| |
Abstract
Objective: Cleft lip with or without cleft palate is the most common orofacial congenital anomaly among live births. This study was carried out to determine the incidence rate of oral clefting in Gorgan, North of Iran during 2004-2009.
Methods: This descriptive hospital-based study was performed on 35,009 live newborns in Dezyani Hospital in Gorgan, Northern Iran during 2004-2009. All newborns were screened for oral clefts. Data including birth date, gender, type of oral clefts, parents' consanguinity, parental ethnicity and presence of other congenital anomalies were recorded for analysis.
Result: The overall incidence rate of oral clefts during this 6-year period was 1.05 per 1000, or 1 per 946 live births. The incidence of cleft lip and isolated cleft palate was 0.08 and 0.37 per 1,000 live births, respectively. The ratio for different cleft types was 1:7:4 (CL: CLP: CP).
The incidence of oral clefting was 1.2 per 1,000 male births and 0.86 per 1,000 female births (RR=1.40, 95%, CI: 0.73-2.71). According to parental ethnicity, the incidence of oral clefting was 0.7, 1.7 and 1.26 per 1,000 in Native Fars, Turkman and Sistani, respectively. The relative risk for oral clefting in Turkman to native Fars group was 2.56 (p<0.02). In this study, 56.7% of clefts were CL+P, 8.1% were CL and 35.1% of cases were CP. CP was more common for girls (54%) than for boys (46%) but CL was more common for boys.
Conclusion: The result showed that the incidence of oral clefts in the study population as being at 1.05 per 1,000 live births, which is increased compared to an earlier study in this area with 0.97 per 1,000 live births.
Keywords: Cleft lip; Cleft palate; Gender; Ethnicity; Iran.
Introduction
Cleft lip with or without cleft palate is the most common orofacial congenital anomaly among live births.1 The oral clefting rates varies from 1:500 to 1:2000 births in different countries.2 The incidence rate of oral clefts in various parts of Iran varies from 0.80 to 2.14 per 1,000 births. Oral clefting incidence in northern Iran was reported to be at 0.97 per 1,000 (1 in 1025) births during 1998-2003.3 The International Prenatal Database of Typical Orofacial Clefts has recently reported that the overall incidence of cleft lip with or without cleft palate was 0.99 per 1,000. The incidence of cleft lip was 0.328 per 1,000 and that of cleft lip and palate was 0.664 per 1,000.4
Oral clefting is affected by gender, geographic location, nationality, nutritional and periconceptional consumption of folic acid.5-7 In addition, several studies have reported that positive family history is associated with oral clefts.1,8,9 Indeed, maternal age, maternal alcohol consumption, psychological stress during pregnancy, diabetes mellitus type 1, anticonvulsant drugs, and maternal smoking have been shown to be risk factors for oral clefts.10-15 Racial and ethnic factors have also shown to have an effect on the incidence rate of oral clefts. A high rate of oral clefting is found in Asian and Native American populations and the lowest is reported among African populations.6 An intermediate rate of oral clefts is shown in Caucasians.5,16,17 The main objective of this study was to establish the incidence and explore effective variables on cleft lip and palate in Gorgan, Northern Iran during 2004-2009.
Methods
This hospital-based study identified all newborns with an oral cleft from among 35,009 live births between 2004 and 2009 in the Dezyani Hospital. This hospital is the largest hospital with labor facility in Gorgan, a capital city in the Golestan province in Northern Iran. It is a referral hospital with an annual rate of more than 6,000 deliveries, accounting for the largest portion of deliveries in the city. Patients are usually from moderate to low socioeconomic class families with various ethnic backgrounds.
Native Fars, Turkman and Sistani are the three main ethnic groups in the area. Native Fars are the predominant inhabitants and have the most members. Turkman is the ethnic group that emigrated from central Asia more than three centuries ago. The Sistani group emigrated from southeastern Iran since half a century ago. All live births delivered in this hospital during the investigation were examined and screened for oral clefts immediately after delivery by a gynecologist. The diagnosis was later confirmed by a pediatrician according to ICD-10. A questionnaire addressing relevant clinical and demographic factors was completed for each case by the pediatrician and completed by a nurse during an interview with the parents. The questionnaire included date of birth, gender, type of oral clefts, parents' consanguinity, parental ethnicity and the presence of other congenital anomalies. According to the clinical examination. Newborns with oral clefts were divided into three groups: cleft lip, isolated cleft palate, and cleft lip with cleft palate. The questionnaires were collected and the data were processed using SPSS Version 11.5 software for descriptive analysis. The results was expressed as OR with 95% confidence interval (CI). The significance level was adjusted at p<0.05.
Results
The overall incidence rate of oral clefts during the 6-year period was 1.05 per 1,000 or 1 in 946 live births. Oral clefts were found to be more common in males than females (1.2 vs. 0.86 per 1,000). The male to female relative risk for oral clefts was 1.40 (95% CI: 0.73-2.71); however, the difference was not significant, (Table 1). CP was more common in girls (54%) than in boys (46%) but CL was more common among boys.
According to ethnicity, the incidence rate for oral clefting was 0.7, 1.7 and 1.26 per 1,000 in Native Fars, Turkman and Sistani, respectively, (Table 2). The relative risk for oral clefting in Turkman to native Fars group was 2.56 (p<0.02). Also, the relative risk for oral clefting in Sistani to Fars ethnic group was 1.84; however, the difference was not significant.
The incidence of cleft lip and isolated cleft palate was 0.08 and 0.37 per 1,000 live births, respectively. In this study, 56.7% of clefts were CL+P, 8.1% were CL and 35.1% of cases were CP, (Table 1). The ratio for different cleft types was 1:7:4 (CL: CLP: CP). According to ethnicity, the CL: CLP: CP ratios were 1:10:4, 1:4:4, 1:6:3 in native Fars, Turkman, and Sistani groups, respectively.
The parents of 13 babies were related, 7 couples were first cousins, and 6 were weakly related. In this study, 21.6% of cases with oral clefts had other accompanying congenital anomalies; three with hydrocephalus, two with polydactyli, one with microcephalus, one with hypospadias, and one with microphtalmia. The lowest and highest incidence rates for oral clefts was observed in 2006 and 2007, respectively.
Table 1: Incidence (per 1,000) of oral cleft, isolate cleft lip and isolate cleft palate according to years, and gender in live births in Northern Iran from 2004-2009.
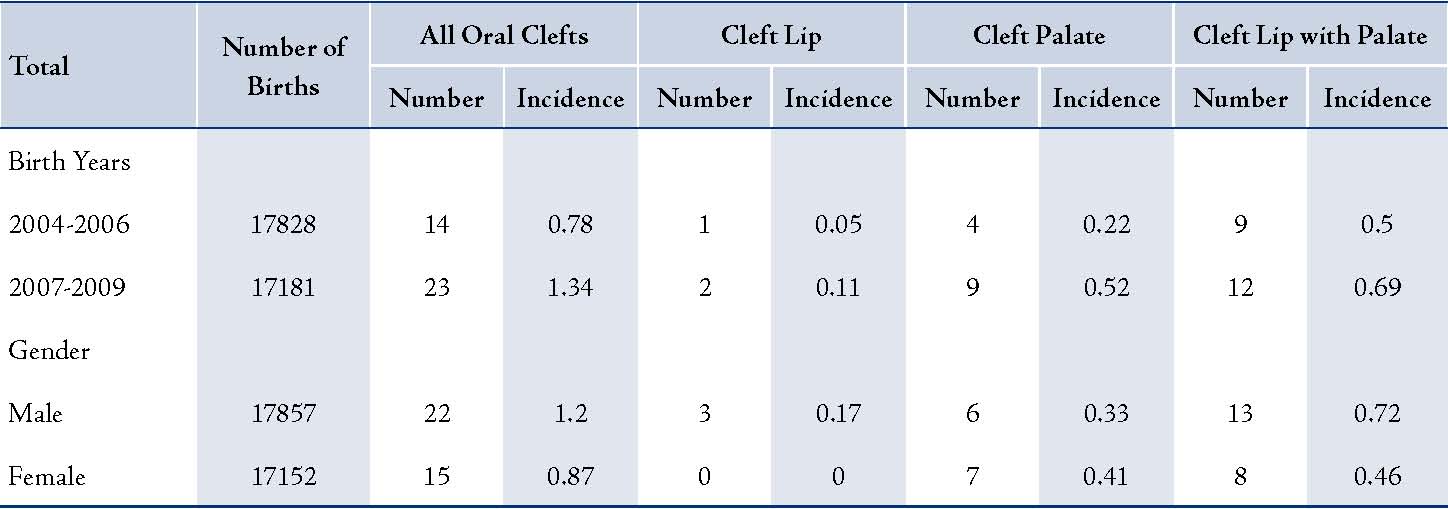
Table 2: Incidence (per 1000) of oral clefts, isolate cleft lip and isolate cleft palate according to ethnicity in live births, North of Iran from
2004-2009.

Table 3: Incidence of Oral clefts in various areas in Iran.

Discussion
In this study, the overall incidence rate of oral clefts was 1.05 per 1,000 live births which is higher than the figure reported by a previous study in Gorgan with 0.97 per 1,000 live births.3 The increase in oral clefts may be due to the immigration phenomenon in the area because this area is a farm land and has good job opportunities. Some low-income families emigrated to the area from southeastern Iran. Another reason may be due to Dezyani Hospital being a referral hospital, i.e., high-risk patients and families of low-socioeconomic status being referred there from other areas of Golestan province.
The rate of oral clefting in this area is higher than those reported in other studies from Hamedan 1.01, Shiraz 0.80, and Yazd 0.86.18,19,20 On the other hand, this rate is lower than the 2.14 per 1,000 births reported for Tehran, (Table 3).21 The incidence rate of oral clefts in this study is higher than the Khazaei study (a meta-analysis of 11 studies in Iran) with 1.0 per 1,000 live births.22 Also, it was reported that the high incidence of oral clefts in Tehran may be due to the use of mustard gas during the Iran-Iraq war,23 but recently in a Jamalian study, consanguinity was reported to be the main risk factor.21 The incidence rate of oral clefts in the current study is lower than the rates reported by studies in Asia: 1.91 for Pakistan, 1.39 for Jordan, 1.76 for Northern China, 1.81 for Korea, 1.34 for Japan, and 1.5 per 1,000 births for Oman.9,24,25,26,27,28
In this study, the incidence rate of oral clefts was lower than the rate reported by studies from Denmark (1.66),29 Netherland (1.68),30 Spain (1.44),31 Canterbury/New Zealand (1.69),32 Bolivia (1.23),33 Argentina (1.7),34 Canada (1.1 to 1.53 in 2002-2008),35 Sweden (2.01),36 USA (1.21),37 and Ethiopia with 1.49 per 1,000 births,38 but the rate was higher than the rate reported from Uganda with 0.73 per 1,000 births.39
More details about the incidence rate of oral clefts in various parts of the world are mentioned in Wyszynski's text.40 Various incidence rates of oral clefting could be related to the influence of social and ethnical/racial factors in different parts of the world, which are commonly explained as genetic disorders. Also, the differences among these findings could be related to the study population, type of classification, and various selection criteria such as live births and still births in the study or eliminating aborted fetus from the study.
The rate of isolated cleft palate was 0.37 per 1,000 live births. This finding is similar to our previous study in Northern Iran,3 but this rate is lower than a report in Tehran with 0.77 per 1,000 births,21 lower than Pakistan with 0.46,9 Canterbury/New Zealand with 0.84,32 and Argentina with 0.46 per 1000 births.34 The rate of cleft lip was 0.08 per 1,000 live births and this rate is lower than that among Jordanian people.24
Oral clefts are found to be more common in boys than girls (1.2 vs. 0.86 per 1000). The male to female relative risk for oral clefts was 1.40 (95% CI: 0.73-2.71). This finding is similar to several studies in Jordan,24 Japan,8 Korea,41 Tanzania,42 Tehran,43 South-Western Iran,19 and our previous study in Northern Iran.3 Also, oral clefting was significantly more common among boys in Japan and Estonia,8,11 and most commonly affected by cleft lip and cleft lip with cleft palate in Pakistan.9
Indeed, the International Perinatal Database of Typical Orofacial Clefts has recently reported that the overall incidence of cleft lip with or without cleft palate was 0.992 per 1,000; cleft lip was 0.328 per 1,000; and cleft lip and palate was 0.664 per 1,000.4
According to ethnicity, the incidence rate of oral clefting in this study was 0.7, 1.7 and 1.26 per 1,000 in Native Fars, Turkman and Sistani, respectively. The relative risk for oral clefting in Turkman to native Fars group was 2.56 (p<0.02). Also, the relative risk for oral clefting among Sistani to Fars ethnic group was 1.84, which was not significant.
Native Fars, Turkman and Sistani are the three main ethnic groups in Gorgan, Norther Iran. Previous researches have pointed to the effect of race/ethnicity on the incidence of oral clefts.5,44-45 Also, it was found that the incidence of oral clefts varies in different populations such as black, Caucasian, Asian, and Native Americans.6 This difference especially in a given population could be related to differences in nutritional habits, environmental exposure or genetic factors.16
In this study, 56.7% of clefts were CLP, 8.1% were CL and 35.1% of cases were CP. The ratio for different cleft types was CL: CLP: CP (ratio 1:7:4). The CL: CLP: CP ratio according to ethnicity groups were 1:10:4, 1:4:4, 1:6:3 in native Fars, Turkmens and Sistani groups, respectively. A previous study by Fogh-Andersen (1942) reported a CL: CLP: CP ratio (1:2:1), which is often described as the normal ratio for different cleft types in Caucasians.46 Also, studies from Japan and Africa revealed a much lower incidence of CP.8,47 Furthermore, a study in Estonia found a high occurrence rate of CP among all clefts (CL: CLP: CP ratio 1:2:2), which was different from the normal Caucasians ratio.11
Regarding the high occurrence rate of CP in all ethnic groups, the study results were similar to the ones observed in Estonia,11 Finland,48 and Sweden.49
In this study, 21.6% of cases with oral clefts were associated with other anomalies including hydrocephalus, polydactyly, microcephalus, hypospadias and microphthalmia. But among Koreans, 8.4% of cases with oral clefting were associated with congenital heart disease, short frenulum, Pierre Robin syndrome, Down syndrome, Patau syndrome, and van der Woude syndrome.41 Recently, a study in USA showed that 15.9% of reported cases had malformations in other systems.4 Another study in Estonia reported that 30.3% of patients with clefts had accompanying developmental anomalies including syndactyly, heart defects, mental and physical retardation and inguinal hernia.11
The absence of stillbirths, small number of cases, limited study period (6 years), as well as the lack of side of cleft proportions, and submucosal clefts were the main limitations of the current study. Also, the ethnicity of 3 cases was not recorded.
Conclusion
The present study shows that the incidence rate of oral clefts in the population as being 1.05 per 1,000 live births, which has increased from 0.97 per 1,000 live births in comparison to an earlier study in this area.
Acknowledgements
We appreciate the personnel of the Pediatric and Gynecology wards at Dezyani Hospital. This study was supported by the deputy research, Golestan University of Medical Sciences (35/6987). The authors declare no conflict of interest.
References
1. Abramowicz S, Cooper ME, Bardi K, Weyant RJ, Marazita ML. Demographic and prenatal factors of patients with cleft lip and cleft palate: A pilot study. J Am Dent Assoc. 2003 Oct;134(10):1371-6.
2. Marazita ML. Genetic etiologies of facial clefting. In: Mooney MP, Siegel MI, eds. Understanding craniofacial anomalies: The etiopathogenesis of craniosynostosis and facial clefting. New York: Wiley, 2002;147-62.
3. Golalipour MJ, Mirfazeli A, Behnampour N. Birth prevalence of oral clefting in northern Iran. Cleft Palate Craniofac J. 2007 Jul;44(4):378-80.
4. [No authors listed]. Prevalence at Birth of Cleft Lip With or Without Cleft Palate: Data from the International Perinatal Database of Typical Oral Clefts (IPDTOC). Cleft Palate Craniofac J. 2011 Jan; 48(1):66-81
5. Vanderas AP. Incidence of cleft lip, cleft palate, and cleft lip and palate among races: a review. Cleft Palate J. 1987 Jul;24(3):216-25.
6. Das SK, Runnels RS Jr, Smith JC, Cohly HH. Epidemiology of cleft lip and cleft palate in Mississippi. South Med J. 1995 Apr;88(4):437-42.
7. Wehby GL, Murray JC. Folic acid and Orofacial Clefts: a review of the evidence. Oral Dis. 2010 Jan;16(1):11-9.
8. Natsume N, Kawai T, Ogi N, Yoshida W. Maternal risk factors in cleft lip and palate: case control study. Br J Oral Maxillofac Surg. 2000 Feb;38(1):23-5.
9. Elahi MM, Jackson IT, Elahi O, Khan AH, Mubarak F, Tariq GB, Mitra A. Epidemiology of cleft lip and cleft palate in Pakistan. Plast Reconstr Surg. 2004 May;113(6):1548-55.
10. Grewal J, Carmichael SL, Ma C, Lammer EJ, Shaw GM. Maternal periconceptional smoking and alcohol consumption and risk for select congenital anomalies. Birth Defects Res A Clin Mol Teratol 2008; 82(7):519-26.
11. Jagomagi T, Soots M, Saag M. Epidemiologic factors causing cleft lip and palate and their regularities of occurrence in Estonia. Stomatologija.2010, 12(4): 105-8.
12. Harden CL, Meador KJ, Pennell PB, Hauser WA, Gronseth GS, French JA, et al. Practice parameter update: management issues for women with epilepsy--focus on pregnancy (an evidence-based review): teratogenesis and perinatal outcomes: report of the Quality Standards Subcommittee and Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology and American Epilepsy Society. Neurology. 2009;73(2):133-41
13. Honein MA, Rasmussen SA, Reefhuis J, Romitti PA, Lammer EJ, Sun L, et al.Maternal smoking and environmental tobacco smoke exposure and the risk of orofacial clefts. Epidemiology. 2007 Mar;18(2):226-33.
14. Little J, Cardy A, Munger RG.Tobacco smoking and oral clefts: a meta-analysis. Bull World Health Organ. 2004 Mar;82(3):213-8.
15. DeRoo LA, Gaudino JA, Edmonds LD.Orofacial cleft malformations: associations with maternal and infant characteristics in Washington State. Birth Defects Res A Clin Mol Teratol. 2003 Sep;67(9):637-42.
16. Croen LA, Shaw GM, Wasserman CR, Tolarová MM. Racial and ethnic variations in the prevalence of orofacial clefts in California, 1983-1992. Am J Med Genet. 1998 Aug 27;79(1):42-7.
17. Gundlach KK, Maus C. Epidemiological studies on the frequency of clefts in Europe and world-wide. J Craniomaxillofac Surg. 2006 Sep; 34 Suppl 2:1-2.
18. Zandi M, Heidari A. An epidemiologic study of Orofacial Clefts in Hamedan city, Iran: A 15- year study. Cleft Palate Craniofac J. 2011 Jul;48(4):483-9.
19. Rajabian MH, Aghaei S. Cleft lip and palate in southwestern Iran: an epidemiologic study of live births. Ann Saudi Med. 2005 Sep-Oct; 25(5):385-8.
20. Yassaei S, Mehrgerdy Z, Zareshahi G, Prevalence of cleft lip and palate in births from 2003 - 2006 in Iran. Community Dent Health. 2010 Jun; 27(2):118-21.
21. Jamilian A, Nayeri F, Babayan A. Incidence of cleft lip and palate in Tehran. J Indian Soc Pedod Prev Dent. 2007 Oct-Dec; 25(4):174-6.
22. Khazaei S, Shirani AM, Khazaei M, Najafi F. Incidence of cleft lip and palate in Iran. A meta-analysis. Saudi Med J . Apr 2011, 32(4) :390-3.
23. Taher AA. Cleft lip and palate in Tehran. Cleft Palate Craniofac J. 1992 Jan; 29(1):15-6.
24. Al Omari F, Al-Omari IK. Cleft lip and palate in Jordan: birth prevalence rate. Cleft Palate Craniofac J. 2004 Nov; 41(6):609-12.
25. Wang W, Guan P, Xu W, Zhou B. Risk factors for oral clefts: a population-based case-control study in Shenyang, China. Paediatr Perinat Epidemiol. 2009 Jul; 23(4):310-20.
26. Kim S, Kim WJ, Oh C, Kim JC. Cleft lip and Palate Incidence among the Live Births in the Republic of Korea. J Korean Med Sci . 2002; 17: 49-52
27. Cooper ME, Ratay JS, Marazita ML. Asian Oral-Facial Cleft Birth Prevalence. The Cleft Palate-Craniofacial Journal: 2006 September; 43(5):580-9.
28. Rajab A, Thomas C. Oral clefts in the Sultanate of Oman. Eur J Plast Surg. 2001;24(5):230-3.
29. Grosen D, Bille C, Petersen I, Skytthe A, Hjelmborg JB, Pedersen JK, et al. Risk of oral clefts in twins. Epidemiology. 2011 May;22(3):313-9.
30. Rozendaal AM, Luijsterburg AJ, Ongkosuwito EM, de Vries E, Vermeij-Keers C. Decreasing prevalence of oral cleft live births in the Netherlands,1997-2006. Arch Dis Child Fetal Neonatal Ed. 2011 May;96(3):212-6.
31. Rodríguez Dehli C, Mosquera Tenreiro C, García López E, Fernández Toral J, Rodríguez Fernández A, Riaño Galán I, et al. [The epidemiology of cleft lip and palate over the period 1990-2004 in Asturias]. An Pediatr (Barc). 2010 Sep;73(3):132-7.
32. Smit R, Fowler PV. Non-syndromal Orofacial clefts in the Canterbury/West Coast region during the 2000-2009 period. N Z Dent J. 2010 Dec;106(4):129-31.
33. McLeod NM, Urioste ML, Saeed NR. Birth prevalence of cleft lip and palate in Sucre, Bolivia. Cleft Palate Craniofac J. 2004 Mar; 41(2):195-8.
34. Rittler M, Cosentino V, López-Camelo JS, Murray JC, Wehby G, Castilla EE. Associated anomalies among infants with oral clefts at birth and during a 1-year follow-up. Am J Med Genet A. 2011 Jul;155(7):1588-96.
35. Pavri S, Forrest CR. Demographics of Orofacial Clefts in Canada from 2002 to 2008. Cleft Palate Craniofac J 2011 In-Press. doi: 10.1597/10-223
36. Amini H, Axelsson O, Ollars B, Anneren G. The Swedish Birth Defects Registry: ascertainment and incidence of Spina bifida and cleft lip/palate. Acta Obstet Gynecol Scand. 2009;88(6):654-9.
37. Genisca AE, Frías JL, Broussard ChS, Honein MA, Lammer EJ, Moore CA, et al. and The National Birth Defects Prevention Study. Orofacial Clefts in the National Birth Defects Prevention Study, 1997-2004 .Am J Med Genet A. 2009 June;149A(6):1149-58.
38. Eshete M, Gravenm PE, Topstad T, Befikadu S. The incidence of cleft lip and palate in Addis Ababa, Ethiopia. Ethiop Med J. 2011 Jan;49(1):1-5.
39. Dreise M, Galiwango G, Hodges A, Incidence of Cleft Lip and Palate in Uganda. Cleft Palate–Craniofacial Journal, 2011 March;48(2):156-60.
40. Mossey PA,Little J.Epidemilogy of oral clefts : An International perspective. In:Wyszynski DF (ed).cleft lip and palate: From origin to treatment. Oxford University press.Oxford.2002; pp: 127-58.
41. Kim S, Kim WJ, Oh C, Kim JC. Cleft lip and palate incidence among the live births in the Republic of Korea. J Korean Med Sci. 2002 Feb;17(1):49-52.
42. Manyama M, Rolian C, Gilyoma J, Magori CC, Mjema K, Mazyala E, et al. An assessment of orofacial clefts in Tanzania. BMC Oral Health. 2011;11:5-11.
43. Sadri D., Ahmadi N. The Frequency of Cleft Lip and Palate and the delated Risk Factors in a Group of Neonates in the City of Kerman during 1994-2002, Journal of Mashhad Dental School 2007;1-2(31):71-76.
44. Amaratunga AN, Chandrasekera A. Incidence of cleft lip and palate in Sri Lanka. J Oral Maxillofac Surg. 1989 Jun;47(6):559-61.
45. Chapman CJ. Ethnic differences in the incidence of cleft lip and/or cleft palate in Auckland, 1960-1976. N Z Med J. 1983 May 11;96(731):327-9.
46. Fogh-Andersen P. Inheritance of harelip and cleft palate. Copenhagen: A. Busck; 1942.
47. Ogle OE. Incidence of cleft lip and palate in a newborn Zairian sample. Cleft Palate Craniofac J. 1993 Mar;30(2):250-1.
48. Rintala AE. Epidemiology of orofacial clefts in Finland: a review. Ann Plast Surg 1986;17(6):456-9.
49. Hagberg C, Larson O, Milerad J. Incidence of cleft lip and palate risks of additional malformations. Cleft Palate Craniofac J 1998;35(1): 40-5.
|
|