|
Abstract
Accidental ingestion of foreign bodies is common in ENT practice. A very small number of ingested foreign bodies perforate the esophagus and even a smaller fraction of extra mucosal migration penetrates into the soft tissues of the neck. Most cases reported in the literature involve fish bones. If left untreated, they may result in life threatening complications. This case presents a patient with a metallic foreign body (metal wire) in the esophagus which migrated extraluminally into the prevertebral muscle of the neck and describes the difficulties encountered in removing the migrated foreign body. Intra-operative radiography using two metallic pointers was used to locate the exact position of the foreign body during exploration of the neck.
Keywords: Esophagus; Metallic foreign body (steel wire); Migration; Prevertebral muscles.
Introduction
Accidental ingestion of foreign bodies being lodged in the upper aero-digestive tract is one of the most common otolaryngological emergency encountered at our tertiary care hospital. However, esophageal penetration and migration of foreign bodies into soft tissues of the neck are fairly rare occurances.1 Most reported cases in the literature involve fish bones which are eventually found in the soft tissue of the neck.2
Sharp penetrating foreign body in the esophagus may have varying presentations. They may penetrate the esophageal mucosa and may become embedded into the deeper sub mucosal and muscular layers of the esophagus. Sometimes the foreign bodies may penetrate through the esophageal wall and become lodged in the soft tissues of the neck.3-5 Rarely, have the penetrating foreign bodies been found to exit through the skin of the neck.6 The term "migrating" foreign body is used to describe these above cases.
Migrating foreign bodies into the soft tissue of the neck may remain quiescent or may cause life threatening suppurative or vascular complications,7 hence, removal of the migrated foreign body is imperative. Management involves exploration of the neck via an external approach. Locating the foreign body embedded into the soft tissues of the neck can sometimes be a challenging and frustrating experience for the surgeon. We present a case of migrating metallic foreign body embedded into the prevertebral muscles of the neck and share our experience with relevant review of literature.
Case Report
A 27-year-old female presented to the emergency department with history of pain while swallowing food for 3 days. She complained that the pain started immediately after having dinner. She was examined at the local hospital where a lateral radiograph of the neck showed a foreign body at the level of the 3rd and 4th cervical vertebrae. Flexible esophagoscopy was done at the local hospital. The foreign body could not be detected in the lumen of the esophagus during flexible esophagoscopy, so she was referred to our tertiary care hospital. On admission, she had severe odynophagia and dysphagia with fever of 38.5°C. She was started on intravenous antibiotics and intravenous fluids.
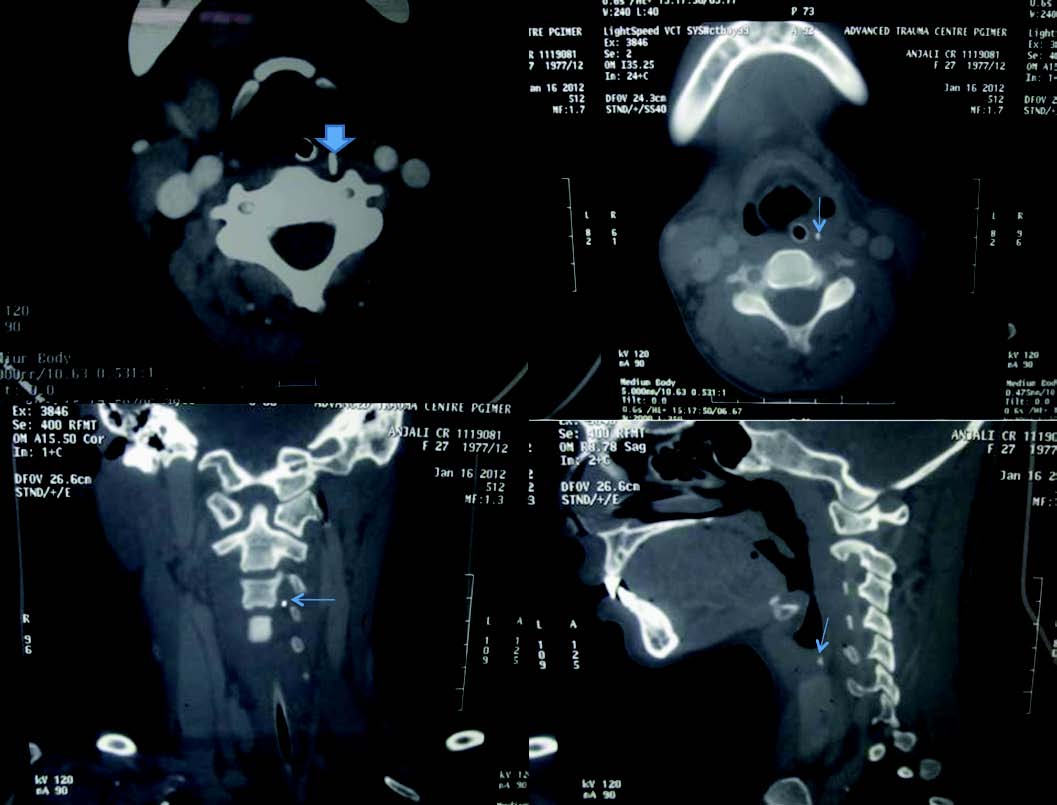
Figure 1: CT scan of the neck: (Axial and sagital) showing foreign body embedded into the prevertebral muscles.
Contrast-enhanced computer tomographic scan of the neck was done following suspicion of esophageal perforation. A radiopaque linear metallic foreign body was seen in the retropharyngeal space embedded into the prevertebral muscles at the level of the 3rd to 5th cervical vertebrae (Fig. 1). There was no surgical emphysema. Surgical exploration of the neck was performed through left lateral cervical incision. The sternocliedomastoid and carotid sheath were retracted laterally and the esophagus was retracted medially. A careful and extensive search was made in the retropharyngeal space but the foreign body could not be identified in the neck. With the aid of an intra-operative radiograph (fluoroscopy guidance), two metallic markers were placed and the foreign body was visualized between the two metallic markers (Fig. 2). An extensive search was made in the area between the markers. A 3 cm thin metallic wire was found embedded within the prevertebral muscle which was removed (Fig 3). Rigid esophagoscopy was done but no perforation of the esophageal lumen could be identified.
A nasogastric tube and vacuum surgical drain was placed and the wound closed in layers. Barium swallow done after 72 hrs showed no leak. The nasogastric tube was removed after 72 hrs. The patient had uneventful recovery and was discharged after one week.
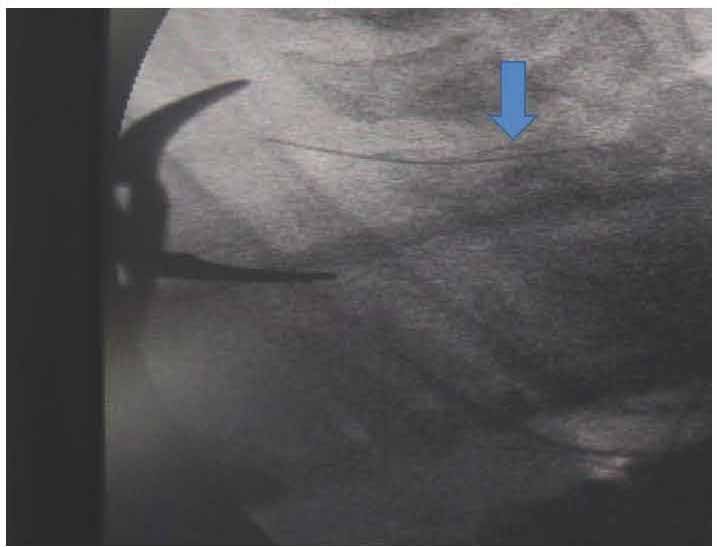
Figure 2: Intra operative radiography (using C arm) with metallic pointer showing the foreign body between two metallic markers.
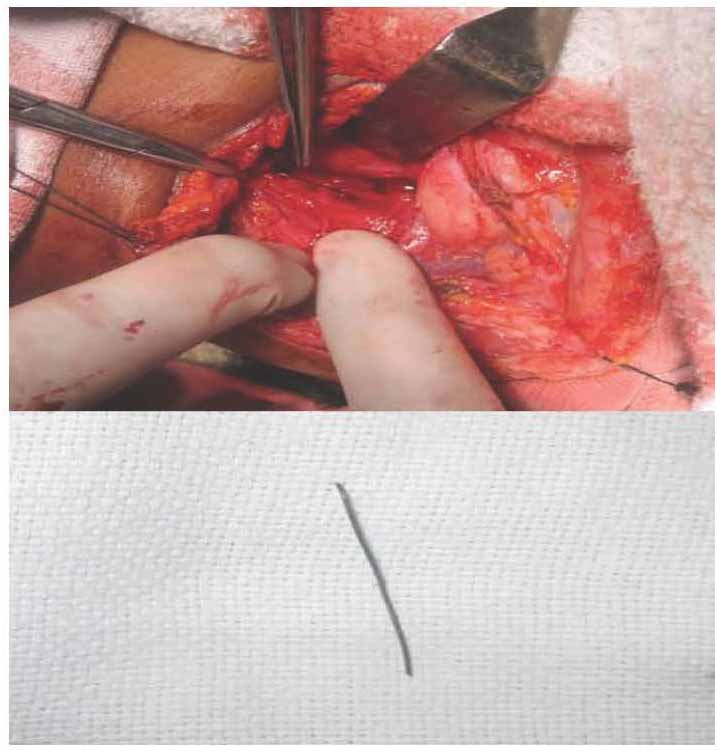
Figure 3: Foreign body embedded within prevertebral muscles removed by exploration of the neck.
Discussion
Foreign bodies of the upper aerodigestive tract are one of the most common emergencies in day-to-day otolaryngological practice. Commonly found objects in adults include fish bones, chicken bone, pieces of glass, dentures, coins, and needles. These foreign bodies can be lodged in the tonsils, valeculla, pyriform sinus and the cervical esophagus. They can easily be removed by esophagoscopy.
However, sharp-edged foreign body may rarely penetrate the esophageal lumen and migrate extraluminally into the soft tissues of the neck. Remsen et al. reported 321 cases of penetrating foreign bodies and only 43 of these cases were found to have migrated extra luminally into the neck.8 The sharper the foreign body, the greater the risk of perforation. Horizontally oriented foreign bodies are more likely to penetrate the esophageal lumen. The exact mechanism of perforation is still unknown. Possible mechanisms include: strong esophageal peristaltic movements against the foreign body, neck movement and careless manipulation of the foreign body while attempting to remove it may actually influence the risk of perforation. Tissue reaction to the foreign body as well as infection and abscess formation could also play a part.
A migrated foreign body may remain quiescent or may lead to life threatening complications which may include suppurative complications like retropharygeal and parapharyngel abscess,9 epidural abscess,10 thyroid abscess and mediastinitis.7 Vascular complications like carotid rupture, penetration of facial artery, arotoesophageal and innominate esophageal fistula have also been reported.8 Patients with penetrating foreign bodies present with foreign body sensation, odynophagia or hemoptysis and sometimes with fever and neck swelling. A foreign body should be suspected to have migrated extraluminally when esophagoscopy fails to identify the foreign body in the esophageal lumen and postoperative radiograph confirms its presence still in the neck. CT scan of the neck with fine 1 mm cuts is the investigation of choice to predict the exact location of the foreign body.1 In some situations, CT scan may not be able to predict whether the foreign body is within or outside the wall of the esophagus. In such situation, CT with contrast is helpful. If the foreign body is seen distinctly away from the contrast in the lumen, then the foreign body can be safely assumed to be extraluminal. Barium swallow is useful in detecting esophageal leak but its value is limited in localizing the foreign body.
Exploration and early removal of the migrated foreign body via an external approach is recommended to prevent life threatening complications. The position of the neck during CT scan and surgery may not be the same because soft tissues of the neck are mobile in relation to the bony and cartilaginous structures so it should be kept in mind that the position of the foreign body may not be the same during surgery as seen on CT scan,11 as was seen in this report. Because the neck was extended during surgery, the foreign body was found lower than what was seen on CT scan. Exploration of the neck to locate the foreign body can sometimes be a frustrating experience for the surgeon as was true in the current case. Use of intraoperative radiograph using fluoroscopy supplemented with metallic markers to locate the foreign body can be of great help to the surgeon as it was in this case report.12 Intra operative radiograph is useful especially in cases where the foreign body is embedded within the muscles. Nasogastric tube must be placed in all cases to allow for healing of the perforation while allowing feeding to continue. Barium swallow should be done to check for persistent esophageal perforation before removing the nasogastric tube.
Conclusion
A high index of suspicion is needed to diagnose a migrating foreign body. Early intervention is crucial in such cases to prevent complications. A thorough esophagoscopy and CT scan of the neck with and without oral contrast are the gold standard for diagnosis. A careful and systematic approach during exploration of the neck is needed. Intraoperative radiography can be of great help in locating the foreign body. Thus intraoperative CT scan may play a role in managing difficult situations in the future.
Acknowledgements
The authors reported no conflict of interests and no funding was received for this work.
References
1. Chung SM, Kim HS, Park EH. Migrating pharyngeal foreign bodies: a series of four cases of saw-toothed fish bones. Eur Arch Otorhinolaryngol 2008 Sep;265(9):1125-1129.
2. Leong HK, Chan RK. Foreign bodies in the upper digestive tract. Singapore Med J 1987 Apr;28(2):162-165.
3. al Muhanna A, Abu Chra KA, Dashti H, Behbehani A, al-Naqeeb N. Thyroid lobectomy for removal of a fish bone. J Laryngol Otol 1990 Jun;104(6):511-512.
4. Bakshi J, Verma RK, Karuppiah S. Migratory foreign body of neck in a battered baby: a case report. Int J Pediatr Otorhinolaryngol 2009 Dec;73(12):1814-1816.
5. Al-Sebeih K, Valvoda M, Sobeih A, Al-Sihan M. Perforating and migrating pharyngoesophageal foreign bodies: a series of 5 patients. Ear Nose Throat J 2006 Sep;85(9):600-603.
6. Sethi DS, Stanley RE. Migrating foreign bodies in the upper digestive tract. Ann Acad Med Singapore 1992 May;21(3):390-393.
7. Loh KS, Tan LK, Smith JD, Yeoh KH, Dong F. Complications of foreign bodies in the esophagus. Otolaryngol Head Neck Surg 2000 Nov;123(5):613-616.
8. Remsen K, Lawson W, Biller HF, Som ML. Unusual presentations of penetrating foreign bodies of the upper aerodigestive tract. Ann Otol Rhinol Laryngol Suppl 1983 Jul-Aug;105:32-44.
9. Poluri A, Singh B, Sperling N, Har-El G, Lucente FE. Retropharyngeal abscess secondary to penetrating foreign bodies. J Craniomaxillofac Surg 2000 Aug;28(4):243-246.
10. Tsai YS, Lui CC. Retropharyngeal and epidural abscess from a swallowed fish bone. Am J Emerg Med 1997 Jul;15(4):381-382.
11. Lu PK, Brett RH, Aw CY, Singh R. Migrating oesophageal foreign body–an unusual case. Singapore Med J 2000 Feb;41(2):77-79.
12. Sreetharan SS, Prepageran N, Satwant S. Unusual migratory foreign body in the neck. Singapore Med J 2004 Oct;45(10):487-488.
|