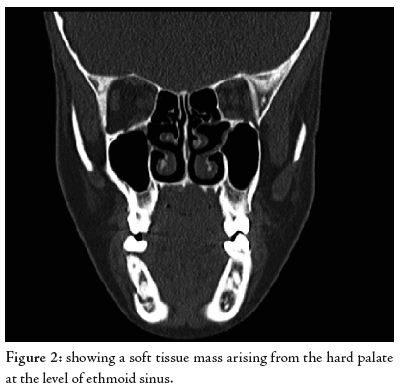
The Computed tomography (CT) showed a well defined contrast enhancing mass with no obvious bony erosion, (Fig. 2). The fine needle aspiration cytology from the lesion showed the histological features of epithelial and myoepithelial elements arranged in a variety of patterns and embedded in a mucopolysaccharide stroma.
ANSWERS
1. Pleomorphic adenoma of minor salivary gland arising from hard palate. The other rare differential diagnosis includes malignant minor salivary gland tumor, neurogenic tumors.
2. Preoperatively, the FNAC has a diagnostic role in such lesions. The mass lesion arising from the hard palate can be a malignant lesion requiring a radical approach.
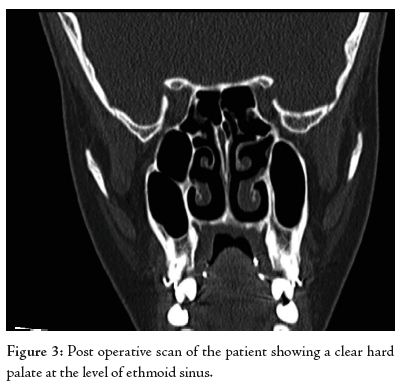
3. Complete surgical excision under general anesthesia is the treatment of choice for such a lesion (Fig. 3). The preoperative CT scan not only helps in delineating the extent of lesion but also is useful in assessing any bony erosion of hard palate.
DISCUSSION
The palate has the highest concentration of minor salivary glands in the upper aero-digestive tract.1 The pleomorphic adenoma is the most common benign minor salivary gland tumor arising from the palate.2 The clinical presentation of such a lesion is typically a firm or rubbery submucosal mass without ulceration or surrounding inflammation. The exact etiology of this tumor is unknown but it is hypothesized that it originates from the intercalated and myoepithelial cell.2
Preoperatively, the fine needle aspiration cytology has a definite diagnostic role and shows epithelial, myoepithelial, and stromal components. The CT scan and magnetic resonance imaging (MRI) showed, always performed to asses for the presence of any bony erosion, soft tissue or nerve involvement. Since the majority of minor salivary gland neoplasms arising from palate are malignant, a detailed history, examination and investigations are essential before the excision of such lesions.3 The complete surgical excision is the treatment of choice in cases such as pleomorphic adenoma. The lesion in the current case was excised completely under general anesthesia and patient was symptoms free in the six months follow up.
ACKNOWLEDGEMENTS
The authors reported no conflict of interest and no funding has been received on this work.
-
Beckhardt RN, Weber RS, Zane R, Garden AS, Wolf P, Carillo R, et al. Minor salivary gland tumors of the palate: clinical and pathological correlates of outcome. Laryngoscope 1995 Nov; 105(11):1155-1160.
-
Cummings CW, Frederickson JM, Harker LA, Krause CJ, Schuller DE. Otolaryngology head and neck surgery ,3rd ed. St.Louis: Mosby- Year Book,Inc; 1998.
-
Spiro RH. Salivary neoplasms: overview of a 35 –year experience with 2807 patients. Head Neck Surg 1986 Jan-Feb; 8(3):177-184.