
Recurrent Cervical Stenosis – a Troublesome Clinical Entity
Mariam Mathew, Anita Krishna Mohan
ABSTRACT
Cervical is a troublesome clinical problem. It usually follows surgery on cervix; also seen with endometrial and cervical malignancies. There is a high recurrence rate after the traditional treatment which is cervical dilatation. Various other treatment options have been tired. We report a case of recurrent cervical stenosis successfully treated with a different technique.
Submitted: 05Mar 2008
Reviewed: 15 Apr 2008
Accepted: 10 May 2008
From the Department of Obstetrics & Gynecology, Sultan Qaboos University Hospital, Al Khod, Muscat, Oman.Address correspondence and reprint requests to: Dr Mariam Mathew, Department of Obstetrics & Gynecology, Sultan Qaboos University Hospital, P O Box 38, Postal Code 123, Al Khoud, Muscat, Sultanate of Oman.
E-mail: mathewz@omantel.net.om
INTRODUCTION
Cervical stenosis is a troublesome clinical problem that usually follows cervical trauma. It is most commonly seen after cone biopsy for cervical intraepithelial neoplasia. Cervical stenosis is also seen with endometrial or cervical malignancies and with intrauterine adhesions. Intrauterine adhesions resulting in menstrual aberrations, infertility or recurrent abortions usually result from curettage in a pregnant or postpartum uterus. The traditional treatment of cervical stenosis is cervical dilatation, but it is associated with high recurrence rate.1 If dilatation is unsuccessful further therapy often remains unclear.
We report the successful treatment of recurrent cervical stenosis in a multiparous woman following evacuation for a partial mole.
CASE REPORT
A 42 year old Para 4+5 developed severe abdominal pain 3 months after evacuation and curettage for a partial molar pregnancy. She had remained amenorrheic since then. Serum ß human chorionic gonadotrophin (HCG) had returned to normal. On ultrasound examination, an intrauterine collection of 39x28mm was seen. (Figure 1) Pap smear showed no malignant cells. Patient underwent dilatation and drainage of haematometra under general anaesthesia. Hysteroscopy after release of haematometra did not show any abnormality. Histopathology of endometrium showed proliferative pattern. She returned after 4 weeks with similar symptoms and recurrence of haematometra was diagnosed on ultrasound scan. Patient underwent repeat dilatation of cervix, hysteroscopy and CuT 380 insertion under general anaesthesia. Following that she was put on Conjugated Estrogen with Medroxyprogesterone Acetate tablets for a month. During this period she had weekly outpatient dilatation of cervix three times. Patient became free of symptoms with return of normal menstruation for the past six months. The intrauterine devise was removed after three months.
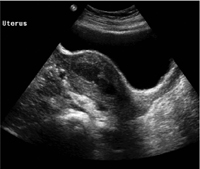
Figure 1: The arrow shows haematometra on transabdominal ultrasound scan.
DISCUSSION
Cervical stenosis is most commonly seen after Loop Electrosurgical Excision Procedures (LEEP) or cone biopsy for cervical intraepithelial neoplasia. Patients usually present with new onset dysmenorrhoea and amenorrhoea.2 If there is a visible dimple in the cervix and the patient is cooperative, an outpatient cervical dilatation can be attempted. If this is unsuccessful or not preferred, dilatation under general or regional anaesthesia with ultrasound assistance in the operating room is the next step. When a haematometra is present, entry into the uterus will be signaled by a gush of thick, brown old blood. Hysteroscopy with endometrial and endocervical sampling should be done to rule out malignancy.
Unfortunately cervical dilatation to relieve stenosis is often only a temporary success. The cervix which became stenotic before often becomes stenotic again with recurrence of haematometra. Clinical consequences of unsuccessful therapy can be severe, including hysterectomy.1
Alternative treatment options like transcervical insertion of a 16-22 fr. Malecot catheter,3 coated nitinol stent,4 and absorbable adhesion barrier – (Interceed; Gynecare, Ethicon, Somerville, NJ) 5 are reported in the literature. The catheter and temporary cervical stent may get dislocated and may be associated with uterine infection due to prolonged dilated cervix. Using an absorbable adhesion barrier in the cervical canal eliminates some of these potential complications.
The coated nitinol stent proposed by Grund et al 4 appears to be a valid alternative as it is elastic, flexible and self expanding with a continuous dilative force on the cervical canal. The permanent dilative force – optimally exerted in an elastic manner over 8 to 9 months – is claimed to have a long term effect. As the stent was not available in the country we had to look for other alternatives.
Use of intrauterine contraceptive device (IUCD) with oral cyclical hormones is an accepted treatment for intrauterine adhesions; but has not been reported for treatment of cervical stenosis. It is cheaper, easily available with no major complications. Hence it can be considered as a successful treatment option for this troublesome clinical entity.
CONCLUSION
In conclusion, insertion of copper IUCD with oral hormones and repeated outpatient dilatation as in our case can be considered as a successful treatment option for recurrent cervical stenosis.
-
Valle RF, Sankpal R, Marlow JL, Cohen L. Cervical stenosis: A challenging clinical entity. J Gynecol Surg 2002; 18:129-143.
-
Baldauf JJ, Dreyfus M, Wertz JP, Cuenin C, Ritter J, Philippe E. Consequences and treatment of cervical stenosis after laser conization or loop electrosurgical excision. J Gynecol Obstet Biol Reprod 1997; 26:64-70.
-
Yanushpolsky EH, Ginsburg ES, Fox JH, Stewart EA. Transcervical placement of a Malecot catheter after hysteroscopic evaluation provides for easier entry into the endometrial cavity for women with histories of difficult intrauterine inseminations and/or embryo transfers: a prospective case series. Fertil Steril 2000; 73:402-405.
-
Grund D, Kohler C, Krauel H, Schneider A. A new approach to preserve fertility by using a coated nitinol stent in a patient with recurrent cervical stenosis. Fertil Steril 2007; 87:1213-1216.
-
Gudipudi D, Montemarano N, Del Priore G. Alternative approaches to cervical stenosis. Fertil Steril 2007; 88:763-764.