Psoriasis is a chronic inflammatory skin disease with diverse etiologies. Patients with psoriasis have been purported to have increased risk of cardiovascular diseases (CVD), both being T-helper-1/17 mediated chronic inflammatory diseases.1 Studies show that both psoriasis and atherosclerosis evolve through common pathogenic mechanisms, the persistent inflammation being the trigger.1,2 Inflammation results in increased oxidative stress and the release of reactive oxygen species (ROS), leading to oxidative damage to tissues and oxidative modification of lipoproteins, increasing their atherogenicity and contributing to atherosclerotic CVD.2
Oxidized low-density lipoprotein (ox-LDL) is considered an early marker of oxidative stress and lipid peroxidation.3 It is proinflammatory, causing oxidative damage to lipids and proteins, damaging the skin integrity and is also implicated in the evolution and progression of atherosclerosis. Ox-LDL is immunogenic, leading to the formation of antibodies against them. The role of these antibodies is still controversial, dependent on different epitopes of ox-LDL and different types of antibodies. Though studies claim they are atheroprotective, various studies still show the presence of their immune complexes in atherosclerotic lesions.4,5 Thus, the estimation of the levels of antibodies against oxidized LDL (anti-ox-LDL) help in evaluating the pathogenesis of psoriasis and atherosclerotic processes. Assessment of the ratio of anti-ox-LDL/ox-LDL would serve as a composite parameter to study their role in the pathogenesis of psoriasis and its comorbidity, CVD.
We sought to assess the ratio of anti-ox-LDL/ox-LDL as a cardiovascular risk marker in patients with psoriasis and compare this to a control group to identify its association with disease severity.
Methods
This research was part of a cross-sectional study6 conducted at the Departments of Biochemistry and Dermatology of Jawaharlal Institute of Postgraduate Medical Education and Research, Pondicherry, India. We included 45 patients with psoriasis vulgaris who attended the psoriasis clinic of our hospital, a tertiary care center in South India, and 45 age and gender-matched healthy volunteers. Ethical approval was obtained from the Institute’s Human Ethics Committee. The study protocol conformed to the ethical guidelines of the Declaration of Helsinki from 1975 as revised in 1983.7
Written informed consent was obtained from all study subjects. Patients with malignancies, hepatic and renal disease, diabetes mellitus, inflammatory disease, and pregnancy were excluded from the study. For all patients with psoriasis, a psoriasis area severity index (PASI) score was determined independently by two dermatologists and the mean value computed. Ox-LDL and anti-ox-LDL were estimated using commercially available ELISA kits (Cusa Biotech Co. Ltd, China and Immco Diagnostics Inc, USA), respectively.
Statistical analysis was done using SPSS Statistics (SPSS Statistics Inc., Chicago, US) version 22. Data were described as mean ± standard deviation (SD). Levels of ox-LDL and anti-ox-LDL between cases and controls were compared using the independent Student’s t-test. Correlation of the anti-ox-LDL/ox-LDL ratio with PASI was done by Pearson’s correlation. A p-value < 0.050 was considered statistically significant.
Results
The baseline characteristics of the subjects in the two groups were comparable.6 The mean age of the patients was 44.9±14.3 years in the psoriasis group and 42.6±11.3 years in the control group (p = 0.398). There were 36 males and nine females giving a 4:1 male to female ratio in both groups. The mean body mass index (BMI) of the psoriasis group was 22.9±3.4 and 23.0±2.2 in the control group (p = 0.910). The mean PASI score for patients with psoriasis was 14.0±8.3, and the mean duration of psoriasis was 44.4±61.7 months.6
Table 1: Comparison of study parameters between the two groups.
|
Ox-LDL, mU/mL |
31.8±3.2 |
25.5±4.6 |
< 0.0001 |
|
Anti-ox-LDL, EU/mL |
38.9±13.0 |
13.2±3.4 |
< 0.0001 |
|
Ox-LDL/LDL |
0.4±0.1 |
0.3±0.1 |
0.313 |
Ox-LDL: oxidized LDL; Anti-ox-LDL: antibody against oxidized LDL.
*Unpaired t-test.
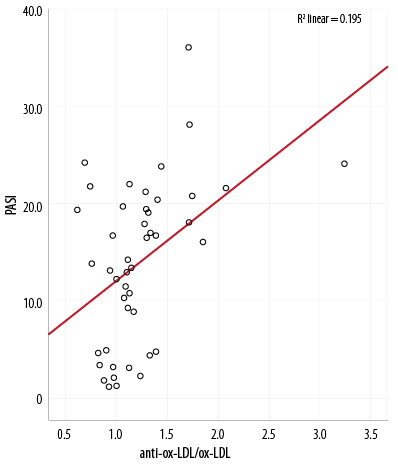
Figure 1: Scatter plot showing Pearson’s correlation of anti-ox-LDL/ox-LDL with PASI (r = 0.441,
p = 0.002).
We found significantly higher levels of ox-LDL and anti-ox-LDL in the case group compared with the control group indicating an elevated oxidative stress in psoriatic patients [Table 1]. Moreover, this study observed a significantly higher ratio of anti-ox-LDL/ox-LDL (a composite marker of oxidative lipoprotein burden and hence CVD risk) in the case compared to control group [Table 1]. There was no significant difference in anti-ox-LDL/ox-LDL between males (1.2±0.5) and females (1.3±0.4) (p = 0.761).
Our results showed that the anti-ox-LDL/ox-LDL ratio correlated significantly with disease severity, its levels increasing linearly with increasing severity [Figure 1].
Discussion
Ox-LDL plays important roles in the evolution of atherosclerosis, including activation of monocytes, leading to their infiltration and smooth muscle cell proliferation.3 Atherosclerosis is initiated by the accumulation of oxidatively modified LDL within plaques, which release ROS. Accumulation of ox-LDL in psoriatic skin also plays a role in the immune-inflammatory events resulting in progressive skin damage.8 Ox-LDL has several epitopes that are antigenic, resulting in the generation of antibodies. The anti-ox-LDL level is an indirect reflection of the in vivo oxidation of LDL. Measuring anti-ox-LDL levels might aid in understanding the relationship between oxidative processes and the development of atherosclerosis.4,5
Though a recent study by Gerdes et al9 was not able to demonstrate a significant difference in the levels of ox-LDL between psoriatic and control patients, most recent studies have reported the obverse. Tekin et al8 reported significantly higher ox-LDL and anti-ox-LDL levels in patients with psoriasis compared to controls. They observed that accumulation of ox-LDL was markedly increased especially in the upper epidermis and absent in non-lesional skin. The results of this study were consistent with that of the previous studies, demonstrating significantly higher levels of ox-LDL in psoriasis.
Ox-LDL induces development and progression of atherosclerosis more effectively than native lipoproteins. Ox-LDL has been shown to activate many downstream signaling pathways via its action on lectin-like ox-LDL receptor-1, contributing to the pathogenesis of atherosclerosis.10
In various studies done in patients with CVD, there is a hot debate whether anti-ox-LDL is associated with CVD. Bergmark et al11 showed by multivariate analysis that anti-ox-LDL might discriminate better between patients with atherosclerosis and control subjects than any other parameters of lipoprotein profile. Moohebati et al12 suggested that serum levels of anti-ox-LDL immunoglobulin (Ig)-G are not associated with the presence and severity of CVD.Orem et al5 observed that 42% of case group patients and 3.3% of the controls had higher anti-ox-LDL than the cut-off point, which correlated positively with PASI. In agreement with their findings, our study observed significantly higher levels of anti-ox-LDL in patients with psoriasis, which correlated with disease severity. These antibodies have been identified to have controversial roles. IgG anti-ox-LDL form immune complexes with ox-LDL and are atherogenic. IgM anti-ox-LDL aid in removing the deposited ox-LDL and are protective.4
We did not characterize the type of anti-ox-LDL antibody and was a limitation of this research. We did not find a statistically significant difference in the ratio of anti-ox-LDL/ox-LDL between male and female subjects. Though gender is expected to influence atherosclerotic risk, the above finding might be due to the predominance of the male gender in the recruited subjects. Moreover, to avoid the possible influence of gender on atherosclerotic risk, we recruited gender-matched controls. Other limitations of this study include a small sample size and lack of follow-up after treatment.
Conclusion
We identified a significantly increased ratio of anti-ox-LDL/ox-LDL in patients with psoriasis compared to controls, which increased linearly with increasing disease severity. Hence, our results suggest that an elevation in the ratio of anti-ox-LDL/ox-LDL can serve as a composite parameter reflecting the total oxidative lipoprotein burden in these patients. This places them at an increased risk from immune-mediated pathogenic events, which is crucial in the pathogenesis of psoriasis and its comorbid condition, atherosclerosis, which is the main cause of mortality in these patients. Its positive correlation with disease severity might warrant early treatment. Hence, statin therapy and antioxidant supplementation may be useful in psoriasis to reduce oxidation of LDL and oxidative stress, thereby rectifying the imbalance of proinflammatory to anti-inflammatory milieu to ameliorate the associated comorbidities.
Disclosure
The authors reported no conflicts of interest. Intramural funding was received from the Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry, India.
references
- 1. Wakkee M, Thio HB, Prens EP, Sijbrands EJ, Neumann HA. Unfavorable cardiovascular risk profiles in untreated and treated psoriasis patients. Atherosclerosis 2007 Jan;190(1):1-9.
- 2. Rocha-Pereira P, Santos-Silva A, Rebelo I, Figueiredo A, Quintanilha A, Teixeira F. Dislipidemia and oxidative stress in mild and in severe psoriasis as a risk for cardiovascular disease. Clin Chim Acta 2001 Jan;303(1-2):33-39.
- 3. Nilsson J, Nordin Fredrikson G, Schiopu A, Shah PK, Jansson B, Carlsson R. Oxidized LDL antibodies in treatment and risk assessment of atherosclerosis and associated cardiovascular disease. Curr Pharm Des 2007;13(10):1021-1030.
- 4. Gounopoulos P, Merki E, Hansen LF, Choi SH, Tsimikas S. Antibodies to oxidized low density lipoprotein: epidemiological studies and potential clinical applications in cardiovascular disease. Minerva Cardioangiol 2007 Dec;55(6):821-837.
- 5. Orem A, Cimşit G, Değer O, Orem C, Vanizor B. The significance of autoantibodies against oxidatively modified low-density lipoprotein (LDL) in patients with psoriasis. Clin Chim Acta 1999 Jun;284(1):81-88.
- 6. Sunitha S, Rajappa M, Thappa DM, Chandrashekar L, Munisamy M, Revathy G, et al. Comprehensive lipid tetrad index, atherogenic index and lipid peroxidation: Surrogate markers for increased cardiovascular risk in psoriasis. Indian J Dermatol Venereol Leprol 2015 Sep-Oct;81(5):464-471.
- 7.WWorld Medical Association. The Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects First adopted in 1964 (Helsinki, Finland) and revised in 1975 (Tokyo, Japan), 1983 (Venice, Italy), 1989 (Hong Kong), 1996 (Somerset-West, South Africa) and 2000 (Edinburgh, Scotland). Note of clarification, 2002 (Washington). 1996 Oct.
- 8. Tekin NS, Tekin IO, Barut F, Sipahi EY. Accumulation of oxidized low-density lipoprotein in psoriatic skin and changes of plasma lipid levels in psoriatic patients. Mediators Inflamm. 2007; 2007:78454.
- 9. Gerdes S, Osadtschy S, Buhles N, Baurecht H, Mrowietz U. Cardiovascular biomarkers in patients with psoriasis. Exp Dermatol 2014 May;23(5):322-325.
- 10. Mitra S, Goyal T, Mehta JL. Oxidized LDL, LOX-1 and atherosclerosis. Cardiovasc Drugs Ther 2011 Oct;25(5):419-429.
- 11. Bergmark C, Wu R, de Faire U, Lefvert AK, Swedenborg J. Patients with early-onset peripheral vascular disease have increased levels of autoantibodies against oxidized LDL. Arterioscler Thromb Vasc Biol 1995 Apr;15(4):441-445.
- 12. Moohebati M, Kabirirad V, Ghayour-Mobarhan M, Esmaily H, Tavallaie S, Akhavan Rezayat A, et al. Investigation of serum oxidized low-density lipoprotein IgG levels in patients with angiographically defined coronary artery disease. Int J Vasc Med. 2014; 2014: 845960.