|
Introduction
Occupational noise-induced hearing loss or noise-induced hearing loss (NIHL) is a worldwide problem in the industry and it contributes to 16% of hearing loss among adults globally, ranging from 7% to 21% in various sub-regions and higher in developing countries.1 In Malaysia, cases of NIHL investigated by the Department of Occupational Safety and Health (DOSH) had increased from 120 cases in 2007 to 427 cases in 2009.2,3 Noise is one of the environmental and occupational hazards listed in the Factory and Machinery Act 1967.
NIHL is a temporary or permanent sensorineural hearing loss caused either by a single exposure to a very loud sound or by repeated exposure to louder sounds over an extended period.4 Normally, it affects both sides of the ears due to noise exposure above 85 dB.5 The WHO defines material hearing impairment as an average of the hearing threshold levels (HTL) for both ears that exceed 25 dB at 1000, 2000, 3000, and 4000 Hz.6 Furthermore, hearing loss or deafness would lead to abnormal behavior such as anxiety disorders, mood disorders, personality disorders and schizophrenia; as well as communication breakdown.7
Quarrying is one of the major activities in producing materials (i.e., rock and sands) for building infrastructures. The main activity of quarries in this state involves granite blasting, crushing granite into smaller rocks and converting it into asphalt.8 The main contributory noise comes from the granite crushers. Besides, sounds from engines of excavators, dumping trucks and lorries are also considered as sources of noise.9
There are limited data on knowledge, attitude and practice (KAP) among quarry workers. The study on KAP towards NIHL among sawmill workers revealed poor scores, especially in terms of knowledge and practice.10,11 Meanwhile, on the prevalence of NIHL, studies conducted in other industries have shown a high prevalence of NIHL varying from 16% to 83%.10,12-16 Some of the identified associated factors included age, being smoker, intensity of noise exposed, duration of working, poor practice in using HPD, and ignorance.10,17 Konings et al. reported that genetics also plays a role in determining the susceptibility to hearing loss.18 Other causes of sensorineural hearing loss include diseases to the inner ear such as Miniere’s disease or tumors,19 and hepatitis B infection.20
This study aims to assess the KAP towards NIHL, prevalence of NIHL and its associated factors among quarry workers as evidence to enhance the promotion of hearing conservation program in the industry.
Methods
This cross sectional study was conducted among quarry workers in a north-eastern state of Malaysia from October 2009 to July 2010. The list of quarries was obtained from the state’s Mineral and Geosciences Department, and the permission was obtained from the respective quarries’ managers. Six quarries consented to participate in the study. The total number of eligible respondents was 119, but only 97 completed all the questionnaires and tests required with an 82% response rate. The respondents who were male, aged between 18 to 50 years, working in the quarry area for at least 6-month duration with no family history of ear diseases were included in this study.
Participants were required to answer a set of validated questionnaires on KAP towards NIHL.11 The questionnaires were developed and validated in Malay language. The Cronbach's alpha of knowledge, attitude and practice domains were 0.7, 0.9 and 0.8, respectively. It consisted of socio-demographic data, occupational and non-occupational history, knowledge, attitudes and practice domains. The knowledge domain had seven sub-domains of 16 items with multiple choice answers (true, false or do not know). The correct answer was given a score of 2, ‘do not know’ was given a score of 1 and wrong answer was given a score of 0, with a total score of 32. The attitude domain also had seven sub-domains of 22 items, with answer options ranging from strongly disagree, disagree, neutral, agree, to strongly agree. The score was in a Likert scale from 0 to 4 depending on the questions. For the respondents to be considered as having good attitude, they would answer with the two highest scores according to the Likert scale mentioned. Practice domain had only two subdomains with 11 items. The answer scores was based on the Likert Scale from 0 to 3; 0 for never, 1 for seldom, 2 for often and 3 for always; thus the total score for this part was 33. The percentage of the scores was calculated by dividing the score by the total score for every domain then multiplied by 100%. According to Razman et al.11 to gain satisfactory knowledge, the score should be more than 70% of the total score.
Finally, the respondents underwent pure tone audiometry (PTA) to determine their hearing status. All audiometric tests were conducted by a qualified audiologist at the Audiology Laboratory, ORL-HNS Clinic, using a two-channel clinical audiometer made by Grason-StadlerInc, USA model GSI 61®. With the ears covered by headphone and back-facing the audiologist, the respondent was asked to press the button whenever he heard a tone. The lowest tone heard at each frequency was considered as the hearing threshold (HTL).21 The hearing thresholds of each ear at frequencies of 500, 1000, 2000, 4000 and 8000 Hz with increments of 10 dB, were then measured. The noise level of the machines used was measured using the Impulse Integrating SLM made by Quest® model 2800. A total of 39 crushers, 12 truck cabins, 12 excavator cabins, and 12 shovel cabins were measured.
Data analysis for descriptive and logistic regressions to determine the associating factors was performed using PASW Statistics 18 Version 18.0 This study obtained ethical approval from the Ethical Committee, School of Medical Sciences, University Sains Malaysia on 12 Nov 2007.
Results
A total of 97 respondents participated and completed the entire test required in this study. The socio-demographic and occupational characteristics of the respondents are shown in Table 1. The self-reported non-occupational noise exposure characteristics of the respondents are shown in Table 2.
Table 1: The sociodemographic and occupational characteristics of the 97 respondents.
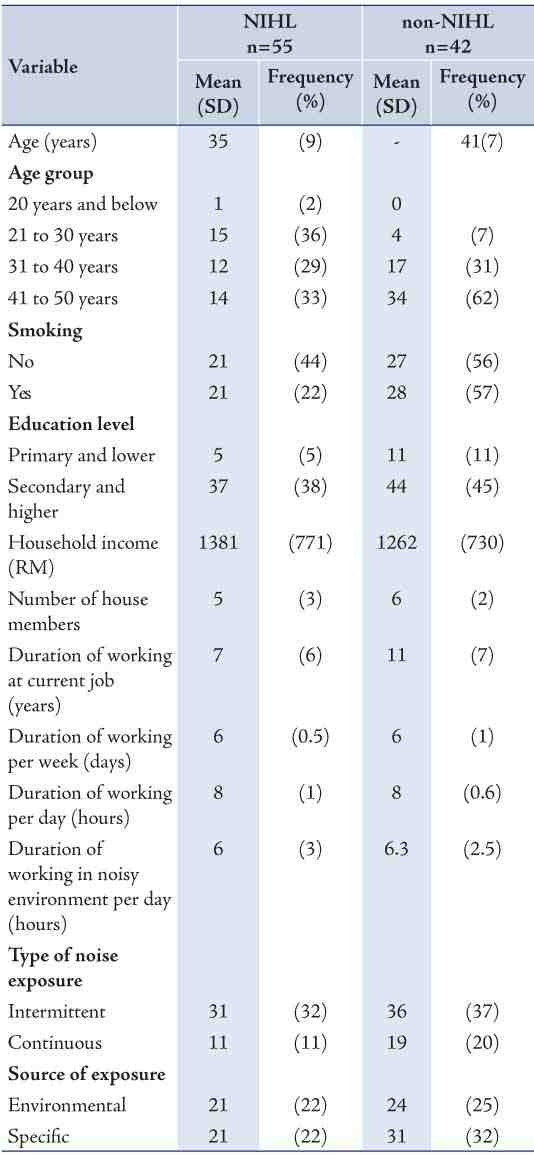
Table 2: Self-reported non-occupational noise exposure of the 97 respondents.
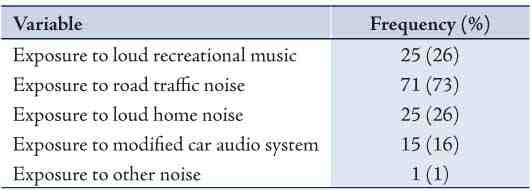
Table 3: Mean score and mean percentage score of KAP of the 97 respondents.
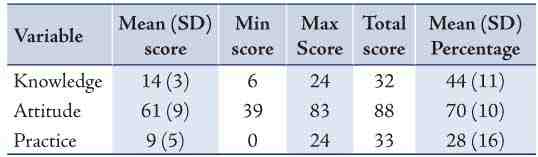
Table 4: Correct answers by the 97 respondents in the knowledge domain.
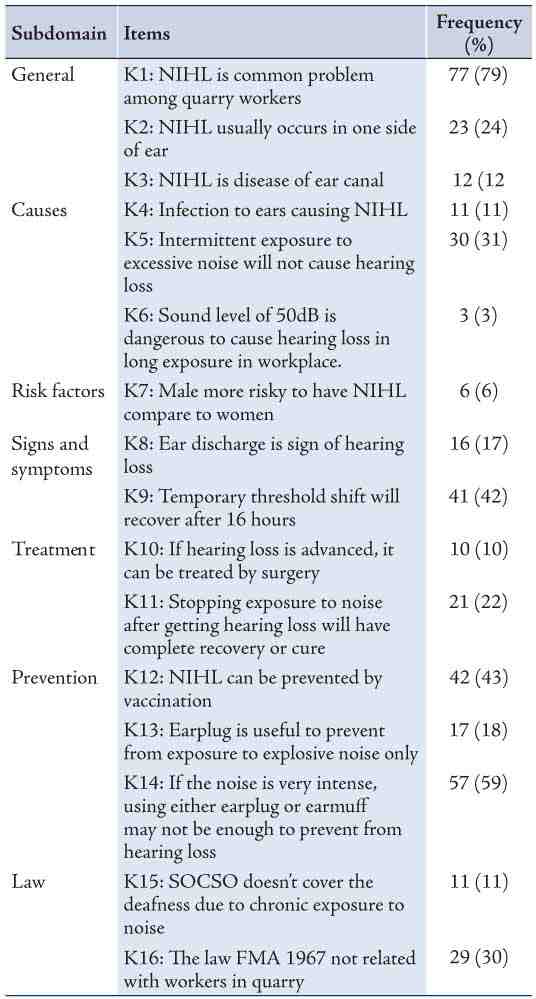
Table 5: Good attitude shown by the 97 respondents.
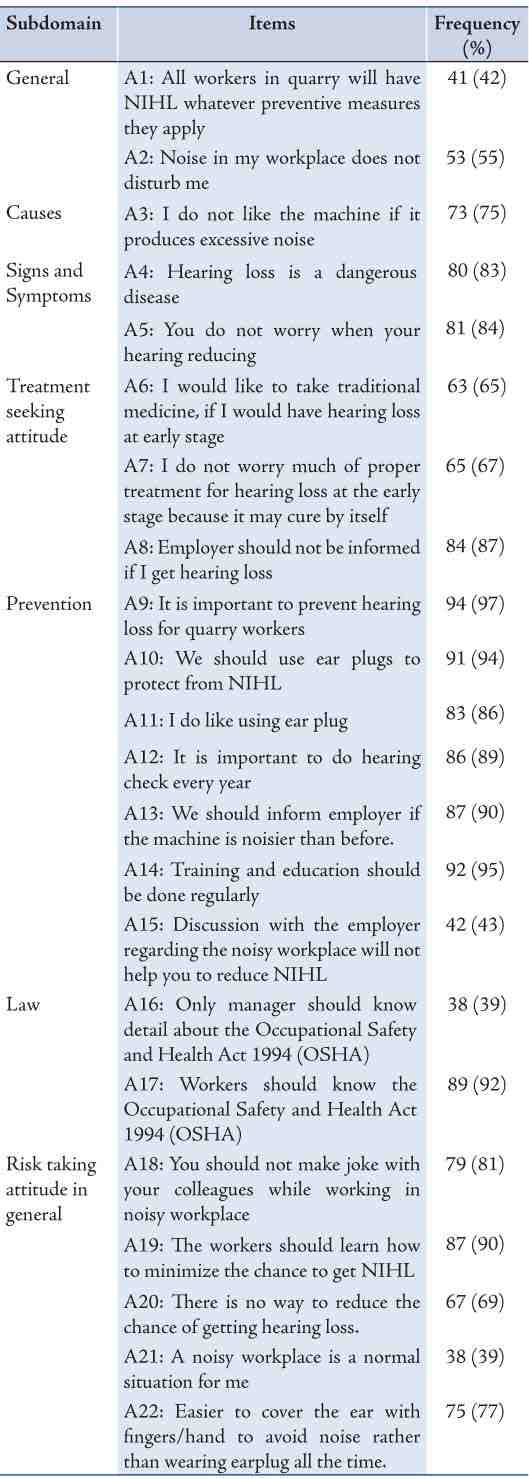
Table 6: Good practice shown by the 97 respondents.
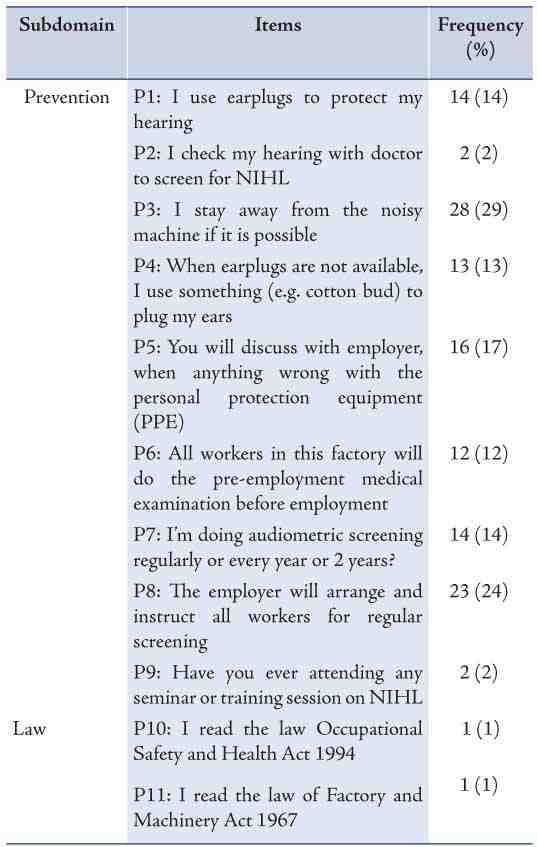
The mean score and percentage of KAP are shown in Table 3. The most correct answer obtained in the knowledge domain was only K1 (79%). For the attitude domain, respondents scored well in most of the items; however, they scored low on attitude towards risk-taking behavior and prevention. The poor score for risk-taking behavior and prevention were reflected by the poor score in the practice domain. The frequency and percentage of correct answers given by respondents in the knowledge domain are shown in Table 4, while the frequency and percentage of answers representing good attitude are shown in Table 5, and the frequency and percentage of answers representing good practice are shown in Table 6.
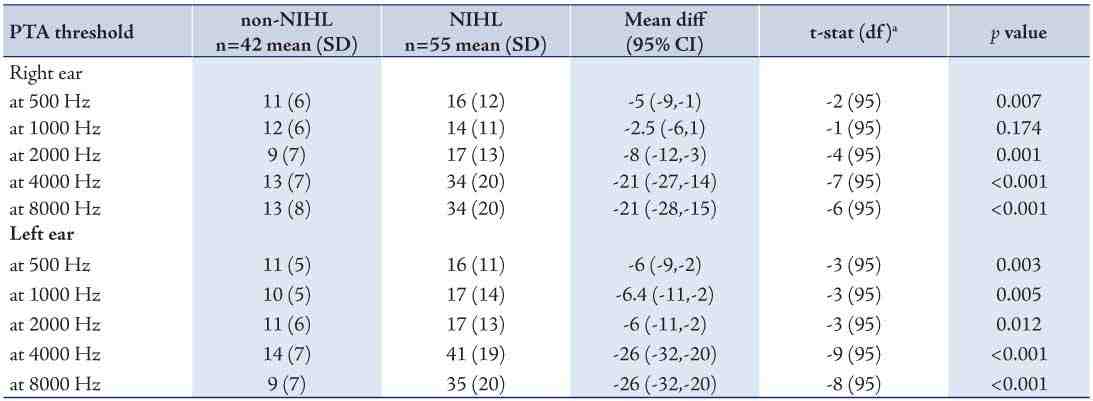
From the PTA test performed, the prevalence of hearing loss was 57% (95% CI 47, 67). Of these, only 9 (16%) had severe hearing loss and the remaining had mild or moderate hearing loss. PTA test performed on the 97 respondents revealed significant differences in mean hearing threshold levels (HTL) between the non-NIHL and NIHL at all tested frequencies for both ears with p-values ranging from <0.001 to 0.05, except at 1000 Hz for the right ear which showed no significant difference in mean threshold level between participants with NIHL and non-NIHL (p=0.174), as shown in Table 7. The results from comparison of means of HTL are shown in Table 8. Overall, among the 97 respondents, 34 (62%) had bilateral hearing loss and 21 (38%) had unilateral hearing loss.
From the univariate analysis, the associated factors of NIHL were age (crude OR 1.1, 95% CI: 1.1, 1.2; p<0.001), duration of work at current job (crude OR 1.1, 95% CI: 1.0, 1.2; p=0.008), number of working days per week (crude OR 2.2, 95% CI: 1.0, 4.7; p=0.048), and practice score (crude OR 0.9, 95% CI: 0.8, 1.0; p=0.014). The multivariate analysis performed revealed age and practice score to be the associated factors with adjusted OR 1.1 (95% CI: 1.1, 1.2) and 0.9 (95% CI: 0.8, 1.0), respectively.
Table 7: Mean hearing threshold level (HTL).
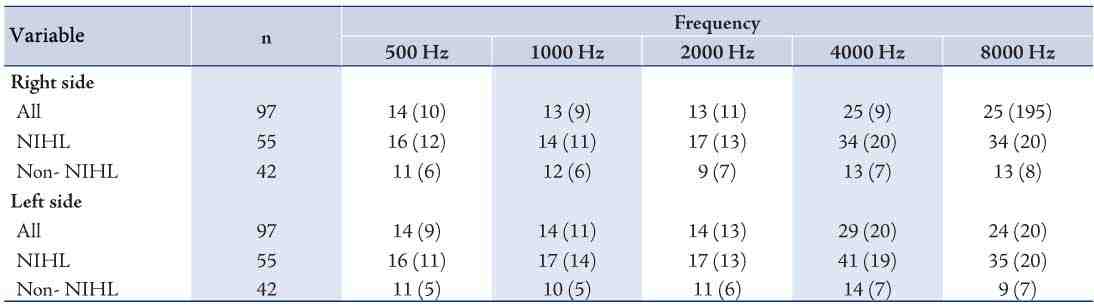
Table 8: Comparison of mean HTL between non-NIHL and NIHL.
Discussion
In the quarries, noise was mainly generated from the machines used. The noisiest machines were the crusher and shovel with mean sound levels of 98 (7) and 91 (7) dB (A), respectively. These sound levels exceeded the level that may cause NIHL to the workers.5 The mean (SD) age for the respondents was 38 (8) years. The mean age was relatively young since the respondents were selected among those aged between 18 to 50 years in order to avoid the probability of presbycusis among respondents.22
The mean age of participants with NIHL was higher compared to their counterparts without NIHL (41 [7] and 35 [9] years, respectively), (Table 1). This finding was also comparable with the study among metallurgical company workers in Rio de Janeiro, Brazil which showed age in those with NIHL to be older (50 [12] years) compared to those without NIHL (34 [11] years).13
The mean percentage of total scores obtained in this study for knowledge, attitude and practice towards NIHL were 44 (11), 70 (10) and 28 (16), respectively. These figures are comparable with the scores reported in previous studies on sawmill workers by Fadzli,10 where the mean percentage of total scores were 45 (13), 67 (9) and 10 (7), and by Razman et al.11 where the mean percentage of total scores were 69 (9), 61 (9) and 19 (14) for knowledge, attitude and practice, respectively.
In this study, there was only one respondent with the satisfactory score level in knowledge, 46 (47%) in attitude and one in practice. These findings were similar to those reported by Fadzli,10 which showed areas the percentage of those with satisfactory level was 0% in knowledge and practice, but in attitude domain this study showed better percentage of respondents with a satisfactory level (19%). The poor scores in KAP and similarly with studies conducted by Fadzli,10 and Razman et al.11 were mainly due to low socioeconomic group and lack of awareness among the workers. The educational level of the respondents was below secondary level, and they displayed ignorance on the use of personal protective equipment (PPE). In the current study, the percentage of those using proper PPE (i.e., ear muffs) was only 49%.
The prevalence of NIHL among the quarry workers in this study was 57% (95% CI: 47, 67). The prevalence was high compared to those reported in a metallurgical company in Rio de Janeiro, Brazil (16%),13 and electro production workers in Greece (44%),16 but comparable to the NIHL prevalence among hydroelectric power plants in Turkey (56%).12 However, it was lower than those reported among industry workers in Malaysia (83%),14 and sawmill workers in Kota Bharu, Kelantan (80%).10
The degree of hearing loss also ranged from mild to severe based on the WHO classification.6 In this study, from 55 of the respondents with NIHL, 23 (42%) had mild and moderate hearing loss and 9 respondents (16%) had severe hearing loss, suggesting that the majority were at the early stages of developing NIHL.
Of the 55 of the respondents with NIHL, 34 (62%) had bilateral hearing loss, 14 (26%) had hearing loss on the left side only, and 7 (13%) only had hearing loss on the right side. Although the standard definition of NIHL is hearing loss on both sides, unilateral NIHL was also common. A study conducted among student musicians in North Carolina showed the prevalence of unilateral NIHL to be 34%.15 While a study by Fadzli also found 14% of sawmill workers to be exhibiting unilateral hearing loss which was worse on the left ear.10 In addition, Ali et al. reported 67% of workers at a cement company in Nigeria had mild sensorineural hearing loss in the right ear while 12% had moderate sensorineural hearing loss in the right ear.23 The cause of unilateral noise-induced hearing loss is not well understood, but on interviews with the respondents, they mentioned using one ear to listen to the machine, especially when they heard some abnormalities in the sound of the machine. They also placed their ear facing one side of the source of noise while performing their daily tasks.
The current study revealed the associated factors contributing to NIHL to be age and practice score. Age was found to be an associated factor with adjusted OR 1.1 (95% CI 1.1, 1.2; p<0.001) and practice score with adjusted OR 0.9 (95% CI 0.8, 1.0; p=0.008). A previous study by Rachiotis et al.16 found those aged over 40 years had 5.3 odds of developing NIHL compared to their younger counterparts. While Guerra et al.13 grouped their subjects into four age groups with up to 20 years-old as the reference and they found subjects aged between 30 and 39 years had 1.3 odds, those aged between 40 and 49 years had 6.0 odds, and those aged over 50 years had 21.3 odds of developing NIHL. In the study on sawmill workers; Fadzli was able to show the associated factors were age, smoking status and duration of work. He found that when the age of workers increased by one year, their hearing threshold would increase by 1 dB(A).10 The association between NIHL and KAP score has only been studied by Fadzli, who found no significant association between knowledge, attitude and practice score and NIHL with p-values of 0.473, 0.075 and 0.084, respectively.10
In identifying the limitation in this study, one major component would be the fact that all the selected respondents were males; but this is so because all the workers in the quarry area and those exposed to the noise were males.24 Indeed there were female personnel working in the quarry areas; however, they were confined in offices occupying clerical jobs such as administration and accounting, and were thus not subjected to noise monitoring regulations.25 Also, most of the information in the questionnaires was obtained by self-reporting and therefore may be subjected to recall bias.
Conclusion
We conclude that noise is one of the occupational hazards and environmental pollutants in quarries causing NIHL among workers. This may be caused by working with noisy machines or being exposed to other environmental noise. The poor KAP score towards NIHL among quarry workers were below satisfactory level especially in the domain of practice. This may lead to higher prevalence of NIHL in the future.
Acknowledgements
The authors reported no conflict of interest and no funding was received for this work.
References
1. Nelson DI, Nelson RY, Concha-Barrientos M, Fingerhut M. The global burden of occupational noise-induced hearing loss. Am J Ind Med 2005 Dec;48(6):446-458.
2. DOSH, Annual Report Department of Occupational Safety and Health Malaysia. 2007.
3. DOSH, Annual Report Department of Occupational Safety and Health Malaysia. 2009.
4. Mosby, Mosby's Medical Dictionary 8th ed. 2009, St Louis: Elsevier.
5. ACOEM. Noise-induced Hearing Loss. 2002 [cited 2010 26 Nov 2010]; Available from: http://www.acoem.org/guidelines.aspx?id=846.
6. WHO, Report of the Informal Working Group On Prevention Of Deafness And Hearing Impairment Programme Planning. 1991: Geneva.
7. Scheetz NA. Psychosocial Aspects of Deafness. 2004, Boston: Pearson Allyn and Bacon.
8. MGD. Quarry Resource Planning for the State of Kelantan. 2003: Mineral and Geoscience Department Malaysia.
9. DOSH. Noise Monitoring Report. 2010, Department of Occupational Safety and Health: Kelantan.
10. Fadzli MN. Knowledge, Attitude and Practice, and Effect of Occupational Noise Exposure on Hearing Among Sawmill Workers in Kota Bharu, Kelantan in Department of Community Medicine. 2005, USM.
11. Rus RM, Daud A, Musa KI, Naing L. Knowledge, attitude and practice of sawmill workers towards noise-induced hearing loss in kota bharu, kelantan. Malays J Med Sci 2008 Oct Oct;15(4):28-34.
12. Çelik O, Yalçin S, Oztürk A. Hearing parameters in noise exposed industrial workers. Auris Nasus Larynx 1998 Dec;25(4):369-375.
13. Guerra MR, Lourenço PM, Bustamante-Teixeira MT, Alves MJ; Prevalence of Noise-Induced Hearing Loss in Metallurgical Company. [Prevalence of noise-induced hearing loss in metallurgical company]. Rev Saude Publica 2005 Apr;39(2):238-244.
14. Maisarah, S. and H. Said, The Noise Exposed Factory Workers: The Prevalence of Sensori-Neural Hearing Loss and Their Use of Personal Hearing Protection Devices Med J Malaysia 1993 48(3): 280-285.
15. Phillips, S.L., V.C. Henrich, and S.T. Mace, Prevalence of Noise-Induced Hearing Loss in Student Musicians International Journal of Audiology, 2010 49: 309-316.
16. Rachiotis, G., C. Alexopoulos, and S. Drivas, Occupational Exposure to Noise, and Hearing Function among Electro Production Workers Auris Nasus Larynx International Journal of ORL and HNS, 2006. 33: 381-385.
17. Ferrite S, Santana V. Joint effects of smoking, noise exposure and age on hearing loss. Occup Med (Lond) 2005 Jan;55(1):48-53.
18. Konings A, Van Laer L, Van Camp G. Genetic studies on noise-induced hearing loss: a review. Ear Hear 2009 Apr;30(2):151-159.
19. Emnuel DC, Letowski T. Hearing Science, 2009, Philadelphia, Lippincot Williams and Wilkins.
20. Nasab MS, Fathololoomi MR, Alizamir A, Fathololoomi MR, Alizamir A; Fathololoomi M.R; Alizamir A. Association between hepatitis B and hearing status. Oman Med J 2012 Sep;27(5):418-420.
21. DeBonis D, Donohue C. Survey of Audiology: Fundementals for Audiologists and Health Professionals. 2nd ed. 2008, Boston: Pearson Allyn and Bacon.
22. Huang T. Age-related hearing loss. Minn Med 2007 Oct;90(10):48-50.
23. Ali A, Garandawa HI, Nwawolo CC, Somefun OO; Noise-Induced Hearing Loss at Cement Company, Nigeria. Online Journal of Medicine and Medical Science Research 2012;1(3):49-54.
24. MGD. List of Employees in Quarries in Kelantan. 2009, Mineral and Geosciences Department: Kelantan.
25. Malaysian Government, Factories and Machinery Act 1967 (Act 139) and Regulations. 1967, Kuala Lumpur: International Law Book Services.
|