Tracheostomy is a common otorhinolaryngology procedure. The procedure has complications, which can be divided into early and late. Common early complications are bleeding, pneumothorax, subcutaneous emphysema, infection, and tracheostomy blockage or dislodgement. Late complications include tracheal stenosis, tracheocutaneous fistula (TCF), trachea-innominate artery erosion, and tracheomalacia. Cervical aerocele following TCF repair is rare.1 Delayed cervical aerocele post-decannulation of tracheostomy without a history of TCF repair is extremely rare.2
Cervical aerocele is an air-filled mass in the neck, which communicates with the tracheal lumen.3 Other terms also used to describe the condition include tracheocele, paratracheal air cyst, and tracheal diverticulum. It is a rare condition and rarely reported in the literature. Pediatric cases usually occur after TCF closure,1,4 or post-cricoid split operation.5,6 In adult patients, it can occur following tracheostomy decannulation.7,8 For patients without any surgical procedure history, aerocele may begin as a congenital weakness in the tracheal wall that increases with forceful cough or increased intratracheal pressure.9 For acquired cervical aerocele, following the surgical procedure, the air cyst forms by air escaping from tracheal wall defect rather than outpouching of tracheal mucosa.
We report a rare case of a patient that developed cervical aerocele eight years post-tracheostomy decannulation, which was aggravated by a prolonged cough.
Case Report
We report a case of 32-year-old, Malay, female with non-syndromic craniofacial anomaly and limb deformity since birth. The patient underwent modified Le Fort III osteotomy with maxillary advancement and bilateral sagittal mandibular split with tracheostomy in July 2007. She was on tracheostomy for one month and was decannulated followed by spontaneous stoma closure. She was well for eight years and presented to our clinic with a two-month history of compressible anterior neck swelling. The swelling appeared during coughing and resolved by compression. It was painless and did not gradually increase in size. Before the symptom, the patient had an episode of prolonged cough. She denied a history of voice changes, difficulty in breathing, noisy breathing, dysphagia, or odynophagia. From neck examination, the tracheostomy scar was well healed. There were no signs of inflammation. The anterior neck swelling only appeared after the patient was asked to cough, it was a single mass, situated over the tracheostomy scar measuring 5 × 5 cm in diameter [Figure 1]. The mass did not move with tongue protrusion or swallowing. The mass margin was well-defined, soft in consistency, crepitus on palpation, and non-tender. It was completely reducible with compression. Flexible nasopharyngolaryngoscopy showed normal findings. We saw no submucosal mass in the false cord suggestive of internal laryngocele and no pooling of saliva. Computed tomography (CT) scan findings showed a superficial lobulated midline lesion at the anterior neck region measuring approximately 2.9 cm (anterior-posterior) × 3.6 cm (width) × 4.3 cm (craniocaudal). The lesion was homogenously hypodense with Hounsfield unit suggestive of air content with no enhancement post-contrast. It was located anterior to the trachea, and there was no communication seen between the mass and trachea [Figure 2].
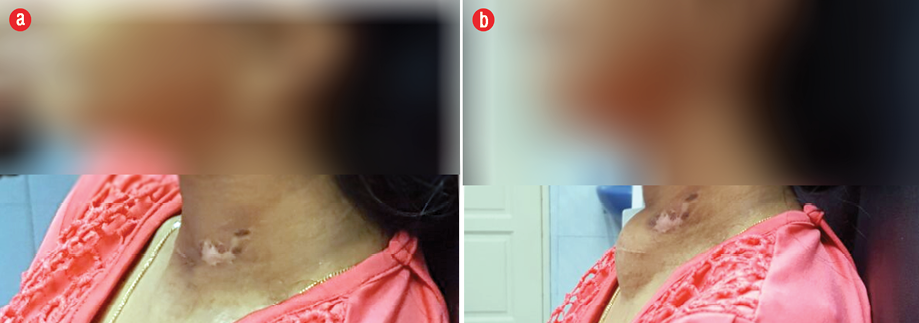
Figure 1: (a) At rest. (b) Post-coughing: swelling over the tracheostomy scar.
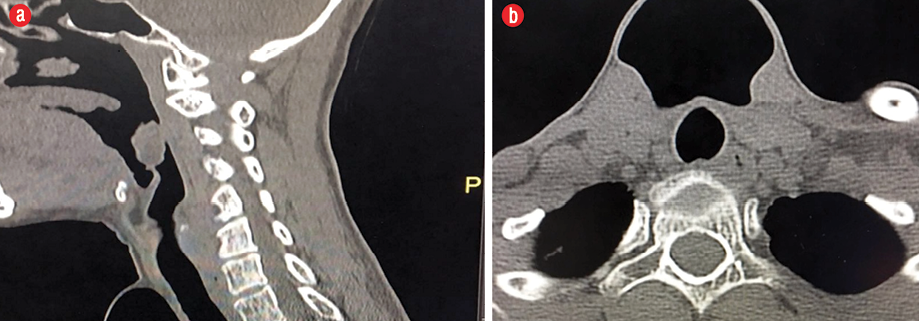
Figure 2:(a) Sagittal and (b) axial view of computed tomography neck scan.
Discussion
Acquired cervical aerocele usually occurs as a complication of TCF closure or repair. TCF is one of the rare delayed complications of tracheostomy. Occurrence of cervical aerocele following TCF repair is very much rare. They have been rarely reported to occur after decannulation of tracheostomy.2 In the literature, three cases of aerocele following decannulation of tracheostomy have been reported in adults7,10 and three cases in children.1,4,11 Two cases were reported 10 years after decannulation2,10 and two cases occurred a few months after decannulation.4,7 Our patient developed cervical aerocele eight years after decannulation following an episode of prolonged cough. In our patient, prolonged cough was the significant risk factor for aerocele. It may be due to bouts of intense increased intratracheal pressure causing a fistula between the trachea and the deep space of the neck.
Acquired cervical aerocele can be asymptomatic or with non-specific symptoms. However, they may present with pharyngeal discomfort and cough with or without phlegm.12 Our patient presented with a history of neck swelling over the tracheostomy scar which was reducible by compression and reappeared during cough. From clinical presentations, the diagnosis of cervical aerocele is very likely although CT scan reported no communication between the mass and trachea. CT scan can help diagnose the aerocele. By definition, cervical aerocele should have a connection with the trachea, but the connection stalk can be tiny and not demonstrated on CT scan.13 Some literature reported that CT scan sometimes did not show any communication especially in cases of very narrow opening or those joined to the trachea by a fibrous tract. A communicating stalk between the aerocele and the trachea is seen in approximately half of cases.14 Besides CT scan, three-dimension reconstruction technology may help to diagnose cervical aerocele accurately. The communication will usually be identified during bronchoscopy or surgical procedure. However, our patient refused the bronchoscopy procedure and excision of the mass.
There are only few articles published on the treatment of cervical aerocele. In asymptomatic patients, no surgical intervention is required, and treatment is conservative. However, for symptomatic cases, surgical intervention is needed. Most cases reported the treatment of aerocele as bronchoscopy and surgical decompression with or without
insertion of drain and pressure dressing. An alternative surgical procedure is removal of the cyst via an external approach and closing the communication using absorbable suture under general anesthesia.15 Due to the rarity of these cases, there is little data reported on either surgical technique and any postoperative complications.16
Conclusion
Cervical aerocele is a rare condition and patients may present with a compressible neck swelling without any other symptoms. CT scan is sometimes unable to show the connection between the mass and trachea, and three-dimensional reconstruction technology is helpful in establishing any communication between the cyst and trachea. Asymptomatic patients should be treated conservatively while symptomatic patients are recommended surgical intervention.
Disclosure
The authors declared no conflicts of interest.
references
- 1. Rosbe KW, Logan TC, Drake AF. Aerocele: an unusual complication of tracheocutaneous fistula repair. Ann Otol Rhinol Laryngol 1996 Dec;105(12):994-995.
- 2. Staffieri C, Blandamura S, Marioni G. Acquired tracheal diverticulum after tracheotomy. Am J Otolaryngol 2013 Sep-Oct;34(5):614-615.
- 3. O’Neal JP, Wood WE, Gilroy PA, O’Donnell TR. Cervical aerocele in a tracheotomy dependent pediatric patient. Int J Pediatr Otorhinolaryngol 2004 May;68(5):589-592.
- 4. Bent JP 3rd, Smith RJ. Aerocele after tracheocutaneous fistula closure. Int J Pediatr Otorhinolaryngol 1998 Jan;42(3):257-261.
- 5. Patel H, Gregor MB, Kleinhaus S. Aerocele, an unusual complication of anterior cricoid split. J Pediatr Surg 1992 Dec;27(12):1512-1514.
- 6. Drake AF, Babyak JW, Niparko JK, Koopmann CF. The anterior cricoid split. Clinical experience with extended indications. Arch Otolaryngol Head Neck Surg 1988 Dec;114(12):1404-1406.
- 7. Henderson CG, Harrington RL, Izenberg S, Dyess DL, Silver FM. Tracheocele after routine tracheostomy. Otolaryngol Head Neck Surg 1995 Oct;113(4):489-490.
- 8. Lotan AN, Eliachar I, Joachims HZ. Pretracheal air cyst: late complication of tracheostomy. Arch Otolaryngol 1977 Oct;103(10):596-597.
- 9. Scholl PD. Adult tracheocele. Otolaryngol Head Neck Surg 1994 Oct;111(4):519-521.
- 10. Chin AT, Borg HK, Chew C, Houghton D. Pre-tracheal air cyst. J Laryngol Otol 2004 Sep;118(9):730-731.
- 11. Briganti V, Tavormina P, Testa A, Oriolo L. Giant tracheocele following primary tracheostomy closure in a 3 year old child. Interact Cardiovasc Thorac Surg 2004 Jun;3(2):411-412.
- 12. Bodet Agustí E. Martínez Vecina V, Romeu Figuerola C, Monzón Gaspà M. [Tracheal diverticulum: a case report]. Acta Otorrinolaringol Esp 2007;58(6):278-279.
- 13. Gayer G. Tracheal Diverticula. Semin Ultrasound CT MR 2016 Jun;37(3):190-195.
- 14. Buterbaugh JE, Erly WK. Paratracheal air cysts: a common finding on routine CT examinations of the cervical spine and neck that may mimic pneumomediastinum in patients with traumatic injuries. AJNR Am J Neuroradiol 2008 Jun;29(6):1218-1221.
- 15. Pop S, Tazi A, Stirbu C. “Air Cyst” of the neck. Eur Ann Otorhinolaryngol, Head Neck Dis 2013 Sep;130(4):237-240.
- 16. Boyaci N, Sen Dokumaci D, Karakas E, Yalcin F, Oney Kurnaz AG. Paratracheal air cysts: prevalence and relevance to pulmonary emphysema and bronchiectasis using thoracic multidetector CT. Diagn Interv Radiol 2015 Jan-Feb;21(1):42-46.