|
Introduction
A 17-month-old female baby was presented as an urgent referral to Sultan Qaboos University Hospital, with a history of right face swelling associated with bulging of her right eye and intermittent fever of 10 days duration. There was no history of rhinorrhea or epistaxis. On examination, the face was asymmetrical with swelling of the right side of her face and right eye proptosis. Examination of the oral cavity showed that she was missing all the deciduous teeth on the right side, despite the presence of the deciduous teeth on the left side. Ophthalmological examination showed intact optic nerve.
MRI showed a large enhancing soft tissue mass on the right pterygopalatine fossa, measuring 5 × 4.2 × 3.8 cm (Fig. 1). It extended inferiorly to the right infratemporal fossa, posteriorly to the petrous bone close to the right carotid canal, inferomedially to the right parapharyngeal space, medially to the right lateral nasal wall, anterosuperiorly to the right orbit through the inferior orbital fissure, superoanteriorly compressing the right optic canal and superoposteriorly to the sphenoid bone. The mass extended to the retrorbital area compressing inferior muscles causing proptosis, with no globe involvement or bone destruction, and the optic nerve displaced superiorly (Fig. 1). There were bilateral multiple cervical lymph nodes on MRI. Bone scan and MRI chest, abdomen, and brain showed no metastasis. There was a large soft tissue mass in the right pterygoid and infratemporal fossa shown in the T2 weighted MR image (A), extending into the right posterior nasal choana (white arrow in A), with central degenerative changes. The mass showed intense enhancement in fat saturated T1 weighted axial, coronal and sagittal images (B, C and D). Biopsy was taken by intranasal endoscopic approach from the right lateral nasal wall. The histopathology diagnosis came as high grade malignant tumor. Histopathology slide is given. (Fig. 2)
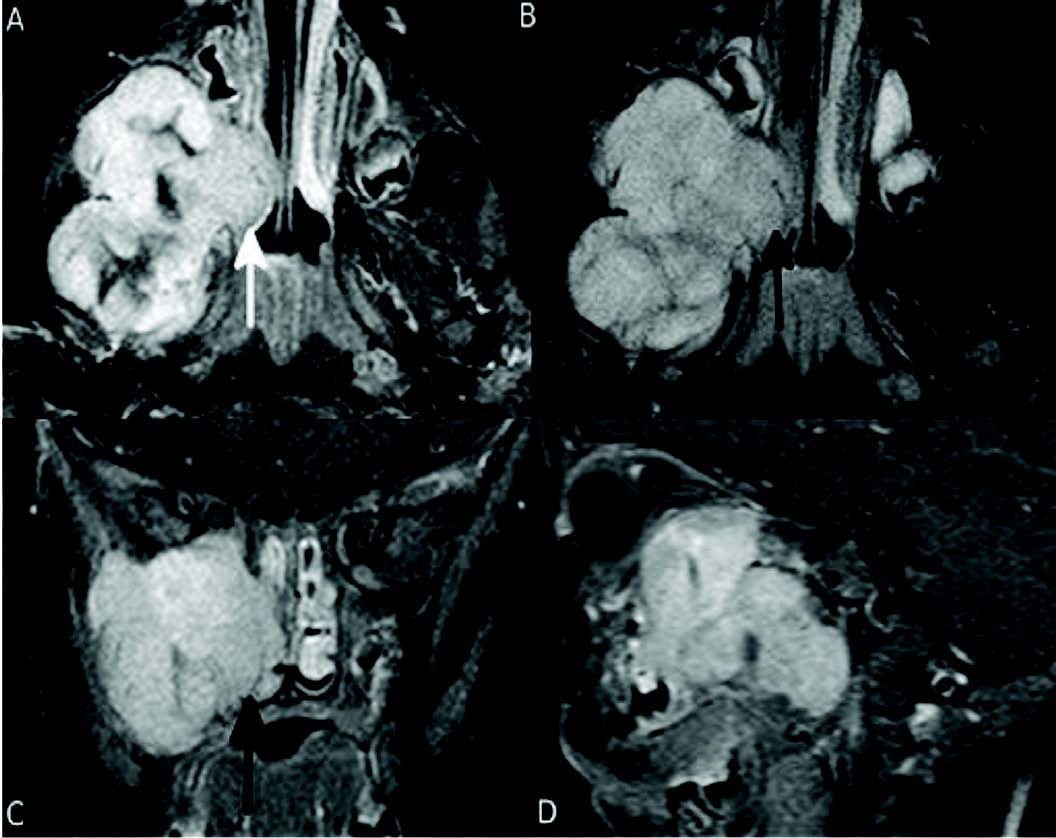
Figure 1: A) Soft tissue mass on right pterygoid and infratemporal fossa on T2-weighted images; B, C and D) T1 weighted axial, coronal and sagittal images.
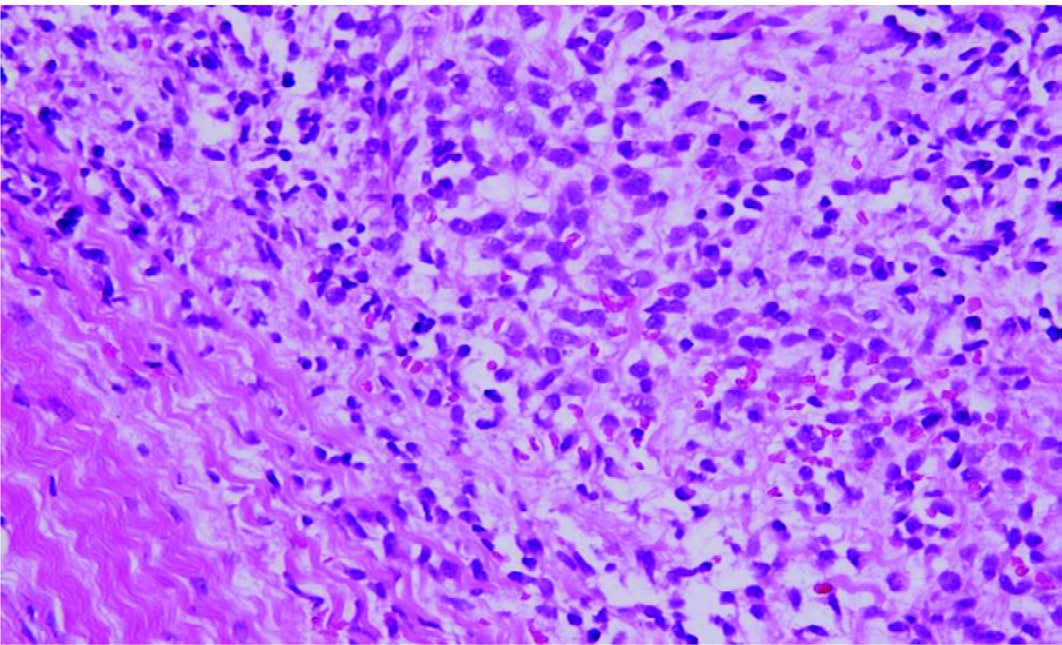
Figure 2: Histopathology slide.
Questions
1. What is the most likely diagnosis?
2. What is the role of MRI in the diagnosis?
3. What is the stage of the tumor?
4. What would be the treatment of choice in this case?
|