Cervical ectopy (CE) can be associated with chronic or recurrent symptoms of cervicitis like leucorrhea, vaginal itching or pruritus, dyspareunia, pelvic pain, and post-coital bleeding, which cause patients to visit a doctor repeatedly.1,2 CE is distinguished by an erythematous and inflamed-like region at the external ostium, which forms due to the eversion of the endocervical columnar mucosal layer towards the outside. CE may be silent and asymptomatic. If symptomatic, it can cause prolonged physical and psychological distress for women due to chronic or recurrent vaginal discharge and discomfort.
Some authors believe that CE may predispose women to contamination of human papillomavirus (HPV). Long-term exposure of everted columnar epithelium to the vaginal environment leads to squamous metaplasia, this rapid cellular generation can be a suitable site for inoculation of HPV during intercourse.1,3,4 Between the 1920s and 1970s, gynecologists widely performed ablation of ectopic epithelium in an attempt to diminish the symptoms of chronic cervicitis and/or reduce susceptibility to lower tract infection or dysplasia. They believed that the elimination of the squamocolumnar junction accelerates the duration of cellular transformation, shortens the time qualified for incorporation and propagation of HPV particles and, subsequently, declines the incidence of cervical intraepithelial neoplasia (CIN).4 However, this disputable topic concerning ablation of benign CE remained quiet for some decades.
In recent years, the importance of ablation of the ectopic zone has been stated to achieve several expectations including relieving symptoms of chronic cervicitis and prevention or treatment of CIN particularly in low-income countries, as they lack the requisite infrastructures for triage, diagnosis, and management.2,5 Various methods have been proposed for damaging the transformation zone.6–9 Cryotherapy is an old and common procedure first introduced in 1960. It consists of a handle device with a metal probe on its tip and a flexible connector that transmits carbon dioxide or nitrous oxide to the probe to freeze and ruin the transformation zone. Although cryotherapy for management of CIN has been advocated by many researchers,3,10,11 its administration for the relief of recurrent or chronic symptoms of benign CE is under debate.12–14
As relevant randomized trials are few in the literature, we sought to determine if cryotherapy can be used as a safe and effective method for relieving symptoms of CE.
Methods
This randomized clinical trial was conducted in the outpatient clinic of Mobini Hospital, Sabzevar, Iran in 2015. After obtaining the approval of the ethics committee (Medsab.Rec.93.3), and taking consent forms (IRCT2014101719559N1), 164 women with chronic or recurrent symptoms of cervicitis whose vaginal examination showed CE were enrolled in the study. The demographic data, medical history, and also frequency, duration, and specifications of symptoms were collected in a checklist.
Inclusion criteria included CE in the visual vaginal examination, complaints of suprapubic pain, increased vaginal discharge (leucorrhea), vaginal itching or pruritus, dyspareunia and post-coital bleeding, normal co-test or Pap smear, lack of sexually transmitted disease, and reproductive age > 21 years. Patients also must be willing to participate in the study. Our criterion for chronicity was the persistence of at least one symptom for at least six months or recurrence of symptoms at least three times in the previous six months despite obtaining treatment. Exclusion criteria were virginity, age < 21 years, past history of CIN, previous cervical ablation procedures and loop electrosurgical excision procedure (LEEP), background diseases associated with immunocompromised conditions (i.e., diabetes mellitus, immunodeficiency syndromes) and use of corticosteroid or immunosuppressive drugs, mental disorders, epilepsy, pregnancy, lactation, menopause, acute vaginal candidiasis, any abnormality in cytology, and positivity of HPV or other sexually transmitted diseases.
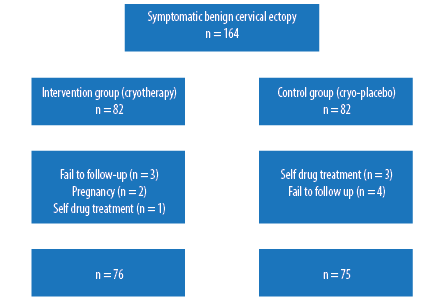
Figure 1: Trial consort diagram.
The 164 eligible women were equally divided into two groups by block randomization; the intervention group and control group. Cryotherapy involves freezing temperatures of -22 to -30 oC, which results in crystallization and evaporation of intracellular fluid and ultimately, demolition of cells at -85 oC. The procedure is performed until the formation of an ice ball, which takes up to five minutes, most often with freeze-thaw cycle.5 In the control group (who underwent demonstrative placebo-cryotherapy), the assistant researcher put the probe near cervical ostium and pressed the trigger without manipulation and destruction of cervical tissue. Patients in both groups received a similar vaginal pharmacologic cream, which started five days after cryotherapy and an appropriate systemic drug. All participants were asked about the severity of symptoms (leucorrhea, vaginal itching, pruritus, pelvic pain, dyspareunia, and post-coital bleeding) using a visual analog scale (VAS) before the procedure. The primary examination was done by a gynecologist, while interventions concerning cryotherapy or placebo took place by a trained midwife. The doctor responsible for examining, determining patient eligibility, and prescribing the proper drug as well as the participants themselves was blinded to the treatment group.
The women attended follow-up visits one, three, and six months post-treatment and their symptoms were reassessed using the VAS and improvement of the CE region inspected speculum. A self-reported questionnaire was used to assess patient’s satisfaction with treatment. Finally, the collected data was entered into SPSS Statistics (IBM Corp. Released 2010. IBM SPSS Statistics for Windows, Version 19.0. Armonk, NY: IBM Corp.) and analyzed using the chi-squared test, Fisher’s exact test, Mann-Whitney U test, t-test, and the level of decreasing symptoms were compared in the two groups. A p-value < 0.050 was considered significant.
Table 1: Patients demographic data.
|
Age, years |
30.2 ± 7.5 |
29.2 ± 6.4 |
0.390 |
|
Marital age, years |
19.4 ± 4.4 |
19.2 ± 3.9 |
0.850 |
|
Marriage length, years |
10.7 ± 8.0 |
9.9 ± 6.8 |
0.490 |
|
Parity |
1.5 ± 1.5 |
1.2 ± 0.9 |
0.660 |
|
Abortion |
0.3 ± 0.5 |
0.3 ± 0.6 |
0.060** |
Data presented as mean±standard deviation.
**Mann-Whitney U test.
Table 2: Prevalence of symptoms experienced by patients before and after treatment in the intervention and control groups.
|
Leucorrhea |
66 (88.0) |
61 (80.3) |
0.141 |
57 (76.0) |
42 (55.3) |
0.006 |
|
Vaginal itching and pruritus |
56 (74.7) |
49 (64.5) |
0.118 |
38 (50.7) |
15 (19.7) |
< 0.001 |
|
Pelvic pain |
51 (68.0) |
52 (68.4) |
0.547 |
40 (53.3) |
25 (32.9) |
0.009 |
|
Dyspareunia |
45 (60.0) |
47 (61.8) |
0.474 |
37 (49.3) |
21 (27.6) |
0.005 |
Fisher’s exact test.
Results
Of the 164 women enrolled in the study, 151 were aged between 21–54 years old and eligible for evaluation [Figure 1]. There demographic details are given in Table 1.
The complaints of the women suffering from symptoms of CE were evaluated before and after the intervention and compared using Fisher’s exact test.The prevalence of symptoms was not significantly different between the two groups before any intervention (p > 0.050).
Following the intervention, the incidence of symptoms in the cryotherapy group decreased significantly compared to the control group (p < 0.001) [Table 2].
Following intervention, the severity of symptoms declined significantly in cryotherapy group compared to the cryo-placebo group (p < 0.050) [Figure 2]. Visual inspection of the CE area showed significant healing following cryotherapy one month after treatment (p < 0.001) [Figure 3].
The transient side effects of suprapubic crampy pain and hot flush, which were seen following the procedure, showed no significant difference between the two groups (p = 0.600 and p = 0.640, respectively). Vaginal discharge in the intervention group was higher than the control group, which took as long as a few days (p < 0.001). Spotting in the control group was greater than the intervention group (p = 0.007). The participants who received cryotherapy were more satisfied with their treatment than the cryo-placebo group (88.2% vs. 22.7%) (p < 0.001).
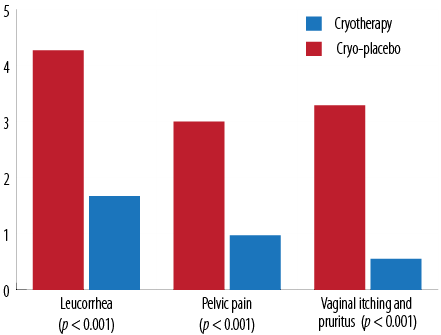
Figure 2: Change in visual analog scale score of symptom severity post-treatment.
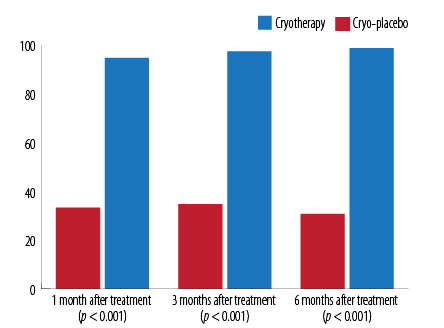
Figure 3: Percentage of participants whose cervical ectopy improved according to the time of examination.
Discussion
Many women suffer from repeated or sustained symptoms of cervicitis worldwide. These symptoms can affect the quality of life and marital relationships and, consequently, affect the health of the family atmosphere. Although some physicians contradict any surgical treatment for benign CE, we advocate its cases where the symptoms are resistant to pharmacological intervention.1,15 We believe that the destruction of the everted glandular layer not only relieves symptoms, but also prevents sexually transmitted infections such as chlamydia, gonorrhea, and HPV. Infection with HPV18 was shown to be more prevalent in women with CE.16
Our study showed that ablation with cryotherapy has an acceptable long-term effect on the treatment of these patients while lacking remarkable side effects. All our participants had already received systemic and topical drugs at least three times without a good response in the six months before the study. Our study supports the results of other researchers who introduced cryotherapy as an acceptable modality for managing symptomatic CE.1,2,17,18 They reported that cryotherapy had the highest efficacy for reducing abundant leucorrhoea, but the lowest success rate for patients with abundant leucorrhea and recurrent cervicitis, which was similar to our findings. They declared that delay in treatment declined the success rate.1,2,17,18
Notably, few harmless side effects including temporary hot flush, abdominal cramps, and leucorrhea were observed in our findings, which were in agreement with previous reports,1–3,5,19 but they did not have any significant impact on the satisfaction rate of our participants. Non-surgical studies using traditional herbal drugs have been done in different areas with contradictory results.8,20 However, the tolerance of the patients to these drugs, probable allergic reactions, and sustainability of their efficacy should be considered and assessed. Other researchers examined topical agent of 70% trichloroacetic acid and monopolar spray coagulation with acceptable results, but reported it was not suitable for hypertrophic CE.17
Other surgical technologies have been applied for ablation of squamocolumnar junction. Electrocautery was the oldest device applied for this purpose since 1920.21 Although it is said that its efficacy for management of benign CE is not different from cryotherapy,18 it has some disadvantages, comparatively. Cauterization needs some precautions; it has the risk of burning lesions if the safeguard plate is not located correctly, and it cannot be used in people with metal prosthetic devices. Another disadvantage is stenosis of the cervix, which has been stated for cauterization more than cryotherapy, has not been proved by evidence-based documents.21 Some authors compared ultrasound with a laser. Both methods appeared effective in relieving symptoms of benign CE with fewer side effects using the laser.21,22 Obviously, the need for expensive facilities and professional experts are considered disadvantages.
Other investigators examined several modalities and declared infrared coagulation was safer than electrocautery and laser, but the latter were more effective for ablation of CE. They believed that impossibility of pointed ablation accounts for a disadvantage regarding cryotherapy.23
Recently, cryotherapy has been more beckoned in new recommended guidelines for cervical cancer screening. Accordingly, in areas with limited resources, which lack required experts and infrastructures for triage and management of CIN like colposcopy or LEEP, cryotherapy has been recommended as a simple and safe method. In these situations, after application of acetic acid on the cervix, acetowhite spots are distinguished by visual inspection and destroyed with cryotherapy simultaneously.24 This approach of ‘see and treat’ has been performed in Ethiopia since 2010.25 Statistically, the efficacy of cryotherapy has been proved for the elimination of cervical dysplasia (CIN1 94%, CIN2 92%, and CIN3 85%). However, the main disadvantage of this modality is the lack of histological samples for evaluation, but it outweighs missing cervical dysplasia, which may progress to invasive neoplasms.24 Additionally, this method has significant advantages including being an outpatient procedure that is safe, simple, and inexpensive.26
Conclusion
Benign CE is a relatively common finding among fertile women. It is typically asymptomatic and may be found incidentally during examination. If it becomes symptomatic, it might be better to apply an ablative approach. Providing a good quality of life for women is essential to have a healthy population. Paying special attention to women with CE who complain of recurrent or chronic distressing symptoms of cervicitis is mandatory. Pharmacotherapy alone is sometimes ineffective and ablation of the ectopic region of cervix remains the final option for management. Cryotherapy is a simple, cost-effective, and safe outpatient treatment for ablative goals. Besides elimination of the symptoms, it can have considerable benefits for the prevention and treatment of CIN, particularly in low resource countries. Further investigations need to warrant the obtained results.
Disclosure
The authors declared no conflict of interest. The study was funded by the Sabzevar University of Medical Sciences.
Acknowledgements
The authors appreciate the Research Deputy of Sabzevar University of Medical Sciences for financial support, and the participants and clinic staff of Mobini Hospital for their cooperation.
references
- 1. Çekmez Y, Şanlıkan F, Göçmen A, Vural A, Türkmen SB. Is cryotherapy friend or foe for symptomatic cervical ectopy? Med Princ Pract 2016;25(1):8-11.
- 2. Gay C, Riehl C, Ramanah R, Desmoulin G, Violaine B. [Cryotherapy in the management of symptomatic cervical ectopy]. Gynecol Obstet Fertil 2006 Mar;34(3):214-223.
- 3. Wesley RS, Muwonge R, Sauvaget C, Thara S, Sankaranarayanan R. Effectiveness of cryotherapy for histologically confirmed cervical intraepithelial neoplasia grades 1 and 2 in an Indian setting. Int J Gynaecol Obstet 2013 Oct;123(1):16-20.
- 4. Franceschi S. Past and future of prophylactic ablation of the cervical squamocolumnar junction. ecancermedicalscience 2015 Apr 29;9:527.
- 5. Mohanty KC, Rand RJ, Berry B. Cryotherapy in the management of cervical ectopy. Genitourin Med 1985 Oct;61(5):335-337.
- 6. Hua X, Zeng Y, Zhang R, Wang H, Diao J, Zhang P. Using platelet-rich plasma for the treatment of symptomatic cervical ectopy. Int J Gynaecol Obstet 2012 Oct;119(1):26-29.
- 7. Li C, Xiong X, Li Y, Li J, Peng B, Wang Z, et al. Therapeutic effects of focused ultrasound in 4014 patients with symptomatic cervical ectopy. Ultrasound Med Biol 2013 Apr;39(4):604-610.
- 8. Mohite S, Kapoor E, Nagarkar B, Mohite SS. Evaluation of efficacy of dashmoolarishta in cervicitis: a proof-of-concept study. World J Pharm Pharm Sci 2014 Apr;3(6):1526-1532.
- 9. Hashmi S, Begum W, Sultana A. Efficacy of Sphaeranthus indicus and cream of Lawsonia inermis in cervical erosion with cervicitis. Eur J Integr Med 2011;3:183-188.
- 10. Sankaranarayanan R, Rajkumar R, Esmy PO, Fayette JM, Shanthakumary S, Frappart L, et al. Effectiveness, safety and acceptability of ‘see and treat’ with cryotherapy by nurses in a cervical screening study in India. Br J Cancer 2007 Mar;96(5):738-743.
- 11. Stienstra KA, Brewer BE, Franklin LA. A comparison of flat and shallow conical tips for cervical cryotherapy. The Journal of the American Board of Family Practice. American Board of Family Practice 1999;12(5):360-366.
- 12. Lewis KD, Sellors JW, Dawa A, Tsu VD, Kidula NA. Report on a cryotherapy service for women with cervical intraepithelial neoplasia in a district hospital in western Kenya. Afr Health Sci 2011 Sep;11(3):370-376.
- 13. Sauvaget C, Muwonge R, Sankaranarayanan R. Meta-analysis of the effectiveness of cryotherapy in the treatment of cervical intraepithelial neoplasia. Int J Gynaecol Obstet 2013 Mar;120(3):218-223.
- 14. Taylor SN, Lensing S, Schwebke J, Lillis R, Mena LA, Nelson AL, et al. Prevalence and treatment outcome of cervicitis of unknown etiology. Sex Transm Dis 2013 May;40(5):379-385.
- 15. Mattson SK, Polk JP, Nyirjesy P. Chronic cervicitis: presenting features and response to therapy. J Low Genit Tract Dis 2016 Jul;20(3):e30-e33.
- 16. Monroy OL, Aguilar C, Lizano M, Cruz-Talonia F, Cruz RM, Rocha-Zavaleta L. Prevalence of human papillomavirus genotypes, and mucosal IgA anti-viral responses in women with cervical ectopy. J Clin Virol 2010 Jan;47(1):43-48.
- 17. Darwish AM, Zahran KM. Trichloroacetic acid application versus spray monopolar diathermy for treating benign cervical lesions: a randomized controlled clinical trial. J Low Genit Tract Dis 2013 Jul;17(3):248-254.
- 18. Jindal M, Kaur S, Sharma S, Gupta KB, Pandotra P. What is better: cryocautery or electrocautery for cervical erosion? Int J Reprod Contracept Obstet Gynecol 2014;3(3):715-719.
- 19. Thida M, Thin KM, Thein ZM, Sein YY, Nyunt T. (2015) Effectiveness, safety and acceptability of the method of visual inspection with acetic acid (VIA) and cryotherapy based single-visit approach to cervical cancer prevention (CCP) in Kungyangon Township, Yangon Region, Myanmar. Myanmar Medical Journal 2015 Sep;57(3):48-56.
- 20. Gupta P, Sharma S. Clinical evaluation of the efficacy of kshara karma with Apamarga kshara and Jatyadi taila pichu in the Management of Cervical Erosion (Karnini Yonivyapada). World J Clin. Pharmacol Microbiol Toxicol 2015 Sep;1(3):43-49.
- 21. Chen J, Zhou D, Liu Y, Peng J, Li C, Chen W, et al. A comparison between ultrasound therapy and laser therapy for symptomatic cervical ectopy. Ultrasound Med Biol 2008 Nov;34(11):1770-1774.
- 22. Li CZ, Wang ZB, Yang X, Tang Y, Wang D, Huang Y, et al. Feasibility of focused ultrasound therapy for recurrent cervicitis with high-risk human papillomavirus infection. Ultrasound Obstet Gynecol 2009 Nov;34(5):590-594.
- 23. Sortey K. Infrared Coagulation of benign erosions of cervix. J South Asian Fed Obstet Gynecol 2014;6(2):104-106.
- 24. Castle PE, Jeronimo J, Temin S, Shastri SS. Screening to prevent invasive cervical cancer: ASCO Resource-Stratified Clinical Practice Guideline. J Clin Oncol 2017 Apr;35(11):1250-1252.
- 25. Deksissa ZM, Tesfamichael FA, Ferede HA. Prevalence and factors associated with VIA positive result among clients screened at Family Guidance Association of Ethiopia, south west area office, Jimma model clinic, Jimma, Ethiopia 2013: a cross-sectional study. BMC Res Notes 2015 Oct;8(1):618.
- 26. Dolman L, Sauvaget C, Muwonge R, Sankaranarayanan R. Meta-analysis of the efficacy of cold coagulation as a treatment method for cervical intraepithelial neoplasia: a systematic review. BJOG 2014 Jul;121(8):929-942.