
Persistent Wheeze Following ACS
Kowthar Hassan
Hassan K. OMJ. 25, 143-144 (2010); doi:10.5001/omj.2010.40
From the Department of Medicine, Sultan Qaboos University Hospital, Muscat, Sultanate of Oman.
Received:29 Dec 2009
Accepted: 07 Feb 2010
Address correspondence and reprint request to: Dr. Kowthar Hassan, Department of Medicine, Sultan Qaboos University Hospital, Muscat, Sultanate of Oman.
E-mail: kowhassan@btinternet.com
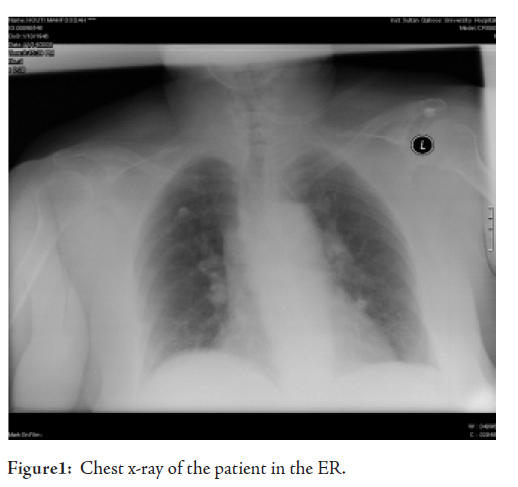
A 70 year-old hypertensive diabetic female from Muscat with a past medical history of a stroke since 9 years ago and is on lisinopril, frusemide and insulin was presented to the emergency room (ER) with dyspnoea which developed three days earlier together with cough and fever. She had attended a local health centre where she was prescribed amoxycillin and erythromycin for community acquired pneumonia. The fever and cough resolved after one day of antibiotic administration but the dyspnoea persisted. Arterial blood gases (ABGs) taken in ER showed a pH of 7.18, PaCO2: 59.9 mmHg, PaO2: 77.1 mmHg and a HCO3 of 18 mmol/L. She was started on 60% oxygen.
Her chest XR showed bibasal haziness assumed to be due to heart failure or community acquired pneumonia or a combination of both conditions since no BNP test was available to differentiate between the two conditions. In view of her previous CVA, her current dyspnoea and the CXR findings, a presumptive diagnosis of possible acute coronary syndrome (ACS) +/_ chest infection was made and she was started on co-amoxiclav, azithromycin, aspirin, clopidogrel, simvastatin, enoxaparin and beta blockers (BB). In addition, she received regular salbutamol nebulizers. Her ECG was not significant for ischaemia and her first troponin level was 0.15 which could have been due to slight renal impairment (creatinine 114). Indeed her second troponin was 0.13 mcg/L making the diagnois of ACS unlikely at this stage. Two hours later, her ABG were pH: 7.428, PaCO2: 36 mmHg, PaO2: 51.5 mmHg, HCO3: 24 mmol/L. The worsening PaO2 in spite of oxygen therapy was accompanied by a scattered wheeze.
The following day, the patient’s chest examination revealed inspiratory crepitations and a widespread wheeze. She desaturated to 84% on room air. An urgently requested spiral CT and D-dimers requested for a pulmonary embolism were normal. Ipratropium nebulizers and three times daily hydrocortisone 100mg were commenced but her condition remained unchanged and her oxygen saturation continued to drop to 85% within 10-15 min of stopping oxygen therapy. Immediately after nebulizer inhalation, her chest would be clear but a loud wheeze would return 10 minutes later.
What is the likely cause of her wheeze and desaturation?
a. pneumonia
b. heart failure
c. ACS
d. drug-induced
e. chronic bronchitis