|
Abstract
Transient osteoporosis of the hip (TOH) is a rare condition mainly affecting pregnant women in their third trimester and middle aged men. We report a case of TOH/Bone marrow edema syndrome in pregnancy with involvement of the surrounding soft tissues on magnetic resonance image, which has not been previously reported. The presence of such edema in the soft tissues may help to differentiate this condition from early avascular necrosis of the hip, and may also provide an insight into the pathogenesis of the condition. The reported patient was treated conservatively and fully recovered.
Keywords: Osteoporosis; Transient; Ischemia; MRI.
Introduction
Transient osteoporosis of the hip (TOH) is a rare condition of unclear aetiology characterized by hip pain, limited osteopenia on plain radiography and characteristic magnetic resonance image (MRI) findings. The condition was first described by Curtis and Kincaid in 1959.1 It mostly affects pregnant women, often in their third trimester and middle aged men. Diagnosis is usually made based on the clinical background and the radiological images including plain film, bone nuclear scan, and MRI in addition to excluding the other potential causes of hip pain, especially avascular necrosis of the femoral head. MRI findings include diffuse bone marrow edema (BMED) involving the femoral head, neck, and sometimes the intertrochanteric area, and a small joint effusion is invariably present.2 Bone marrow edema (BMED) syndrome may be used instead of transient osteoporosis (TO), where osteopenia could never be documented, however the distinction based on osteopenia is somewhat arbitrary.2
To our best knowledge; the occurrence of edema in the surrounding soft tissue on MRI has not been previously reported. TOH usually has a benign course with expected full recovery in most of the cases; however, femoral neck fracture has been reported as a complication.3
Case Reports
A 28 year old female, gravida 2, who was in her third trimester (24 weeks) of her pregnancy began to have left lateral proximal thigh pain, which progressed over a few days to shooting pain radiating from the thigh to the knee and leg. The pain was aggravated with weight bearing activity, and after a few days she started to have limping gait and within two weeks, she was unable to perform daily activities and was bedbound. There was no history of trauma, numbness, backache, fever or other constitutional symptoms; neither was there joints pain or swelling, skin rash or urinary symptoms. Medical, surgical and gyne-obstetric histories were significant only for the first trimester miscarriage.
Physical examination revealed that she was hemodynamically stable and afebrile, having no tenderness over the hip region or skin changes, but the movement (both active and passive) of her left hip joint was restricted due to severe pain, her sensation in the left lower limb was intact and the rest of her examination was unrevealing. Her basic laboratory investigations (CBC, coagulation profile, U&E, LFT, Urine analysis) were normal and MRI pelvis (done about 20 after the pain) revealed evidence of bone marrow edema in the left intertrochanteric region of the femur (the edema was of low signal intensity on T1 weighted images and high signal intensity on T2 weighted images and was not suppressed with fat) with somewhat sparing of the subchondral region with associated effusion and edema in the surrounding soft tissues, (Figs. 1, 2). The patient refused to have plain X-ray, thus we were unable to perform the nuclear bone scan because of the pregnancy.
The patient was managed with analgesics, bed rest and prophylactic subcutaneous low molecular weight heparin. One month later, the pain regressed and we were able to stop the analgesics after 7 weeks. She delivered electively at 39 weeks +2 days gestation by cesarean section to avoid possible trauma to the hip during vaginal delivery. On the first post operative day; she complained of severe pain in the contra-lateral side of the hip of the same character and severity to the previous pain and was managed in the same way as with her first presentation. Fortunately this time, the pain lasted for only a few days and disappeared, she had another MRI of the pelvis after about five months from the first one, which showed bone marrow edema involving the right upper femoral epiphysis, upper femoral metaphysic and upper part of the femoral diaphysis extending to the greater trochanter, relatively sparing the subcortical region of the femoral head. Some patchy areas of bone marrow edema were also noted in the right acetabulum. No MR evidence of joint effusion and the surrounding muscles were free from the edema. Her left side showed small areas of residual oedema in the greater trochanter. Two months after delivery, the patient was almost pain free and returned back to her usual activities of daily living. MRI was repeated 18 months after her first presentation and showed complete recovery of the left hip and a significant reduction in the right sided trochanteric edema. (Fig. 3)
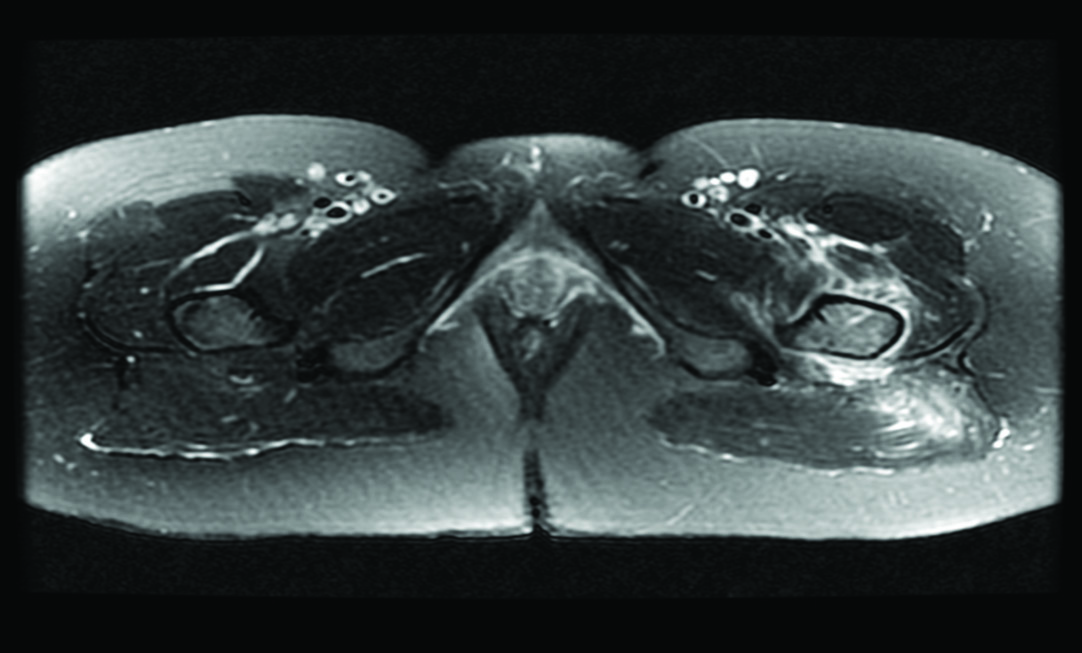
Figure 1: Axial STIR images-left intertrochanteric region of the femur shows bone marrow edema; left intertrochanteric region of the femur manifested by bright signal in the bone with extension to the soft tissues (gluteus maximus).
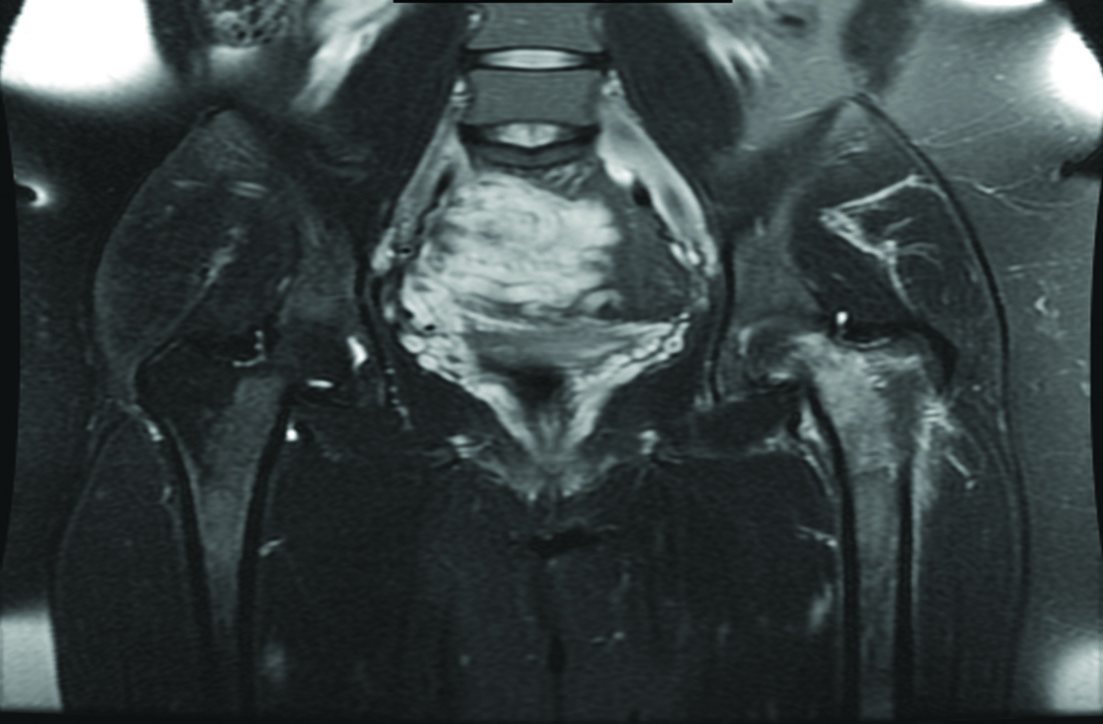
Figure 2: Coronal STIR images shows bone marrow edema left intertrochanteric region of the femur manifested by bright signal.
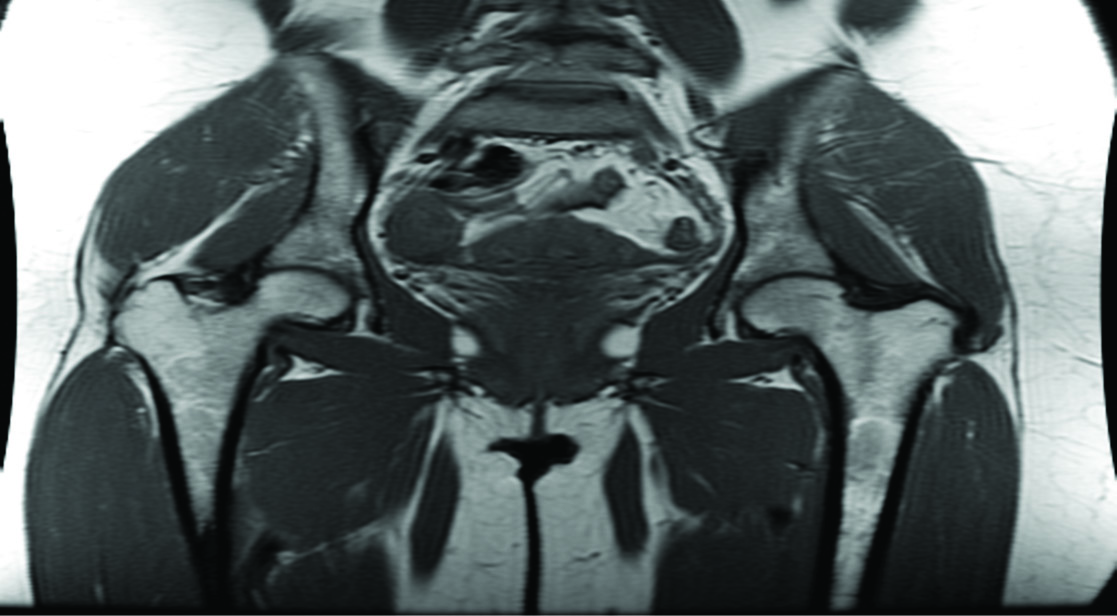
Figure 3: Cornoal T1 MRI pelvis shows significant reduction of right sided trochanteric edema and complete recovery of left sided.
Discussion
Disabling migratory hip pain during the third trimester and in postpartum period with the associated bone marrow edema on MRI and complete clinical and radiological recovery makes transient osteoporosis of the hip the most likely diagnosis in this case despite lack of osteoporosis documentation. BMED syndrome may be used accurately to describe this case radiologically in view of not having evidence of osteoponia; however, the distinction between TOH and BMED syndrome is somewhat arbitrary.2
TOH is a rare condition occurring mainly in the third trimester of pregnancy and postpartum period as well as in middle aged men, and is associated with characteristic MRI finding but the associated soft tissue edema on MRI as in our case was not mentioned previously. The exact etiology of this condition is unknown and different mechanisms have been proposed to explain the etiopathogenesis of TOH that include microvascular injury, abnormal mechanical stress, metabolic, neurological, endocrine, among others.4 Angiographical and scintigraphical studies have shown that nutrient arteries of the femoral head are dilated and the perfusion in this area is higher than in the unaffected contra-lateral side suggesting that ischemia is the most likely cause.5,6 Edema in the surrounding area of the femoral hip (as in our case) may favor the theory of ischemia as the underlying mechanism of this condition. In our case, the edema was evident during the period of pain and occurred concurrently with the edema in the femoral head, and both signs disappeared simultaneously, thus supporting the association rather than a chance occurrence.
The differential diagnosis of TOH includes; avascular necrosis of the femoral head (AVN), infective arthritis/osteomyelitis, stress fracture of neck of femur, radiculopathy, infiltrative marrow process and inflammatory joint disease.4 Usually it is not difficult to differentiate between TOH and the other mentioned conditions except for early AVN, which may occasionally manifest radiologically as diffuse bone marrow oedema pattern on MRI.2 However, other imaging studies may be helpful such as evidence of osteopenia on plain film and diffusely increased uptake on bone scan which are in favor of TOH.7 In the case of AVN, sclerosis followed by articular surface flattening, subchondral collapse and finally end stage degenerative joint disease are the changes seen at different stages on plain radiography.8 Bone scan shows decreased uptake of the isotope over the anterosuperior region of the femoral head and is surrounded by an area of increased uptake due to reactive hyperaemia, forming a cold in hotspots, this is pathognomonic to AVN and is never seen in TOH.9 MRI may be the only feasible way to differentiate between TOH and AVN during pregnancy. If AVN is still considered as a differential for diffuse bone marrow odema pattern on MRI, the edema in the surrounding soft tissue if present probably support TOH over AVN. It is of critical importance to differentiate between these two conditions because the course of the disease as well as the management differs significantly.
Management of TOH is usually conservative and by avoiding weight bearing activity; as well as analgesics; oral, intravenous and intramuscular bisphosphonates.10,11 Calcitonin, prednisolone, and the bone-sparing steroid, as well as deflazacort have also been used.10 However, the fact that this condition frequently occurs in pregnant women limits the choices of pharmacotherapy.
We feel that cesarean section is preferable to vaginal delivery to avoid the risk of trauma to the weak head of femur in cases of TOH. The outcome of this condition is usually excellent in the majority of cases and it takes about 12-24 months to a complete remission.10,12 Care should be taken to avoid the possible complication of femoral neck fracture if the condition is missed or improperly managed.3
Conclusion
Disabling hip pain in the last trimester should be seriously evaluated to exclude the potential causes of significant impact if missed or improperly treated such as TOH. MRI findings of edema in the surrounding soft tissue may support ischemia as the underlying mechanism of TOH and may support TOH diagnosis over early AVN. TOH usually has a benign course with conservative management.
Acknowledgements
The authors reported no conflict of interest and no funding was received on this work.
References
1. Curtiss PH Jr, Kincaid WE. Transitory demineralization of the hip in pregnancy. A report of three cases. J Bone Joint Surg Am 1959 Oct;41-A:1327-1333.
2. Hayes CW, Conway WF, Daniel WW. MR imaging of bone marrow edema pattern: transient osteoporosis, transient bone marrow edema syndrome, or osteonecrosis. Radiographics 1993 Sep;13(5):1001-1011, discussion 1012.
3. Willis-Owen CA, Daurka JS, Chen A, Lewis A. Bilateral femoral neck fractures due to transient osteoporosis of pregnancy: a case report. Cases J 2008;1(1):120. .
4. Harrington S. Idiopathic TOH. Physician Sports Med 2000;28(4):34.
5. Koo KH, Ahn IO, Song HR, Kim SY, Jones JP Jr. Increased perfusion of the femoral head in transient bone marrow edema syndrome. Clin Orthop Relat Res 2002 Sep;402(402):171-175.
6. Malizos KN, Zibis AH, Dailiana Z, Hantes M, Karachalios T, Karantanas AH. MR imaging findings in transient osteoporosis of the hip. Eur J Radiol 2004 Jun;50(3):238-244.
7. Guerra JJ, Steinberg ME. Distinguishing transient osteoporosis from avascular necrosis of the hip. J Bone Joint Surg Am 1995 Apr;77(4):616-624.
8. Vande Berg BC, Malghem JJ, Lecouvet FE, Jamart J, Maldague BE. Idiopathic bone marrow edema lesions of the femoral head: predictive value of MR imaging findings. Radiology 1999 Aug;212(2):527-535.
9. Diwanji SR, Cho YJ, Xin ZF, Yoon TR. Conservative treatment for transient osteoporosis of the hip in middle-aged women. Singapore Med J 2008 Jan;49(1):e17-e21.
10. La Montagna G, Malesci D, Tirri R, Valentini G. Successful neridronate therapy in transient osteoporosis of the hip. Clin Rheumatol 2005 Feb;24(1):67-69.
11. Ma FY, Falkenberg M. Case reports: transient osteoporosis of the hip: an atypical case. Clin Orthop Relat Res 2006 Apr;445:245-249.
12. Arayssi TK, Tawbi HA, Usta IM, Hourani MH. Calcitonin in the treatment of transient osteoporosis of the hip. Semin Arthritis Rheum 2003 Jun;32(6):388-397.
|