A 71-year-old male initially presented with history of greenish discharge from the skin over the site of an implanted pacemaker. He had a medical history of hypertension, dyslipidemia, carotid sinus hypersensitivity status post dual chamber pacemaker implant (five years prior), and abdominal aorta aneurysm repair. He was given a course of oral antibiotics without any improvement and was referred to our center for cardiovascular implantable electronic device extraction. As part of the workup, he underwent transesophageal echocardiography (TEE) to assess any pathology before removal. We then performed a cardiac computed tomography (CT).
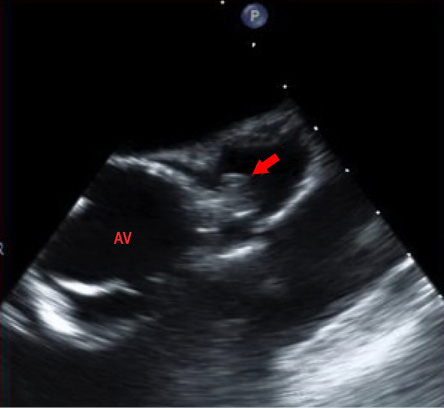
Figure 1: Transesophageal echocardiography with mass-like lesion in the periaortic region. AV: Aortic valve.
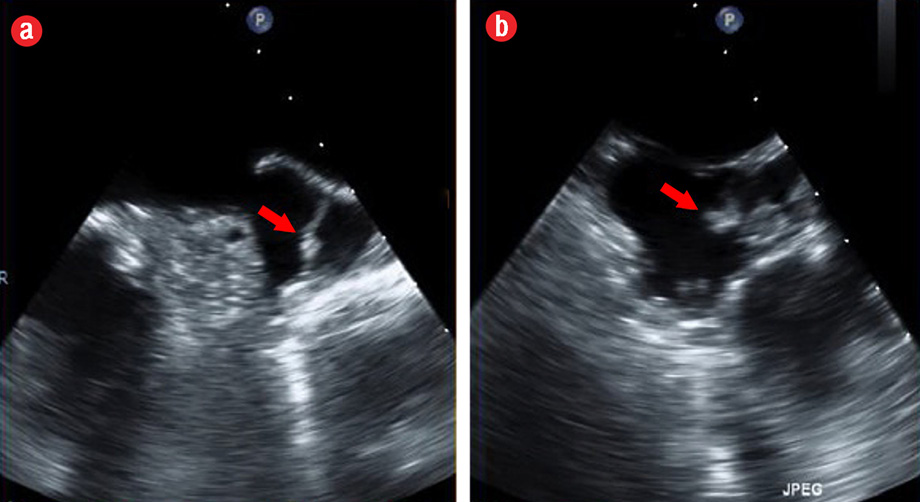
Figure 2: Transesophageal echocardiography image showing the mass-like lesion in the pericardial (transverse) sinus, but not in left atrial appendage.
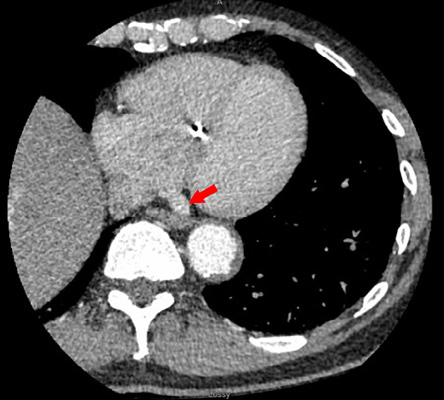
Figure 3: Cardiac computed tomography image showing the prominent transverse sinus (red arrow).
Question
- What is the diagnosis?
a. Left atrial appendage (LAA) thrombus.
b. Vegetation on the aortic valve.
c. Aortic root abscess.
d. Prominent pericardial transverse recess.
e. Pericardial fat.
Answer
d. Prominent pericardial transverse recess.
Discussion
Two-dimensional TEE demonstrated a 0.8 × 0.9 cm echodensity consistent with a mass lesion that was well circumscribed and mobile [Figure 1]. On X-plane TEE, the mass was possibly adjacent to the aortic valve or near the aortic root and LAA [Figure 2]. A cardiac CT confirmed the presence of a prominent transverse pericardial recess without any thrombus or vegetation [Figure 3].
For lesions that do not follow the usual characteristics or are in odd locations, it is advisable to proceed with other imaging modalities. In our case, TEE images were suggestive of a possible periaortic mass in a patient with positive blood cultures and possible endocarditis. However, cardiac CT [Figure 3] confirmed the diagnoses of prominent pericardial transverse recess.
The pericardium consists of an outer fibrous envelope and an inner serous sac surrounding the heart.1 The serous pericardium is further divided into a visceral layer, which covers the heart and great vessels, and a parietal layer, which lines the fibrous pericardium.1 The former is reflected from the heart along the great vessels and onto the parietal pericardium. At these reflections and between the great vessels, recesses or sinuses are formed within the pericardial space.1 One of these recesses is the transverse recess. Clinically, detectable pericardial fluid can accumulate in this space (often the superior borders) forcing the space to extend beyond its normal boundaries. For this reason, pericardial recesses can sometimes create the appearance of a mobile mass on TEE. Incorrect identification of a mass as a LAA thrombus would initiate unnecessary anticoagulation therapy or potential evaluation for excision of the mass if there is a concern for dislodgement. In other cases, it can mimic an aortic root abscess, which may require surgical removal. Previous case studies reported similar appearance of prominent transverse sinus, which was mistaken for LAA mass/thrombus initially.2
Our case highlights the importance of careful examination of the LAA and adjacent structures during 2D TEE.3 If 2D TEE is inconclusive, additional studies such as 3D TTE4 or cardiac CT5 may be indicated to identify suspicious
cardiac lesions.
Disclosure
The authors declared no conflict of interest.
references
- Levy-Ravetch M, Auh YH, Rubenstein WA, Whalen JP, Kazam E. CT of the pericardial recesses. AJR Am J Roentgenol 1985 Apr;144(4):707-714.
- 2. Giove GC, Singla I, Mishra J, Nanda NC. Transesophageal echocardiographic finding of left atrial appendage lobe mimicking a mass lesion. Echocardiography 2011 Jul;28(6):684-685.
- 3. Karakus G, Kodali V, Inamdar V, Nanda NC, Suwanjutah T, Pothineni KR. Comparative assessment of left atrial appendage by transesophageal and combined two- and three-dimensional transthoracic echocardiography. Echocardiography 2008 Sep;25(8):918-924.
- 4. Agoston I, Xie T, Tiller FL, Rahman AM, Ahmad M. Assessment of left atrial appendage by live three-dimensional echocardiography: early experience and comparison with transesophageal echocardiography. Echocardiography 2006 Feb;23(2):127-132.
- 5. Żurada A, Ustymowicz A, Loukas M, Michalak M, Czyżewska D, Gielecki J. Computerized tomography of the transverse pericardial sinus: Normal or pathologic? Clin Anat 2017 Jan;30(1):61-70.