|
Abstract
Objectives: To determine the prevalence of malaria and anemia among pregnant women attending a traditional birth center as well as the effect of herbal remedies, gravidity, age, educational background and malaria prevention methods on their prevalence.
Methods: Blood specimens were collected from 119 pregnant women attending a Traditional Birth Home in Benin City, Nigeria. Malaria parasitemia was diagnosed by microscopy while anemia was defined as hemoglobin concentration <11 g/dL.
Results: The prevalence of malaria infection was (OR=4.35 95% CI=1.213, 15.600; p=0.016) higher among primigravidae (92.1%). Pregnant women (38.5%) with tertiary level of education had significantly lower prevalence of malaria infection (p=0.002). Malaria significantly affected the prevalence of anemia (p<0.05). Anemia was associated with consumption of herbal remedies (OR=2.973; 95% CI=1.206, 7.330; p=0.017). The prevalence of malaria parasitemia and anemia were not affected by malaria prevention methods used by the participants.
Conclusion: The overall prevalence of malaria infection and anemia observed in this study were 78.9% and 46.2%, respectively. Higher prevalence of malaria infection was associated with primigravidae and lower prevalence with tertiary education of subjects. Anemia was associated with consumption of herbal remedies. There is urgent need to control the prevalence of malaria and anemia among pregnant women attending traditional birth homes.
Keywords: Pregnancy; Malaria Prevention; Herbal treatment; Anemia; Traditional birth attendants.
Introduction
A traditional birth attendant (TBA) has been defined as a person who assists mothers during childbirth and who initially acquires her skills by delivering babies herself or through apprenticeship to other TBAs.1 They are known to form an integral part of most communities, and provide a window to local customs, traditions and perceptions regarding childbirth and newborn-care.2 TBAs, predominantly uneducated,3 presently deliver the majority of women in Nigeria, as in other developing countries.1 It is estimated that between 60-80% of all deliveries in developing countries occur outside modern health facilities, with a significant proportion of these attended to by TBAs.1 The scope of services rendered by TBAs are changing by the day, as reports showing that they also provide care to people at puberty, during pregnancy, labor, and also give advice about child care.4
Malaria during pregnancy is a major health concern and ranks among the commonest complications of pregnancy in Nigeria.5 Complications of malaria in pregnancy include hypoglycemia, acute pulmonary edema, premature labor, spontaneous abortion, still births, low birth weights and anemia.6 In the light of the numerous attendant risks of malaria in pregnancy, WHO recommended a three pronged approach to the strategic framework for malaria prevention and control during pregnancy in areas of stable transmission in Africa. This includes the use of insecticide treated bed nets (ITN), intermittent preventive treatment (IPTP) and effective case management of malaria illness and anemia.7 Reports show that compliance with this recommendation in Nigeria is poor.8 TBAs are largely uneducated,3 and may not appreciate the importance of these recommendations.
Anemia in pregnancy is an important public health problem worldwide,9 and particularly in developing countries where nutritional deficiency, worm infestation and malaria are common.10 Anemia in pregnancy is a well known risk factor for maternal death, still births, low birth weights, and fetal impairment.11 Management and control of anemia in pregnancy is enhanced by the availability of local prevalence statistics, which is not adequately provided in Nigeria.9 Thus, accurate and early diagnosis of malaria illness is key to effective management of the disease.12 Most TBAs do not focus on diagnosis in management of disease, as they often lack the skills and facilities to do so. Studies have also shown that TBAs are largely unable to prevent, or treat most-life threatening obstetric complications.13
Against this background and the paucity of reports on the prevalence of anemia, malaria, type and efficacy of malaria prevention methods employed by pregnant women attending Traditional Birth Centers in Edo-State, Nigeria, this study was undertaken.
Methods
The study was carried out from May to August 2010, a period that coincides with the rainy season in Edo State, Nigeria. Target Institution was a leading Traditional Birth Center located in a suburban area of Evbotubu Quarters, Benin City, Nigeria. One hundred and Nineteen (119) pregnant women with age ranging from 16 - 43 years were selected for this study. Selection criteria included being registered in the center for at least one month, and non-attendance of any other conventional health facility. A detailed questionnaire was formed to assess educational status of the study population, level of awareness and use of insecticide treated bed nets (ITN), as well as other preventive measures they take against malaria. The questionnaire also sought to find out the type of anti-malaria drug (Herbal or conventional) used by them during the course of pregnancy.
The herbal mixture given to them at TBA center is Agbo Iba which is known for its anti-malaria properties in Nigeria.14 Dosage was as prescribed by resident traditional birth attendant. Verbal informed consent was obtained from all participating pregnant women and their spouse. Ethical clearance for this work was given by Edo State Ministry of Health, Benin City. For specimen collection and processing; 5 ml of venous blood was collected from each patient, dispensed into ethylene diamine tetra-acetic acid (EDTA) container, and mixed. Malaria was diagnosed by examination of stained thick blood films as previously described.15 Hemoglobin estimation was determined using the Sysmex KX-21 Hematology analyzer (Sysmex Cooperation, Kobe Japan). Anemia in pregnant women was defined as a hemoglobin concentration <11.0 g/dl.16
The data obtained were analyzed with Chi square (X2) or Fischer’s exact test as appropriate and odd ratio analysis was done using the statistical software INSTAT®. Statistical significance was set at p<0.05.
Results
A total of 94 (78.9%) of the 119 pregnant women were infected with the malaria parasite. The prevalence of malaria parasitemia did not differ significantly between subjects that consumed Agbo Iba solely and those that consumed Agbo Iba alongside other conventional medications. Gravidity was significantly associated with malaria parasitemia (OR=4.350; 95% CI=1.213, 15.600; p=0.016) with higher prevalence among primigravidae subjects. The prevalence of malaria parasitemia was significantly lower among pregnant subjects with tertiary level of education compared with subjects with other levels of education (p=0.002). The age of the studied subjects did not affect the prevalence of malaria parasitemia (p=0.114). (Table 1)
The prevalence of anemia in pregnant women was 46.2%, and was significantly affected by malaria. The use of Agbo Iba alone was associated with anemia (OR = 2.973; 95% C.I =1.206, 7.330; p=0.017), [Table 2]. Gravidity, age and educational status of pregnant women did not significantly affect the prevalence of anemia, (Table 2). In addition, the use of some malaria prevention methods did not significantly affect the prevalence of malaria parasitemia and anemia. (Tables 3 and 4)
Table 1: Effect of age, gravidity, educational status and malaria management method on prevalence of malaria parasitic infection in pregnant women.
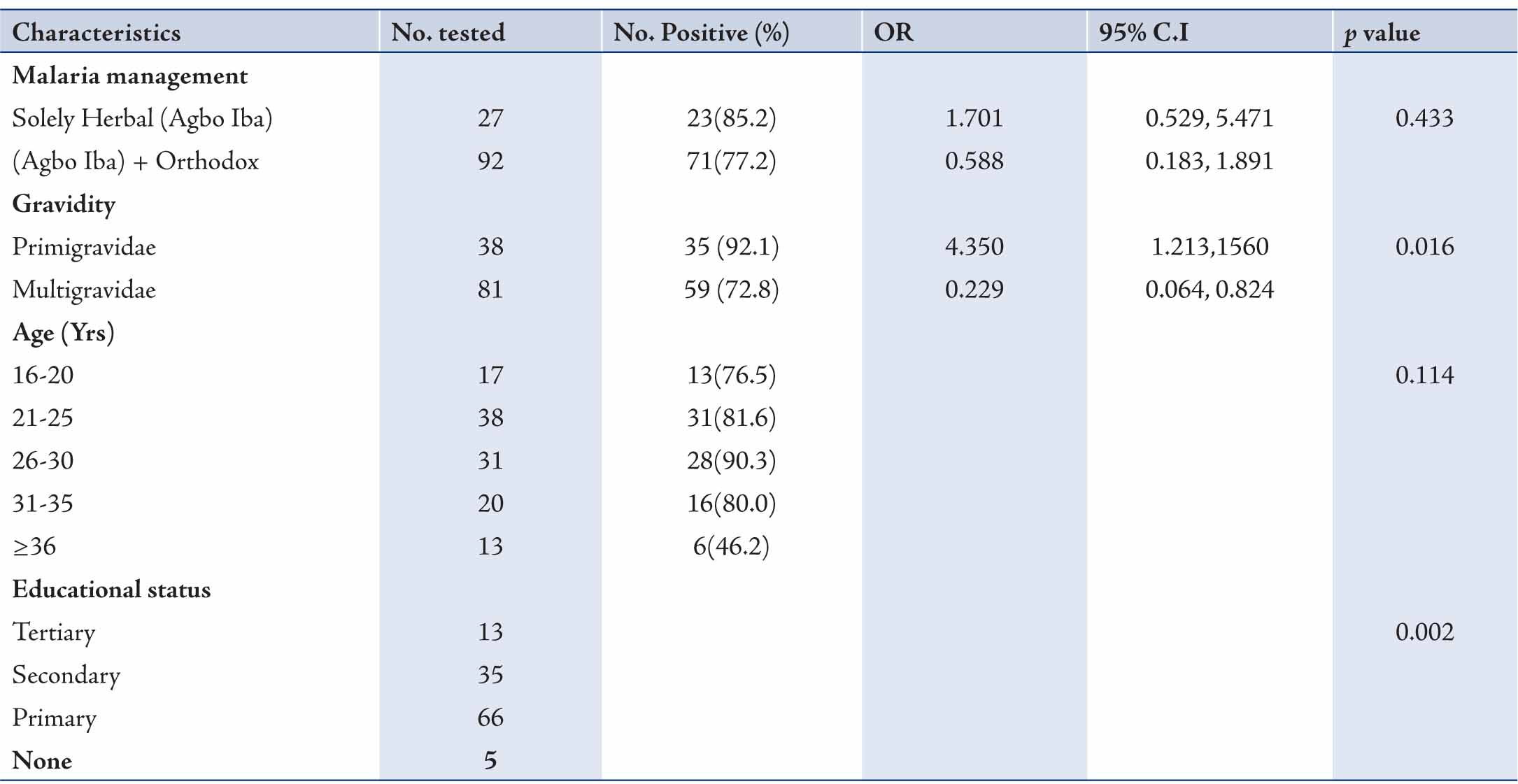
OR-odd ratio; CI- confidence interval
Table 2: Effect of age, gravidity, educational status, malaria parasitemia and malaria management method on the prevalence of anemia in pregnant women.
Table 3: Effect of malaria parasite protection methods on the prevalence of malaria among pregnant women.
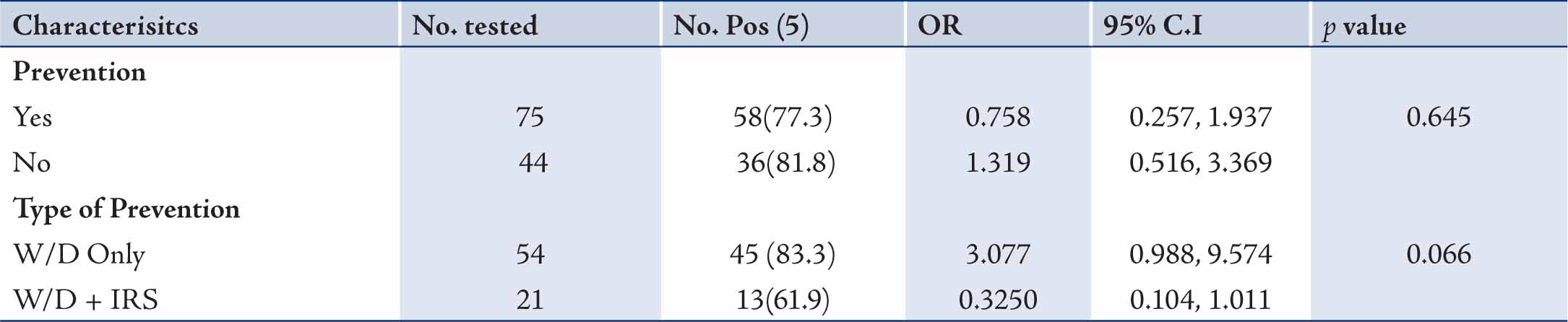
Table 4: Effect of malaria parasite protection methods on the prevalence of anemia among pregnant women.

Discussion
Malaria and anemia are associated with serious mortality and morbidity among pregnant women. Despite the fact that most TBAs are uneducated, they are responsible for 60-80% of deliveries in the developing world.1 This study focused on determining the efficacy of local herbal mixtures used by TBAs in the prevention and treatment of malaria infection. The prevalence of malaria parasitemia observed in this study (78.9%), is higher than that previously reported 62.4%.17 The difference could be due to geographical location, as the study was carried out in Benin City South-South geo-political zone, while that of Idowu et al. was in Abeokuta which is in the South-West geopolitical zone of Nigeria.
Agbo Iba has been reported to have prophylactic action against malaria parasite.18 However in this study; the use of Agbo Iba either solely or in combination with conventional antimalarial drugs did not show any significant difference in the prevalence of malaria. It is possible that the strain of plasmodium falciparum (the only species of plasmodia observed in this study) is resistant to Agbo Iba, as 85.2% of pregnant women who took Agbo Iba alone had malaria parasitemia. This would require further investigation to verify. The high prevalence of malaria parasitemia among pregnant subjects that took Agbo Iba and conventional anti malaria agents may also indicate resistance to either agents or possible antagonistic effect of both combinations. Again this will require further studies to verify. In a similar vein, the prevalence of malaria among pregnant women did not differ significantly within the age range of the study population.
The finding that higher prevalence of malaria parasitemia was associated with primigravidae status had earlier been noted.19,20 It has been reported that Plasmodium falciparium strains may get sequestered in the placenta.21 With successive pregnancies, women are exposed to variety of strains of malaria parasite, and may develop efficient mechanism to control infection and prevent disease.22,23 Primigravidae women have lower immunity against the strains of malaria parasite, hence present more frequently with malaria. The reasons for people with tertiary level of education having a lower incidence of malaria are multifactorial. Persons with tertiary level of education are most likely to live in areas of good sanitary condition and hygiene. That is, areas that may not support the breeding of mosquitoes. Indeed, fewer pregnant women with tertiary education attended the Traditional Birth Home in this study, and had the least prevalence of malaria. It was observed that the malaria therapy is necessary to improve or correct this anemic condition. Generally among pregnant women studied, malaria was found to significantly affect the prevalence of malaria. This has been previously documented.24 There was no difference in the prevalence of anaemia between primigravidae and multigravidae. This is in agreement with a previous report.10
The prevalence of anemia among pregnant women attending traditional Birth Home in this study (46.2%) is lower than that previously reported in Abeokuta (81.2%).10 An important factor to consider is that the etiology of anemia is multifactorial, and thus several underlying morbid and co-morbid conditions could cause wide variations in the prevalence of anemia. Location may also account for this disparity. The use of Agbo Iba solely was significantly associated with anemia among pregnant women attending the Traditional Birth Home. Some antimalarial drugs are known to destroy red blood cells and then exert their activity against the exposed malaria parasite.25,26 This may be the same mechanism by which Agbo Iba functions; however, the Agbo Iba mixture was not effective as high prevalence of malaria was observed in this study. To our knowledge, this is the first report associating Agbo Iba with anemia. The conventional addition of blood building supplements prevention methods used by the pregnant women did not significantly affect the prevalence of malaria parasitemia and anemia. Information from questionnaire revealed that 10 (8.4%) of the 119 pregnant women had knowledge of insecticide treated bed nets, as a method of preventing malaria parasite infection, though none of the subjects had used any. The findings that none of the pregnant women had used Insecticide treated nets had previously been observed.17 There is therefore need for the Government and other intervention agencies to extend malaria control intervention programs to pregnant women attending Traditional Birth Homes with free distribution of insecticide treated bed nets. The specific duration of use of Agbo Iba with or without conventional antimalaria remedies was not noted. The malaria and anemia status of pregnant women prior to consumption of Agbo Iba and the type of conventional anti malaria used were not ascertained. These were limitations observed to the study.
Conclusion
In brief, an overall prevalence of malaria parasitemia and anemia of 78.9% and 46.2%, respectively was observed in this study. The use of Agbo Iba did not significantly affect the prevalence of malaria parasitemia, but it was associated with anemia. Prevalence of malaria parasitemia was higher among primigravidae and least among pregnant women with tertiary level of education. Measures to control malaria infection and anemia among pregnant women attending Traditional Birth Homes are necessary.
Acknowledgements
The authors reported no conflict of interest and no funding was received for this work.
|