
Fetus in Fetu: A Rare Presentation in an Adult Female
Akhtar Murtaza1, Chandak Kanhaiya1, Mahore Sadhna2, Maimoon Sabiha2
Murtaza A, et al. OMJ. 25, (2010); doi:10.5001/omj.2010.43
ABSTRACT
A case of fetus in fetu, a pathologic condition resulting from abnormal embryogenesis in a diamniotic, monochrionic pregnancy is reported. This condition usually presents in infancy and childhood. In this present case, a 30 year old patient misdiagnosed preoperatively as retroperitoneal dermoid is presented. This is the oldest patient reported with fetus in fetu in literature.
From 1Department of Surgery, N.K.P. Salve Institute of Medical Science and Research Centre, Digdoh Hills, Hingna Road, Nagpur, 2Department of Pathology, N.K.P. Salve Institute of Medical Science and Research Centre, Digdoh Hills, Hingna Road, Nagpu
Received: 27 Dec 2009
Accepted: 19 Jan 2010
Address of correspondence and reprint request to: Dr Murataza Akhtar, Professor and Head Department of Surgery,2A, Achraj Towers I,Y point, Chaoni, Nagpur 440013
E:mail: murtazaakhtar@indiatimes.com
Murtaza A, et al. OMJ. 25, (2010); doi:10.5001/omj.2010.43
INTRODUCTION
Fetus in Fetu is a fetiform calcified mass or an encapsulated pendunculated vertebral tumor.1,2 It is a malformed parasitic twin included in host twin due to unequal division of totipotent cells of a blastocyst, resulting in the inclusion of small cellular mass in a more mature embryo thus forming a monozygotic, diamniotic twin pregnancy.3 It is a rare condition which was first described by Meckel in the eighteenth century.4
A 30 year-old married female was admitted with a lump in the right side of the abdomen of 8 years duration. The lump was noticed immediately after pregnancy and it was gradually increasing in size. The patient had not conceived after the appearance of the lump. There were no gastrointestinal or genitourinary complaints. There was also no history of twinning or Teratoma in the family. A large 18cms x 15cms mass of firm consistency was palpable in the right hypochondriac and lumbar region.
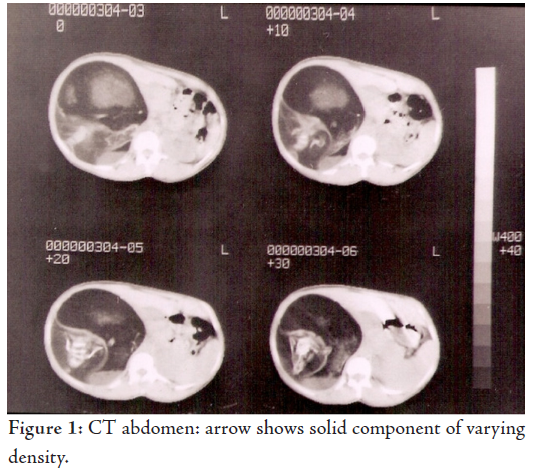
Conventional Radiography of the abdomen showed irregular radio dense lesion with calcification. Abdominal Ultrasound showed a cystic mass with mixed echogenecity. CT scan of the abdomen showed a cystic lesion with solid component of varying densities which was diagnosed as retroperitoneal dermoid. (Fig. 1)
Alpha Fetoprotein levels were normal. On exploration, there
was a well encapsulated mass occupying the right side of the
retroperitoneal space, extending from the under surface of the liver
reaching up to the pelvic rim. Apart from a network of vascularity
around the capsule, there was a vascular pedicle attached to the
tumor mass from the right renal artery. The mass was removed.
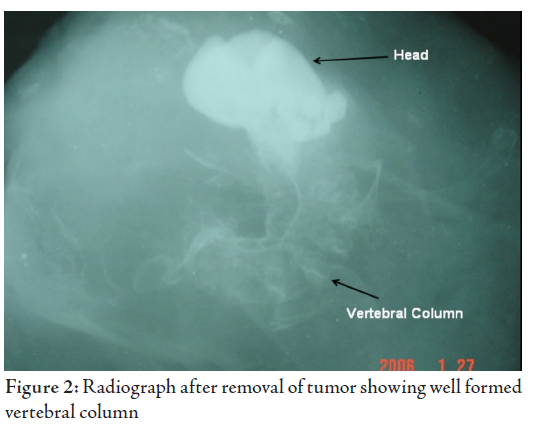
On examination, the tumor contained 2.5 litres of yellow colored
fluid and incomplete enencephalic fetus weighing 1.5 kgs covered with vernix caseosa. The radiograph of the specimen after removal
showed vertebral column, (Fig. 2).
Fetus in fetu is a rare condition occurring once in 500,000 deliveries.5 It is a parasitic monozygotic tumor predominantly found in neonates and children, with 89% cases presenting before the age of 18 months and only 3 cases reported after the age of 15 years. The oldest patient reported to date was 29 years old.6 The present case is of a 30 year old which is extremely rare and the oldest patient reported in literature to date.
Fetus in fetu presents as a lump in the abdomen (70%) and the retroperitoneal space is the commonest site (80%). Other rare sites include sacro-coccygeal region, intracranial, thorax, pelvis and the scrotum.7 Late presentation at the age of 30 years in the present case may be due to a dormant fetus which started growing under the influence of a host pregnancy. The role of radio diagnosis is undeniable and CT scan is the most reliable, showing fat collection around central bony structures.7 However, rarity of presentation at the age of 30 years lead to the pre-operative misdiagnosis of Retroperitoneal Dermoid.
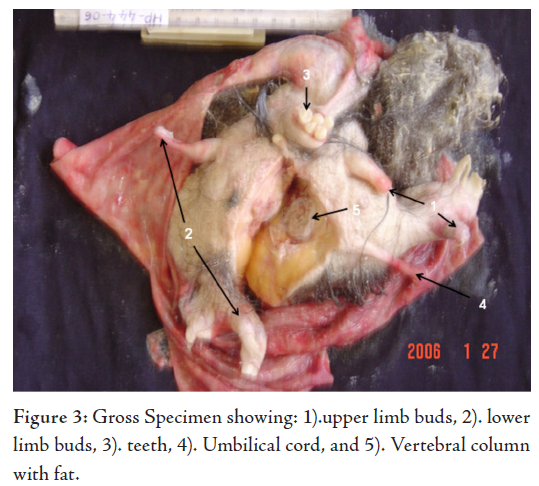
Single parasitic fetus is the commonest presentation (88%), multiple fetus ranging from 2-5 have also been reported. The present fetal size was 15 cm x 12 cm, the reported size varies between 4cm and 24 cm. The fetal weight varies between 1.2 kg and 1.8 kg, and it was 1.5 kg in this present case. The organs demonstrated are namely; spine in 91%, limbs in 82.5%, CNS in 55.8%, GIT in 45%, Vessels in 40% and GUT in 26.5% cases respectively.3 Visualization of the vertebral column and limbs on imaging, gross, and histopathological examination confirms the diagnosis. This fulfills the ?Willis criteria? which stresses much emphasis on the development of axial skeleton and vertebral axis.8
The majority of fetus in fetu present in early years of life and only three cases have been reported in patients over 15 years of age, the oldest being 29. This age factor was responsible for the misdiagnosing as Teratoma. There is a controversy whether a fetus in fetu is the distinct entity or a highly organized Teratoma. It is difficult to differentiate the two. Some authors claim that fetus in fetu is a well differentiated highly organized Teratoma, while others claim it to be a different pathological entity.9 Fetus in fetu occurs in upper the retroperitoneum while Teratoma occurs in the lower retroperitonium, pelvis, ovary and sacrocoocygeal regions.10 Malignant transformation is rare in fetus in fetu and only one case has been reported in literature.11
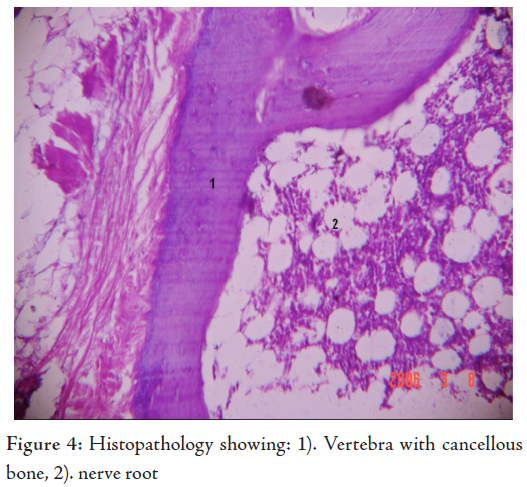
The presence of vertebral column is an important diagnostic criterion which suggests the development of a notochord which in turn is an advanced primitive streak stage.8 A non calcified vertebral column invisible on radiograph or on CT scan or its total absence (9%) does not exclude diagnosis of fetus in fetu.12
However, the presence of a bony vertebral axis with appropriate limb arrangement on gross is an important diagnostic feature which was observed in the studied case, thus confirming the diagnosis of fetus in fetu.13 Other differentiating features include normal levels of Alfa feto protein in fetus in fetu. A new diagnostic modality (molecular analysis) is using an informative genetic marker, for uniparental isodisomy of chromosomes 14 and 15, if it shows no genetic difference between the host and the Fetiform mass, then it is diagnostic of fetus in fetu.14
Fetus in fetu derives its blood supply from the rich vascular plexus around the cyst wall. Vascular pedicle is rare and usually observed in large growing masses with delayed presentation.15
Surgical excision is the treatment of choice in both Fetiform Teratoma and fetus in fetu. Under strict post surgical follow up, if recurrence occurs, the diagnosis could be revived to Fetiform Teratoma.
CONCLUSIONFetus in fetu is commonly seen in childhood. Presentation at the age of 31 years is very rare. Fetus in fetu should always be kept as differential diagnosis of retro peritoneal dermoid in adults.
The authors reported no conflict of interest and no funding was received on this work.
-
Hoefel CC, Quy K, Phan HT, Nghia Hick Jruong, Nguyen TS. Fetus in fetu: A case report and literature review. Pediatric 2000; 105(6):1335-1344.
-
Fetus in fetu from http//www.thefetus.net/ accessed 2000-09-09
-
Gurses N, Gurses N, Bernay F. Twin fetuses in fetu & a review of literature. Z Kindercher, 1990; 45:319-22.
-
Luzzatto C, Talenti E, Tregnahi A, Fabris S, Scapinello A, Guglielmi M. Double Fetus in fetu: diagnostic imaging. Paediatr Radiol.1994; 24:602-603
-
Grant P, Pearn JH. Foetus in foetu, Med J. Aust 1969; 1:1016 -1020
-
Massed MG, Kory L, Beneditti E, Ghorl RD, Geha AS, Abcarian H. Dysphagia caused by a fetus in fetu in a 29 year old man. Am.Thorac. Surg, 2001; 71(45):1338-1341.
-
Nagar A, Raut AA, Narlawar RS. Foetus in Fetu. J Postgrad Med 2002; 48:133-134.
-
Willis RA. The borderland of embryology and pathology 2nd ed. Washington DC: Butterworth, 1962; 442-462.
-
Potter EL. Pathology of the fetus and the newborn. In: Potter EL, ed. Pathology of the fetus and the newborn. 2nd ed. Chicago, Ill: Year Book, 1961; 183-187.
-
de Lagaurie P, de Napoli CS, Stempfli N, Truong QD, Vuillard E, Ferkadji L, et al. Highly differenciated Teratoma and fetus in fetu: a single pathology? J Pediatr Surg 1997; 32:115 -116 .
-
Hopkin KL, Dickson PK, Ball TI, Ricketts RR, O?Shea PA, Abramovosky CR. Fetus in fetu with malignant recurrence. J Pediatr Syrg 1997; 32:1476-1479.
-
Moorthy K, Rao PP, Deshpande AA, Thakur RK, Supe AN. Fetus in fetu or a retroperitoneal teratoma--a controversy revisited. A case report and review of literature. Indian J Cancer. 1997; 34(4):179-181.
-
Hsiao YC, Chen CC, Shih TY, Shih HS, Chen W, Wu NK. Fetus in fetu: report of a single case. Zhonghua Min Guo Xiao Er Ke Yi Xue Hui Za Zhi. 1993 Mar-Apr; 34(2):151-156.
-
Brand A, Alves MC, Saraiva C, Loio P, Goulao J, Malta J, et al. Fetus in Fetu- Diagnostic criteria and differential diagnosis -A case report and literature review. J Ped Surg. 2004 April; 39(4):616-618.
-
Patankar T, Fatterpekar GM, Prasad S, Mukharji SK. Fetus in fetu: CT appearance report. Radiology 2000; 214:735-737.