|
Abstract
Objective: This study aimed to detect the cytomorphological changes in buccal mucosa among alcoholics and cigarette smokers.
Methods: Buccal smears were collected from 200 volunteers; 50 were alcoholics, 50 were cigarette smokers, 50 were alcoholic and cigarette smokers, and another 50 were treated as a control group (neither drinkers nor smokers). The smokers and alcoholics included in this study had been continuously exposed for more than 5 years. Smears were stained using the Papanicolaou technique.
Results: The cytological assessment in the alcoholics group revealed; atypical cellular changes detected in four individuals, bacteria was found in smears of 16 individuals; 18% cocci and 14% actinomyces species were also detected. Hyperkeratosis was detected in five individuals, while 25 individuals showed no oral changes. In the smokers group; atypical cellular changes were seen in six individuals and bacteria were detected in the smears of 15 individuals; 18% cocci and 12% Actinomyces species. Hyperkeratosis was observed in 14% of the individuals, but 44% showed no oral cytological changes. In the cigarette smoking and alcoholics group; atypical cellular changes were detected in only 14%, while bacteria were detected in 54% of smears; 32% were cocci and 16% were Actinomyces species. Changes in cells infected by human papilloma virus were detected in 4% and monilia in 2% of the cases. Also, 20% of the individuals showed hyperkeratosis and 12% showed no lesions.
Conclusion: The study proved that alcohol and cigarette smoking are risk factors for oral atypical cellular changes and possibly of oral infection. The degree of change depends on the duration of alcohol consumption and cigarette smoking.
Keywords: Oral cytology; Cigarette smoking; Alcoholics.
Introduction
Oral cancer is one of the six most common cancers in the world,1 and is one of ten major causes of death across the globe.2 It is a disfiguring disease prevalent among middle-aged adults and is associated with low survival rate.3 Two thirds (2/3) of oral squamous cell carcinoma and 75% of head and neck cancer can be attributed to tobacco use and alcohol consumption.4,5 The risk increases with the frequency of exposure.6 A recent study showed that 48% of head and neck cancer patients were alcoholics.7 While, tobacco smoking has been observed to be associated with increasing risk of oropharangeal cancer and oral leukoplakia.8 Most oral cancers are preceded by precursor lesion, which could be of great help in early diagnosis. Oral cytology, which is largely based on the presence of nuclear or cytoplasmic alterations, can easily be performed to detect cancer at an early stage and to establish quantitative techniques.9-11 This study aims to investigate the cytomorphological changes in the buccal mucosa and the association with cigarette smoking and alcohol consumption.
Methods
Two hundred cytological materials were randomly collected from volunteers in Khartoum state, Sudan; 50 of the total volunteers were alcoholics (have taken more than 21 standard drinks per week), 50 were regular cigarette smokers, 50 were both alcohol drinkers and cigarette smokers; while another 50 volunteers were considered as a control group who were neither drinkers nor smokers. Each participant was well informed about the study and signed a written ethical consent form before participating in the study. The study was approved by Ethical Committee, College of Medical Laboratory Research Board, Sudan University of Science and Technology.
Buccal smears were taken from the subjects by scraping; using a brush and tongue depressor. Smears were fixed immediately in 95% ethyl alcohol for 15 minutes and eventually stained, adopting the Papanicolaou procedure. Quality control measures were adopted during sample collection and processing. For cytological assessment; each smear was examined for atypia, presence of bacteria or fungi, leukocytes and keratinization. Atypia was recognized when one or more of the following was observed: disturbed chromatin distribution, alteration in nuclear size, increased nuclear DNA content, prominent nuclear, multi nucleation, abnormal nuclear line, hyperchoromatosis and cytoplasmic vacuolations. Data were analyzed using the SPSS computer program. Frequencies, cross tabulation and chi-square were calculated.
Results
The age and sex of the study participants are presented in Table 1. One hundred and thirty-three (88.7%) of the participants were males and 17 (11.3%) were females; age ranged from 20-75 years. The cytopathological changes observed in the buccal smears are depicted in Table 2. Cell atypia was detected in 4 (8%), 6 (12%) and 7 (14%) cases among the alcoholics group, smokers group and in the alcoholics and smokers group, respectively. Hyperkeratosis was observed in all groups; the highest form was detected in the alcoholics and smokers group, while the lowest form was detected in the alcoholic group; 10 (20%) and 5 (10%) of cases, respectively. Changes in cells infected by human papilloma virus were detected in 4% and monilia in 2% of the cases. Also, 20% of the individuals showed hyperkeratosis and 12% showed no lesions.
Table 1: Distribution of the study population by age and sex.
|
Age group
(Years)
|
Sex of study group
|
Sex of control group
|
Total
|
|
Male
|
Female
|
Male
|
Female
|
|
N
|
%
|
N
|
%
|
N
|
%
|
N
|
%
|
|
20-30
|
65
|
43.3
|
0
|
0.0
|
13
|
26.0
|
10
|
20.0
|
88
|
|
31-40
|
35
|
23.3
|
5
|
3.3
|
8
|
16.0
|
4
|
8.0
|
52
|
|
41-50
|
19
|
12.7
|
9
|
6.0
|
5
|
10.0
|
4
|
8.0
|
37
|
|
51-60
|
7
|
4.7
|
3
|
2.0
|
3
|
6.0
|
3
|
6.0
|
16
|
|
61-70
|
5
|
3.3
|
0
|
0.0
|
0
|
0.0
|
0
|
0.0
|
5
|
|
> 70
|
2
|
1.3
|
0
|
0.0
|
0
|
0.0
|
0
|
0.0
|
2
|
|
Total
|
133
|
88.6
|
17
|
11.3
|
29
|
58
|
21
|
42
|
200
|
Cocci and actinomyces bacterial species were detected in all the groups; the alcoholics constituted the highest cases (n=16; 32%), while the smokers group accounted for the lowest frequency (n=8; 16%). Nuclear enlargement changes indicating the presence of human papilloma virus (HPV) were observed in only some buccal smears of alcoholics and smokers group, (Table 2). In addition, only six cases in the latter group showed no cytological changes in their smears in comparison to 25 cases in the alcoholics group, and 22 cases in the smokers group.
Table 2: Frequency of cytopathological results among the study population.
|
Results
|
Study group
|
Control group
|
|
Alcohol consumption
|
Cigarette smoker
|
Cigarette and alcohol abuse
|
|
N
|
%
|
N
|
%
|
N
|
%
|
N
|
%
|
|
Atypia
|
4
|
8
|
6
|
12
|
7
|
14
|
0
|
0.0
|
|
Hyperkeratosis
|
5
|
10
|
7
|
14
|
10
|
20
|
0
|
0.0
|
|
Coccal infections
|
9
|
18
|
9
|
18
|
16
|
32
|
6
|
12.0
|
|
Actinomyces infections
|
7
|
14
|
6
|
12
|
8
|
16
|
0
|
0.0
|
|
HPV(infected cells)
|
0
|
0
|
0
|
0
|
2
|
4
|
0
|
0.0
|
|
Monilia
|
0
|
0
|
0
|
0
|
1
|
2
|
0
|
0.0
|
|
No cytological changes
|
25
|
50
|
22
|
44
|
6
|
12
|
44
|
88.0
|
|
Total
|
50
|
100
|
50
|
100
|
50
|
100
|
200
|
100
|
In the control group (neither smokers, nor alcoholics); neither cell atypia nor hyperkeratosis was observed. But in the smears of 6 (12%) subjects, bacteria (cocci and actinomyces species) were detected. Furthermore, it was reported that 24, 17 and 5 participants used to drink liquor, beer or both liquor and beer respectively, in the alcoholics group. Yet, only two subjects from the participants who drink liquor or both liquor and beer showed cell atypia in their buccal smears.
Discussion
The present results report the causes of oral cell changes among cigarette smoking and alcohol drinking subjects, which are strongly related to cancer risks. The risk tends to increase with the duration of smoking and alcohol consumption; the longer an individual is exposed to smoking and alcohol consumption, the higher the risk.12 Exposure to ethanol with or without tobacco smoking has been found to be associated with carcinogenic cytological changes.13 Anderson et al. examined 276 oral smears from alcoholics, and observed a significant increase in the number of dyskeratotic cells compared to controls.14 Prolonged alcohol consumption is reported to be the cause of pathological changes in oral mucosa including dysplasia, keratosis and increased mitotic figures,15 and increased nuclear cytoplasmic ratio has also been observed.16
In this study, cell atypia was not observed in liquor drinkers. It is claimed that most prevalent alcohol beverages heavily consumed in a given population usually cause most cytological changes.17-19 A high risk of oropharangeal and esophageal cancer is commonly associated with spirit consumption and wine drinking, rather than beer.20
This study suggests that cigarette smoking and alcohol consumption are more common among younger individuals (43.3%), followed by subjects aged between 30-40 years (23.3%). These individuals are subjected to greater risks of developing oral pathological changes, which may lead to cancer; thus the risk is thought to increase with prolonged exposure.21 The appearance of bacteria in some smears of all the studied groups coupled with the presence of leukocytes, indicated that oral infections may be established in association with cigarette smoking or alcohol consumption.
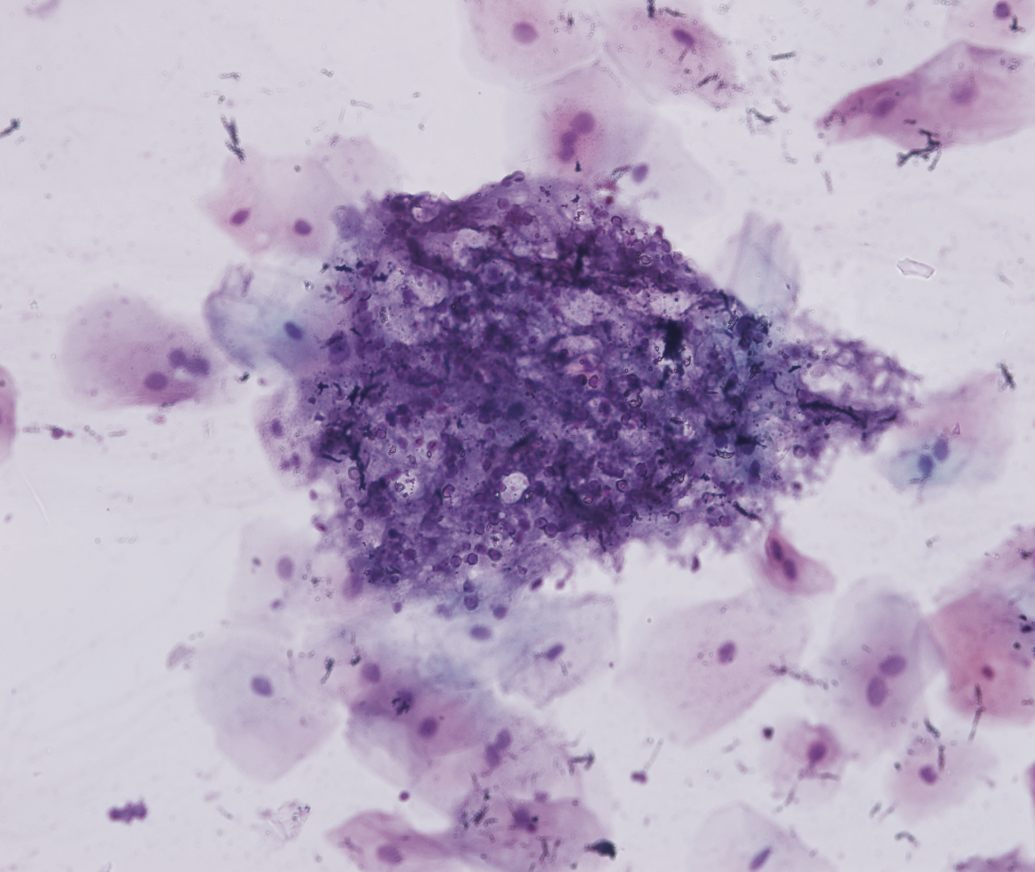
Figure 1: Microphotograph of buccal smear taken from individual, cigarette smokers and alcoholics showing monilia infection through Pap-stains (40×).
Another observation was that the cytopathological changes indicative of HPV was only detected in the alcoholics and smokers group, suggesting that the two habits increase susceptibility to infection. Alcohol consumption may lead to the accumulation of pathogenic microbes within the oral mucosa leading to chronic infection.22 Moreover, alcohol is also considered to reduce memory, salivation and inflammatory responses favoring bacterial multiplication.23,24 Castellsagu et al. reported that simultaneous exposure to both alcohol and tobacco increases the risk of oral cancer by 13-fold.21 Furthermore, heavy alcohol consumption and smoking have been identified as primary risk factors for nearly 80% of oral malignancies.25
Conclusion
Alcohol consumption and cigarette smoking are risk factors for oral atypical cellular changes and possibly oral infection. The degree of change depends on the duration of alcohol consumption and cigarette smoking.
Acknowledgements
The authors reported no conflict of interest and no funding was received for this work.
References
1. Gupta PC, Sinor PN, Bhonsle RB, Pawar VS, Mehta HC. Oral submucous fibrosis in India: a new epidemic? Natl Med J India 1998 May-Jun;11(3):113-116.
2. Razavi SM, Sajadi S. Epidemiological Study of Oral and Perioral Cancers in Isfahan. Dent Res J 2007;4(1):18-25.
3. Castellsagu¥ EX, Quintana M, Maria C, Adoracio¥ NN, Maria J, Amparo J, et al. The role of type of tobacco and type of alcoholic beverage in oral carcinogenesis. International Union against. Cancer 2004;108(2):741-749.
4. Kademani D. Oral cancer. Mayo Clin Proc 2007 Jul;82(7):878-887.
5. Hashibe M, Brennan P, Benhamou S, Castellsague X, Chen C, Curado MP, et al. Alcohol drinking in never users of tobacco, cigarette smoking in never drinkers, and the risk of head and neck cancer: pooled analysis in the International Head and Neck Cancer Epidemiology Consortium. J Natl Cancer Inst 2007 May;99(10):777-789.
6. Morse DE, Psoter WJ, De La Torre Feliciano T, Cruz G, Figueroa N. Detection of very early oral cancers in Puerto Rico. Am J Public Health 2008 Jul;98(7):1200-1202.
7. Kapil U, Singh P. Nutritional Risk Factors in Oral Carcinoma. Pakistan Journal of Nutrition 3.2004; (6):366-370.
8. Mayne ST, Morse DE, Winn DM. Cancers of the oral cavity and pharynx. In: Schottenfeld D, Fraumeni JF Jr (eds) Cancer epidemiology and prevention. Oxford University Press, New York, 2006;674–696.
9. Johnson N. Tobacco use and oral cancer: a global perspective. J Dent Educ 2001 Apr;65(4):328-339.
10. Paiva RL, Sant’Ana Filho M, Bohrer PL, Lauxen IdaS, Rados PV. AgNOR quantification in cells of normal oral mucosa exposed to smoking and alcohol. A cytopathologic study. Anal Quant Cytol Histol 2004 Jun;26(3):175-180.
11. Koss LG. Koss's Diagnostic Cytology and its Histopathologic Bases. 5th ed. New York Lippincott company 2006:11.
12. Winn DM. Tobacco use and oral disease. J Dent Educ 2001 Apr;65(4):306-312.
13. Reis SR, do Espírito Santo AR, Andrade MG, Sadigursky M. Cytologic alterations in the oral mucosa after chronic exposure to ethanol. Braz Oral Res 2006 Apr-Jun;20(2):97-102.
14. Anderson DL. Intraoral site distribution of malignancies and preinvasive malignant cell transformations in dental patients and alcoholics. Acta Cytol 1972 Jul-Aug;16(4):322-326.
15. Müller P, Hepke B, Meldau U, Raabe G. Tissue damage in the rabbit oral mucosa by acute and chronic direct toxic action of different alcohol concentrations. Exp Pathol 1983;24(2-3):171-181.
16. Einstein TB, Sivapathasundharam B. Cytomorphometric analysis of the buccal mucosa of tobacco users. Indian J Dent Res 2005 Apr-Jun;16(2):42-46.
17. Garrote LF, Herrero R, Reyes RM, Vaccarella S, Anta JL, Ferbeye L, et al. Risk factors for cancer of the oral cavity and oro-pharynx in Cuba. Br J Cancer 2001 Jul;85(1):46-54.
18. Kjaerheim K, Gaard M, Andersen A. The role of alcohol, tobacco, and dietary factors in upper aerogastric tract cancers: a prospective study of 10,900 Norwegian men. Cancer Causes Control 1998 Jan;9(1):99-108.
19. Schlecht NF, Pintos J, Kowalski LP, Franco EL. Effect of type of alcoholic beverage on the risks of upper aerodigestive tract cancers in Brazil. Cancer Causes Control 2001 Sep;12(7):579-587.
20. Grønbaek M, Becker U, Johansen D, Tønnesen H, Jensen G, Sørensen TI. Population based cohort study of the association between alcohol intake and cancer of the upper digestive tract. BMJ 1998 Sep;317(7162):844-847.
21. Huang WY, Winn DM, Brown LM, Gridley G, Bravo-Otero E, Diehl SR, et al. Alcohol concentration and risk of oral cancer in Puerto Rico. Am J Epidemiol 2003 May;157(10):881-887.
22. Riedel F, Goessler U, Hörmann K. Alcohol-related diseases of the mouth and throat. Best Pract Res Clin Gastroenterol 2003 Aug;17(4):543-555.
23. Wight AJ, Ogden GR. Possible mechanisms by which alcohol may influence the development of oral cancer–a review. Oral Oncol 1998 Nov;34(6):441-447.
24. Xelsson AP. External modifying factors involved in periodontal diseases. Karlstad, Sweden: quintessence publishing Co. Inc 2005;3:95-119.
25. WHO. Oral Health Country/Area Profile Programme. Department of Noncommunicable.Diseases Surveillance/Oral Health. WHO Collaborating Centre, Malmö University, Sweden, 2001;231.
|